
Abstract
Introduction
Closed rupture of hand and wrist flexor tendons is not an uncommon clinical entity. 9 Established pathophysiological processes associated with this injury include inflammatory and infectious conditions, chronic overuse, and renal failure. 9 However, traumatic rupture due to bony injury occurs far less frequently.
Subacute rupture of the flexor tendons secondary to distal radius fractures is well documented.1-3,8,9,14,16,19,20,21,23,24 Conversely, occult flexor tendon rupture in the acute setting is rare. Reports of chronic tendon injury in conjunction with fractures of the distal radius describe patients treated with closed reduction who later presented with functional deficits.7,9,20,21,24 In recent years, accounts of flexor tendon rupture following open reduction internal fixation have been associated with volar plate fixation.1-3,8,14,16,19 However, discovery of acute traumatic flexor tendon rupture in the absence of significant physical examination abnormalities is not well described.
We present a case involving the incidental discovery of an acute, isolated flexor digitorum profundus (FDP) tendon laceration in order to emphasize the importance of thorough preoperative examination of displaced and comminuted fractures of the distal radius, as some patients may sustain tendon ruptures that will not manifest during initial global assessment of the hand.
Case Report
A 47-year-old right-hand-dominant male presented to our emergency department after sustaining multiple injuries in a motorcycle collision. Standard posterior-anterior, lateral, and oblique wrist radiographs revealed a comminuted 4-part fracture of the left distal radius with dorsal comminution and a volar lunate facet fragment (Figure 1a-1c).
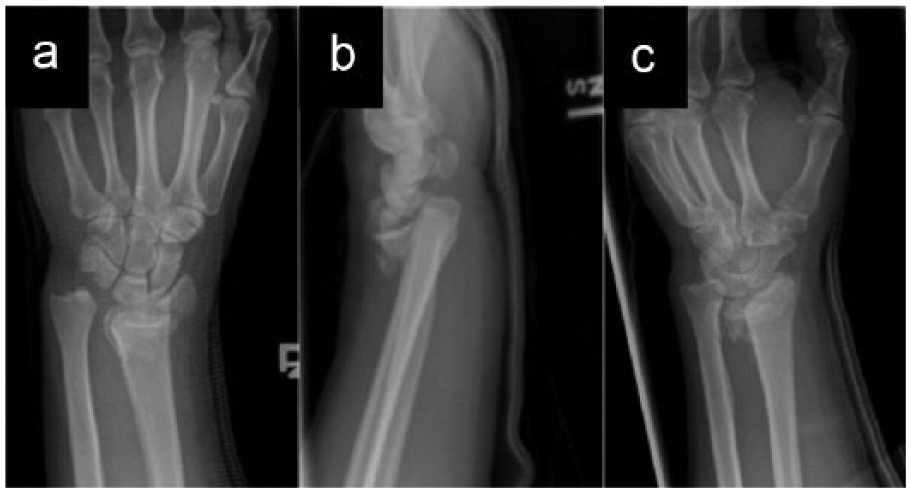
Plain radiographs of the left wrist at the time of initial presentation. a, Posterior-anterior view. b, Lateral view. c, Oblique view.
Standard serial physical examinations assessed pulses, sensation of light touch, and ability to perform the following tasks: extend the thumb at the interphalangeal joint, oppose the thumb and small finger, and cross the index and middle fingers. Sensation to light touch was normal in the median, ulnar, and radial nerve distributions. Closed reduction was performed and the patient was scheduled for operative stabilization.
On the fourth day of hospitalization, the patient underwent open reduction internal fixation of the distal radius fracture. Given the extensive dorsal comminution, shortening, and the presence of a lunate facet fragment, we performed a combined volar fragment-specific and dorsal spanning bridge plate fixation (Figure 2a-2c). The dorsal bridge plate was applied first. During the subsequent volar exposure, the FDP tendon to the index finger was noted to be lacerated at the level of the fracture site (Figure 3; see online Video S1). The pronator quadratus muscle belly was grossly intact, and there was no hematoma in the epitenon. No other structures were noted to be injured. The proximal and distal ends of the FDP tendon were marked, but repair of the severed tendon was deferred for several reasons. First, the severed FDP tendon was an unexpected finding and thus we had not consented the patient for its repair or reconstruction. We wished to have a discussion with the patient regarding his desires and functional demands. In addition, because the laceration was in flexor zone 5, it was unlikely the tendon would further retract, and we therefore felt a delayed repair or reconstruction would have little added morbidity compared with an intervention at the index procedure. Moreover, given the laceration was directly adjacent to the volar implant, there was concern that the tendon would glide directly over the plate, thus compromising the repair. Delayed primary repair was deemed the best option, and the patient was scheduled for subsequent removal of the bridge plate and volar fragment-specific hardware, with the plan to perform tendon repair or reconstruction in a delayed setting.
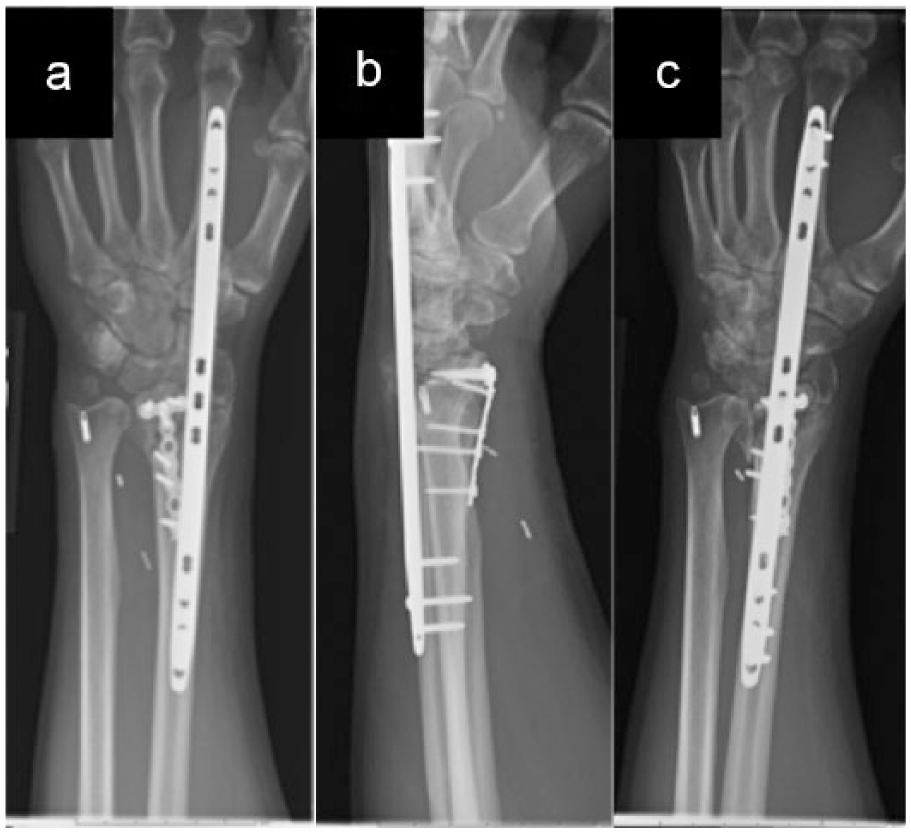
Plain radiographs of the left wrist following operative fixation. a, Posterior-anterior view. b, Lateral view. c, Oblique view.
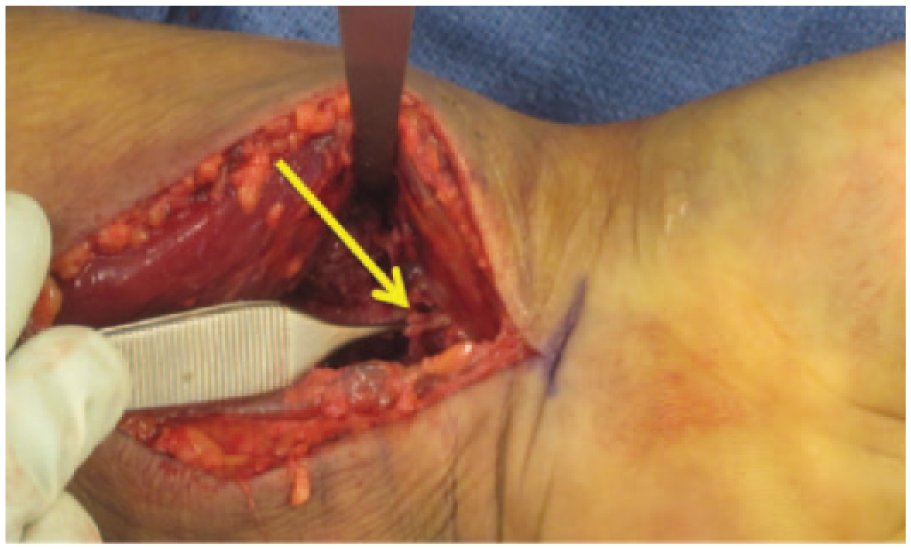
Photograph of the left wrist showing modified volar approach.
Discussion
Fractures of the distal radius are one of the most common injuries of the upper extremity, with an incidence that is steadily increasing.5,17 The flexor tendons of the wrist and hand—particularly those of FDP—lie in close proximity to the volar surface of the distal radius. Yet acute traumatic rupture of flexor tendons in association with distal radius fractures is remarkably rare.4,7,10,11 Several authors have postulated that the belly of the pronator quadratus muscle serves as a protective barrier between the sharp bony edges of the fracture site and the flexor tendons.15,20,25 For these reasons, flexor tendon rupture is often a minor consideration when evaluating patients with closed fractures of the distal radius.
Rupture of the FDP tendon to the index finger due to a distal radius fracture has been reported in 5 prior instances.7,9,20,21,24 In all of these cases, the patients were initially treated with closed reduction; surgical intervention was undertaken primarily to address functional deficits later noted on clinical examination. Southmayd et al described rupture of the flexor digitorum superficialis and profundus tendons to the index finger in a patient who presented shortly after closed reduction of a comminuted Colles fracture. 20 In the case presented by Cooney et al, the patient presented 3 months after the initial injury. 7 The remaining 3 cases involved delayed presentations, with injury to multiple tendons discovered at the time of surgery.9,21,24
In the first report of flexor tendon injury following a distal radius fracture, McMaster proposed 2 mechanisms to explain the pathologic processes that may be responsible. Bone fragments from the fracture site can cause fraying of the tendon, thus weakening its tensile properties and subsequently leading to mechanical failure under physiologic stress loads. Weakening of the tendon may also occur due to a disruption in blood supply secondary to direct pressure from bony callus or plaster casting. 15
However, McMaster’s discussion was limited to late attritional flexor tendon rupture, an injury that has subsequently been described by several authors.1-3,5,8,9,12,13,15,16,18,21,24 Over the past decade, volar plate fixation of operative distal radius fractures has become the common method of fixation. Flexor tendon rupture is a recognized complication related to distal and anterior placement of the volar plate.1-3,8,14,16,19
In contrast, acute tendon rupture presumably results from bone fragments at the fracture site. This patient sustained high-energy trauma that led to severe comminution of the distal radius. However, assessment of the global function of the injured hand did not reveal any loss of tendon function. Instead, the lacerated tendon was identified at the time of surgical exposure of the lunate facet. It is possible that the tendon laceration occurred during the initial traumatic event due to the high-energy injury. A more plausible scenario is that a sharp bony spicule from the fracture site lacerated the tendon. This could have occurred during the initial injury, closed reduction, postreduction digital range of motion exercises, or ligamentotaxis prior to dorsal spanning bridge plate fixation. Insertion of the bridge plate itself is an unlikely cause, as no screws were placed near the site of the laceration.
Although acute flexor tendon ruptures are not a common sequela of distal radius fractures, a high index of suspicion is warranted—especially in cases involving high-energy trauma. Due to pain and edema, patients may not always perform all maneuvers for a complete hand examination. As a result, subtle findings such as isolated FDP ruptures may be difficult to identify. Thus, the hand surgeon should be vigilant in examining flexor tendon function in the setting of acute high-energy injury.
Given the widespread use of volar plate fixation for distal radius fractures, attritional rupture of the flexor tendons due to hardware has become a recognized complication of surgical management. Unidentified acute ruptures can complicate the differentiation between iatrogenic injury, delayed attritional rupture, or a previously unidentified traumatic rupture.
Concurrent presentation of acute flexor tendon rupture and a distal radius fracture is challenging due to conflicting rehabilitation protocols. Although recent studies have advocated active mobilization of the digits within days after flexor tendon repair, 22 many providers still prefer to follow a passive range of motion protocol for 4 weeks postoperatively.
In this case, we used a dorsal bridge plate and a fragment-specific volar plate to stabilize the fracture (Figure 2a-2c). As the patient will be returning to the operating room for removal of the bridge plate and volar fragment-specific hardware, we plan to perform tendon transfers at the time of the second procedure.
In summary, flexor tendon rupture associated with fractures of the distal radius is a rare occurrence, with few reports published in the literature. Specifically, incidental discovery of an isolated FDP tendon rupture in the acute setting is not well described. We hope this case report will improve our knowledge of the mechanisms of flexor tendon injury in the setting of distal radius fractures requiring operative fixation. Due to the potential implications of a missed tendon rupture, careful examination of the flexor tendons should be included in the preoperative examination of distal radius fractures, especially those with a high-energy mechanism of injury.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study did not involve treatments or procedures performed, or medications administered, for research purposes. All proceedings were performed in accordance with national and institutional ethical standards. No patient identifying information has been included in the article.
Statement of Informed Consent
The patient in this report was informed that data concerning his case would be submitted for publication, and he provided consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Video S1 is available in the online supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.