
Abstract
Keywords
Introduction
The treatment of suppurative flexor tenosynovitis (SFT) requires prompt surgical intervention. 10 Failure to do so can result in significant patient morbidity due to scarring within the flexor sheath, stiffness, and persistent infection. 21 Surgical techniques used to treat SFT include open drainage (OD) and debridement or closed catheter irrigation (CCI). Traditionally, the OD technique was associated with poor clinical outcomes secondary to the wide surgical exposure of the affected flexor tendon/sheath complex.6-8,13 The patients in these early studies had a high risk of postoperative pain, stiffness, and wound breakdown.13,20 These high complications led to the development of less invasive techniques. Although first described by Dickson-Wright 5 (utilizing a ureteric catheter), and later refined by Unonius 22 (smaller incisions for sheath exposure and irrigation with a needle) and Carter et al 2 (performed through small incision proximal to A1 pulley with distal counter incision for egress of fluid), 22 Neviaser et al 16 described successful treatment of 20 patients with a limited tendon irrigation approach without postoperative sequelae.2,5,16 Subsequently, numerous other studies and methods regarding CCI have shown excellent results with these less invasive techniques.1,2,11,12,14,15,18,19
Although relatively minimally invasive surgical treatment of SFT has shown promising results, there is a paucity of literature comparing the 2 most common techniques, OD and CCI. Furthermore, while other studies have examined prognostic factors associated with outcomes after treatment of SFT, none have investigated the specific differences between the 2 techniques regarding pain, function, complications, and overall success in eradicating infection.
The purpose of this study was to compare OD versus CCI for treatment of SFT. Specifically, we sought to report on differences in the 2 methods with respect to pain scores, functional outcomes, need for reoperation, and influence of smoking and co-morbidities, in conjunction with analyzing culture and antibiotic data. Secondarily, we report on other prognostic variables associated with outcomes.
Methods
After obtaining institutional review board approval, a retrospective study was conducted analyzing the outcomes of all patients who underwent surgical treatment for SFT between the years of 2003 and 2011. The OD group was defined as those patients who underwent exposure of the flexor tendon sheath through a single incision (a volar Bruner incision or a mid-axial incision), with maintenance of the pulleys for debridement (Figures 1a and 1b). The CCI group included patients who underwent limited open incisions proximal to the A1 pulley and distal to the A4, with concomitant irrigation through a tunneled catheter until all purulent material was cleared from within the sheath (Figure 2). Continued irrigation of the flexor sheath was not conducted postoperatively. The surgeries were performed by 10 different consultant surgeons, adhering to the principles of either OD or CCI. Information pertaining to patient demographics, time from presentation to surgery, mechanism/cause of infection, physical examination, tobacco use, medical comorbidities (eg, diabetes, peripheral vascular disease, liver/renal disease), pre- and postsurgical care, antibiotic usage, and culture and laboratory results were obtained.
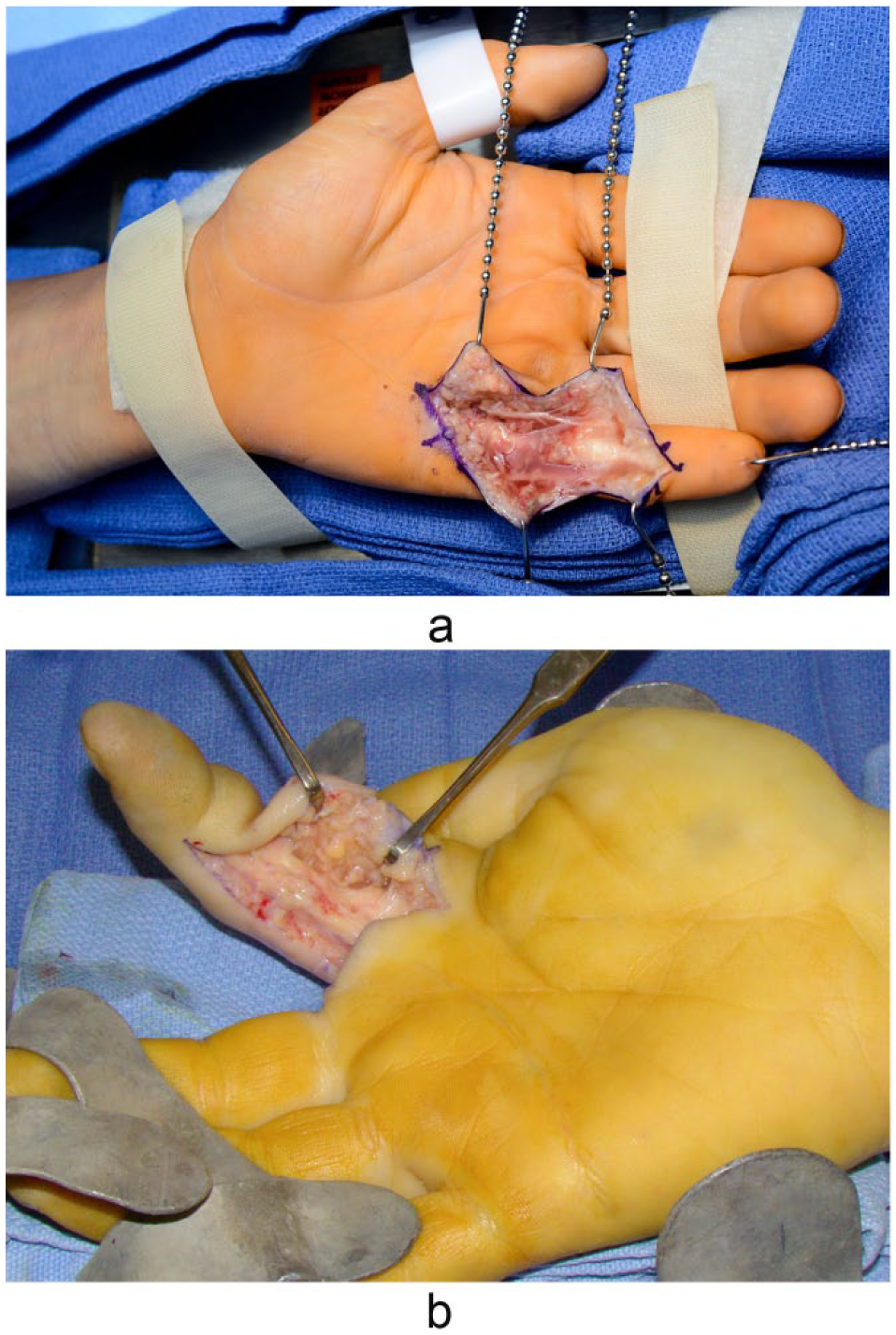
Examples of Bruner (a) and midlateral (b) incisions used for open drainage of suppurative flexor tenosynovitis.

Example of catheter irrigation system.
Exclusion criteria included cases not isolated solely to the flexor tendon sheaths (eg, infections spreading to the deep palmar spaces) and patients who had undergone prior treatment of an infection in the digit not related to the flexor sheath. We included patients who had culture-negative SFT but demonstrated purulence at the time of surgery.
The type and length of antibiotic treatment was guided by the infectious disease (ID) service at the hospital, based on pre- and intraoperative culture results, and chosen per specific ID consultants’ preferred regimen(s). Appropriate splinting in the safe intrinsic position during the initial recovery phases to prevent contracture, elevation of the extremity, early range of motion exercises were initiated immediately postoperatively with the assistance of occupational therapy (OT) as deemed necessary by the treating surgeon. Further OT in the outpatient setting consisted of active and passive range of motion exercises and edema control for all patients, with further wound care measures (eg, ultrasound mist therapy) being provided for a number of the patients. Pain scores, function as per Mayo wrist score (MWS) and Cleveland outcome grade, complications, reoperations, and successful treatment of infection were analyzed. The Cleveland grades, while not validated, were chosen based on them being an objective assessment of functional outcome and their specificity to flexor tenosynovitis analysis.3,8
Statistical Analysis
The primary comparison between OD and CCI for SFT included analyzing pain, range of motion, complications, reoperations, eradication of infection, and functional outcomes, including MWS and Cleveland outcome score, and it was our hypothesis that there would be no detectable clinical difference between OD and CCI, when examining the above-mentioned parameters. Similarly, we also examined the effect of patient-related factors on these outcomes. Our hypothesis was that certain factors, such as smoking, comorbidities, time to receiving antibiotics, and time to surgery, would result in detectable differences in clinical outcomes for patients undergoing surgical treatment of SFT. Univariate Cox proportional hazards models were used to describe the relationships of these outcomes with multiple confounding variables, including demographics, comorbidities, time to surgery or antibiotics, postoperative therapy, duration of hospitalization or antibiotics, and culture results. Descriptive statistics were used to summarize the data and outcomes measures. We utilized univariate regression analysis to describe the associations between outcomes and preoperative, therapeutic, or surgical variables. Nominal variables were compared with contingency analyses using chi-square tests and analysis of variance (ANOVA) regression. Continuous and nominal variables were compared using the student’s 2-tailed unequal variance t tests. All analyses were carried out using the JMP statistical software package (Version 8; SAS Institute Inc, Cary, North Carolina). Statistical significance included a P value < .05.
Results
Twenty-four patients were treated for SFT over the 8-year period, at an average follow-up of 3 ± 2 years. Patient demographics including their smoking history are summarized (Table 1). As for diagnostic factors, all 4 Kanavel signs were present in 17 (71%) patients, with no statistical differences between the groups as far as severity of cases per these physical exam findings. Etiologies underlying the SFT infection were quite variable, including animal bites, foreign objects, and other traumatic injuries. Only 2 of the patients could not recall any inciting event preceding the development of their tenosynovitis symptoms. Eighteen patients had positive culture results, including 11 (46%) Staphylococcus aureus (1 case of Methicillin-Resistant S aureus [MRSA]), 6 (25%) beta-hemolytic streptococcus, and 5 polymicrobial cases. Six of the patients demonstrated no growth from their intraoperative cultures, despite possessing gross intraoperative purulence and clinical symptomatology consistent with SFT. All of these 6 patients received preoperative antibiotics. Gross purulence was present in 22 (92%) patients (Table 2). None of patients in this study experienced recurrent SFT or osteomyelitis.
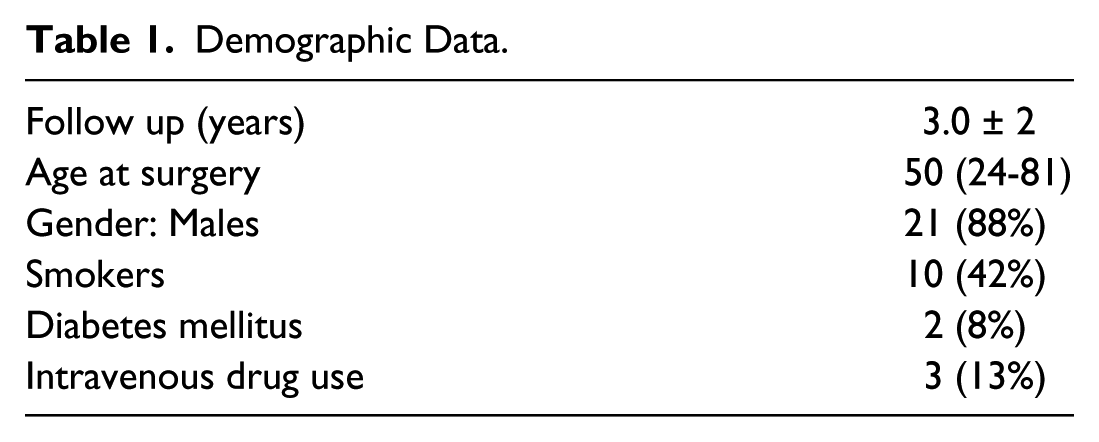
Demographic Data.
Diagnostic Factors.
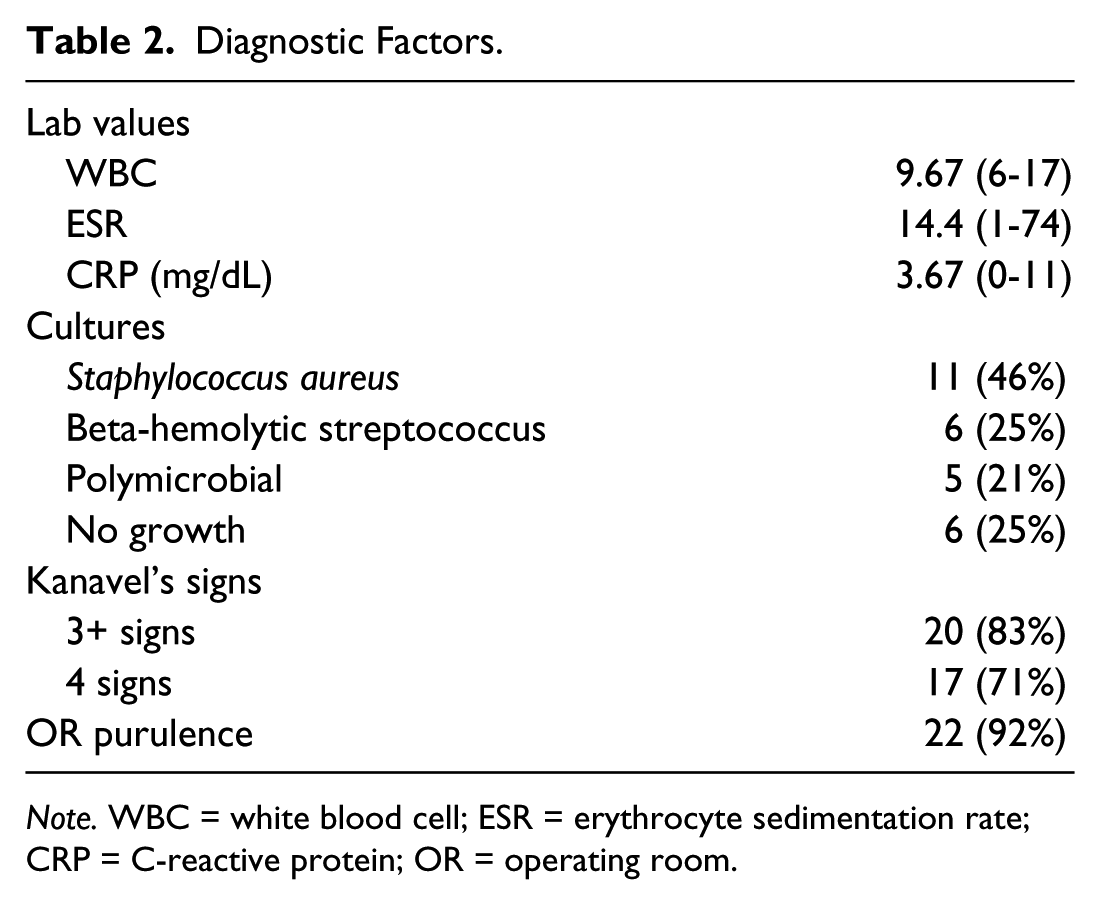
Note. WBC = white blood cell; ESR = erythrocyte sedimentation rate; CRP = C-reactive protein; OR = operating room.
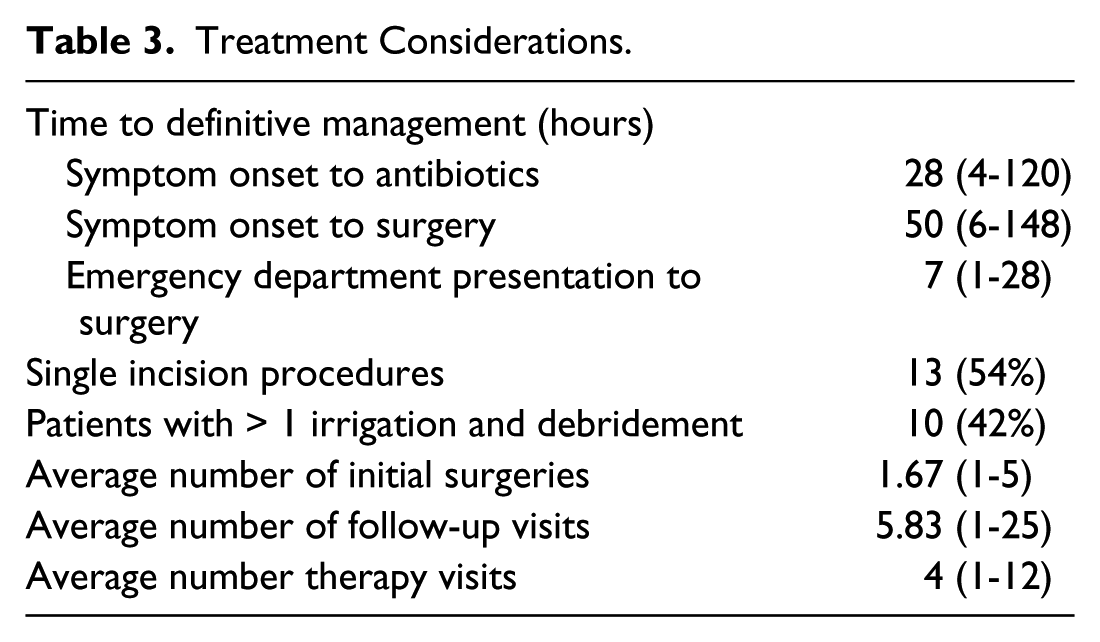
As for treatment, details regarding time to antibiotics and eventual surgery, number of irrigations and debridements performed, and follow-up/OT visit totals were evaluated (Table 3). On average, patients were hospitalized for 4 days (range: 0-8 days) and received 23 days (range: 8-47 days) of antibiotics. Although 10 (42%) of our patients had a planned return to the operating room during their initial postoperative care period (in the form of repeat washout and delayed closure), only one patient required an unplanned additional irrigation and debridement.
Treatment Considerations.
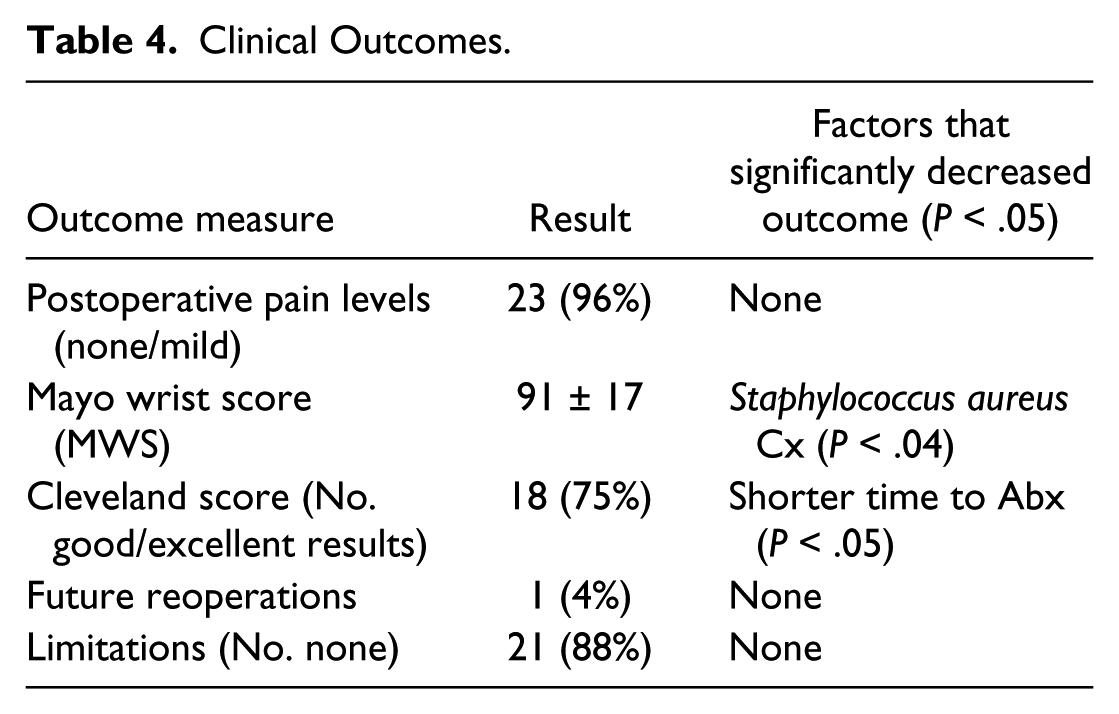
Most of the patients experienced a good recovery from their SFT infections. Twenty-three of 24 patients experienced none/mild pain at latest follow-up, with the average MWS of 91 ± 17. Based on Cleveland criteria, 2 (8%) had poor results, 4 (17%) had fair results, and 17 (71%) had good/excellent results. Only 5 patients reported any kind of postoperative stiffness, without any other limitations in activities of daily living or work. Although there were no variables that had a significant impact on postoperative pain scores, future reoperations, or limitations, the final MWS was negatively affected by a positive S aureus culture result, and the Cleveland outcome grade positively correlated with a shorter time to receiving antibiotics (P < .05) (Table 4).
Clinical Outcomes.
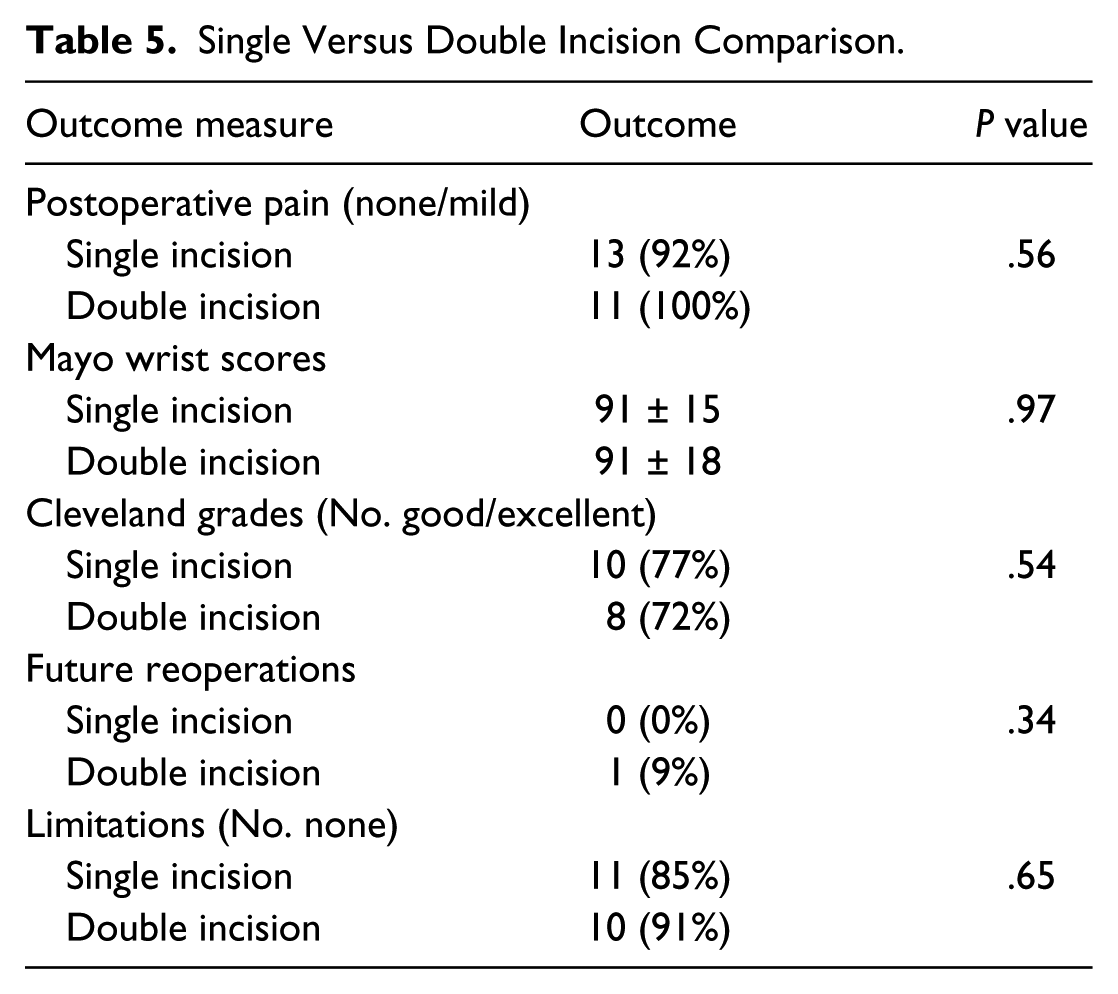
In comparing OD and CCI, there were no statistical differences with respect to age, gender, or medical co-morbidities between the groups. The OD group consisted of 13 patients (13 men and 0 women) with a mean age of 49.2 years. There were 8 smokers and 3 with significant co-morbidities in this group. Mean length of hospitalization was 3.8 days (range: 2-6 days), and duration of antibiotics was 27.5 days (range: 14-47 days). The CCI group consisted of 11 patients (8 men and 3 women) with mean age of 50.3 years. There were 2 smokers and 3 with significant co-morbidities in this group. Mean length of hospitalization was 4.8 days (range: 0-8 days), and use of antibiotics was 18.1 days (range: 8-26 days). There was no evidence of any flap necrosis, be that via an open Brunner incision or mid-axial approach. Average follow-up, total number of follow-up visits, and number of OT visits did not significantly differ between the 2 groups. With regard to pain, MWSs, Cleveland grades, need for unplanned reoperations, and limitations in activities of daily life, there were no statistically significant differences between the OD and CCI groups (Table 5). Patients who smoked required on average 10.8 more days of antibiotics than nonsmokers (29.5 vs 18.7 days for nonsmokers), but this was not statistically significant. Time to surgery, even when focusing on differences between those who underwent surgery more acutely than those who were treated even 12 to more than 24 hours from presentation to our emergency department (ED), did not correlate at all with pain, functional outcomes, limitations, eradication of infection, or need for reoperation.
Single Versus Double Incision Comparison.
Discussion
Surgical treatment of SFT has been well reported, with the role of CCI showing promising results in numerous studies.2,11,12,15,18,19 With perceived benefits over OD of quicker return to function and smaller wounds with less scarring, much of the recent literature regarding surgical treatment of purulent flexor tenosynovitis has focused on CCI. To our knowledge, only 2 other studies have directly compared CCI with OD.4,9 Gutowski et al compared 32 patients who underwent OD with 15 who underwent CCI for SFT. Of the 17 (35%) patients who had documented follow-up in the outpatient clinic, the CCI group appeared to have fewer complications and required less reoperations, despite neither reaching statistical significance. Overall, the authors concluded that there was no difference in postoperative outcomes between the 2 groups, acknowledging their results were significantly affected by their high loss to follow-up. Our results are similar to Gutowski et al. In the other study, Dailiana et al found early diagnosis with drainage through smaller incisions and continuous postoperative irrigation to result in the best functional outcomes. Per their results, a negative influence on outcomes with a delay in treatment was seen in those patients who underwent OD through a Bruner incision, and this trend was even more pronounced with follow-up exceeding 12 weeks. In contrast to the findings of Dailiana et al, as previously mentioned, we did not find any significant differences between the 2 techniques in the outcome measures examined in our series. In addition, we did not find any flap necrosis difference between those who had a Brunner versus mid-axial incision within the OD group.
Multiple studies have examined the prognostic factors associated with clinical outcomes after surgical treatment of SFT.4,13,17 Pang et al analyzed factors affecting the prognosis of SFT in 75 patients who underwent either open or closed treatment. 17 They demonstrated that age >43 years, comorbidities, presence of subcutaneous purulence, digital ischemia, and polymicrobial infections correlate negatively with outcome. They did not find that time to definitive management affected clinical outcomes. Furthermore, this study did not directly comment on any differences between OD and CCI. Maloon et al examined the clinical outcomes of 42 patients with SFT who underwent OD alone. 13 Overall, 38% had good functional results at last follow-up. They found diabetes mellitus, human bites, and presentation beyond 7 days to be poorly correlated with overall outcomes. Within our study, we had fair or good functional and clinical results in 22 of 24 patients (92%). Furthermore, while we did not find comorbidities affected overall outcomes, patients with S aureus cultures had a worse overall outcome in follow-up. However, we do feel that subcutaneous purulence and digital ischemia are important considerations when considering OD.
There are several limitations in this study secondary to the nature of SFT and the ability to analyze its long-term treatment outcomes. First, this is a retrospective review with treatment regimens determined per the discretion of the surgeons and consulting ID services managing the patients. An improvement would be a prospective study for which we plan to do in the future, comparing the 2 treatment methods. Another limitation is the number of different surgeons within our study, and the inherent differences in their description of purulence and surgical technique including volume of fluid used during CCI, planned reoperations, or postoperative treatment protocols. However, this also could be considered an advantage of our study, as it helps to demonstrate that despite multiple potential confounding factors, the patients do very well in the long-term when undergoing either OD or CCI combined with multiple postoperative regimens. Unlike many previous studies, we not only were able to directly compare OD and CCI in long-term follow-up period, but we also analyzed multiple other variables which had the potential to affect the success of treatment for SFT. With 8 out of the 10 smokers in our study undergoing OD, this likely may explain why the OD group, while not approaching statistical significance, required on average a longer duration of antibiotics. Some treatment bias to perform OD in smokers may have existed in this study, but once again, the clinical outcomes of the OD group were similar to that of the CCI group despite this, which simply strengthens the argument for it being a reasonable treatment option for patients with SFT.
In summary, although SFT is a very common surgical emergency, there is a paucity of information regarding the different factors and treatment regimens that influence the outcomes. We found that surgical treatment of SFT with either OD or CCI resulted in good pain relief, functional outcomes, and eradication or infection. There were no differences between the surgical techniques. Factors that negatively influenced outcomes include S aureus culture, prolonged time to antibiotics, and smoking. Time from presentation to our ED to the operating room did not impact overall outcomes. We therefore recommend surgeons to utilize the technique and therapeutic approach they feel most comfortable with when treating SFT. We did not specifically analyze subcutaneous purulence or digital ischemia, but do feel those are important considerations for surgeons to consider. However, if a patient is to undergo CCI, our series demonstrates postoperative indwelling catheter irrigation is potentially not necessary. Antibiotics should be given immediately after cultures have been obtained. Based on our results, surgical management is required in an urgent rather than emergent fashion, in contradiction to previous studies.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kakar is a Consultant for Arthrex, Skeletal Dynamics, and AM Surgical. Drs. Born and Wagner have no commercial interests to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.