
Abstract
Introduction
Historically, failed conservative treatment for irreparable distal radioulnar joint (DRUJ) damage has been treated with distal ulna resection or DRUJ fusion.11,17 Such procedures include the Darrach, Sauvé-Kapandji, distal ulna hemiresection interposition, matched distal ulnar resection, and various arthroplasties.5,15 In many cases, distal ulna ablations show favorable results for initially decreased pain, improved motion, and improved grip strength but generate DRUJ destabilization and pathological motion. 1 Postresectional forearm instability can be 3 dimensional, but the most disabling is usually the radioulnar convergence phenomenon (ulnar impingement) seen during activities demanding weight lifting and gripping.1,9,11,25 The unsupported distal radius can collapse against the ulnar stump when even a small load is applied. 12
Treatment of painful radioulnar impingement is extremely difficult. Several management options are described including soft tissue stabilization,3,22,24 ulna lengthening, further ulnar shortening, distal ulna replacement, and last resort techniques such as wide ulnar resection or creation of a single-bone forearm.16,20 Soft tissue stabilizing procedures are unpredictable and do not reliably prevent recurrent impingement. 25
One such procedure described for treating distal radioulnar instability following failed distal ulna resection is interposition of an Achilles tendon allograft between the distal radius and the ulnar stump, described by Sotereanos et al.9,16,22,23 Although favorable results have been published,9,16,23 this technique does not completely resolve the problem of painful radioulnar convergence, as the patients of this study, all of whom received an Achilles allograft interposition, showed recurrence of their symptoms. Radioulnar impingement is a difficult problem, but while published results for this allograft technique show favorable pain relief by visual analog scale (VAS) and improvement in both forearm rotation and grip strength,9,16,22,23 the complications and failures have not to date been adequately described in the literature.
Another option to stabilize the DRUJ, the Aptis DRUJ prosthesis, also known as the “Scheker prosthesis” (Aptis Medical LLC, Glenview, Kentucky), is a semiconstrained ball-and-socket joint replacing both the radial and ulnar components of the DRUJ. 15
Based on our experience, we hypothesized that (1) Achilles tendon allograft interposition arthroplasty does not adequately stabilize the forearm nor prevent painful dynamic radioulnar convergence and (2) Aptis total DRUJ prosthesis could correct these deficiencies. We describe our experience treating painful instability following failed Achilles tendon allograft interposition arthroplasty.
Materials and Methods
Patient Series
In 3 different institutions, we retrospectively reviewed all patients with ulnar head excision treated with Achilles tendon allograft interposition arthroplasty that failed (see Figure 1) and subsequently required a total DRUJ implant arthroplasty.
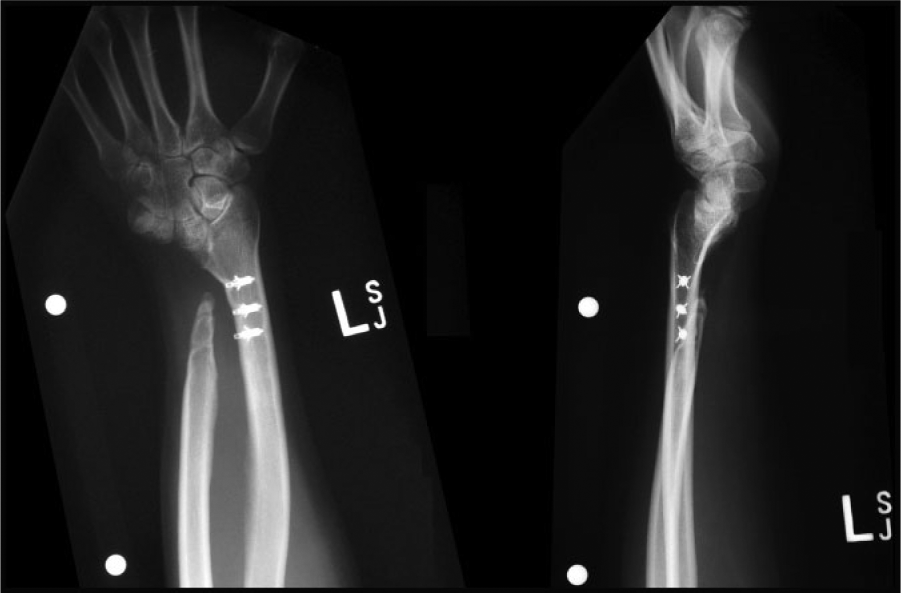
X-ray studies following Achilles tendon allograft interposition arthroplasty procedure.
Despite the Achilles allograft interposition, these patients experienced disabling pain due to recurrent clicking and locking around the distal forearm proximal to where the DRUJ was, from recurrent radioulnar impingement that interfered with daily activities. The pain was more pronounced with activities requiring weight bearing and/or forearm rotation. Patients felt significantly disabled for their usual level of activity.
Seven patients were included: 5 females and 2 males (see Table 1 for patient demographics). The right hand was involved in 4 cases and left in 3 cases. The dominant hand was affected in 3 cases. Two patients were initially diagnosed with bilateral Madelung’s disease.
Summary of Patient Cases and Demographics.
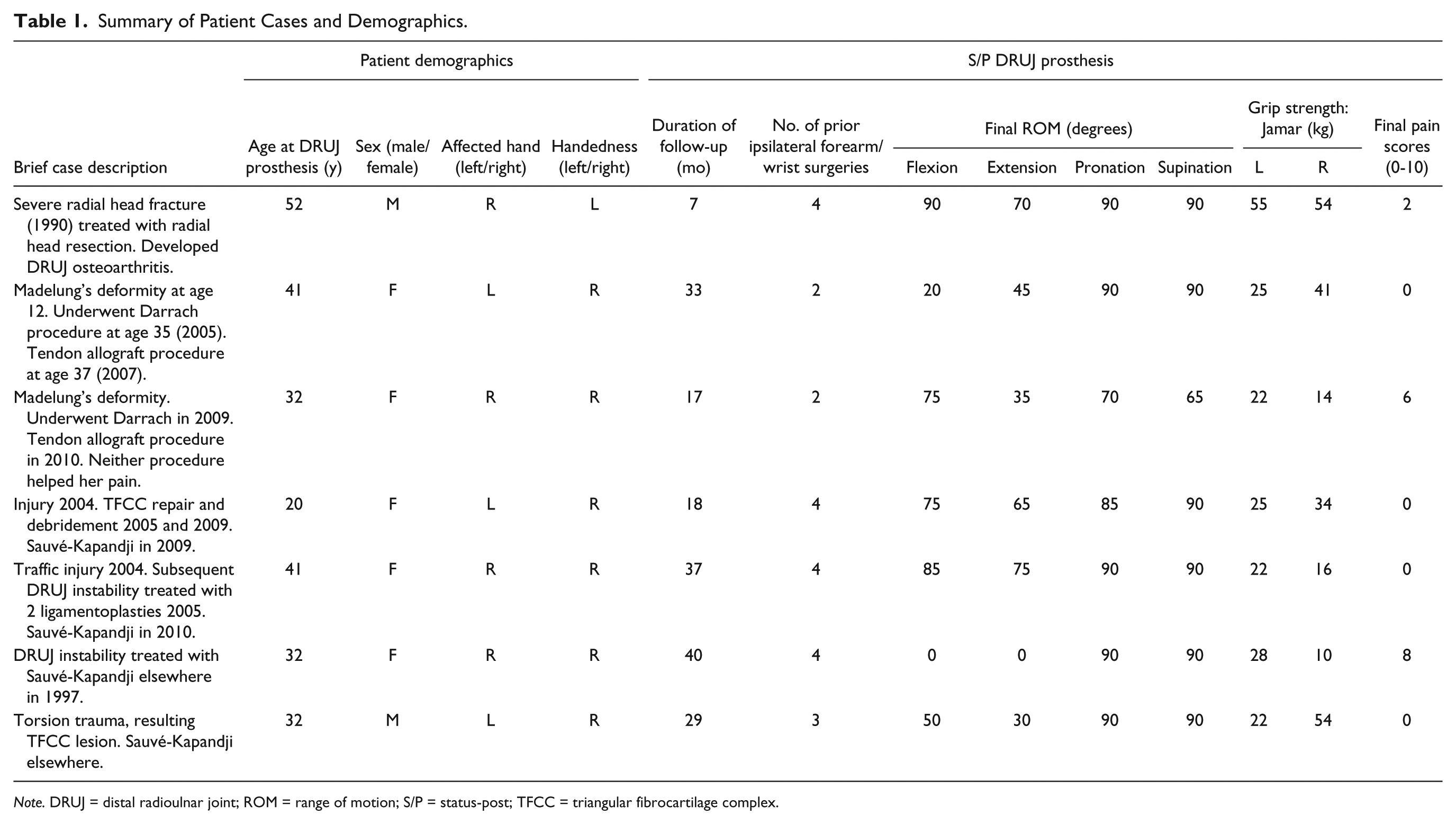
Note. DRUJ = distal radioulnar joint; ROM = range of motion; S/P = status-post; TFCC = triangular fibrocartilage complex.
Recurrent radioulnar impingement pain was noted to return in these patients within a few months of the Achilles tendon allograft interposition surgery (average of 5 months in this study). Static radioulnar impingement on standard posteroanterior radiographs, or dynamic impingement on weight-bearing cross-table posteroanterior radiographs, helped confirm this diagnosis.
After the Achilles allograft procedure was confirmed to have failed, these patients underwent revision to total DRUJ prosthesis. Average age at the time of revision surgery (conversion to the DRUJ prosthesis) was 36 years (range, 20-52 years). Prior to the prosthesis, these patients had already undergone several previous surgeries, with an average of 3.3 operations. Mean follow-up after the DRUJ prosthesis was 25.9 months (range, 7-40 months).
Of note, one of our surgeons has performed 8 allograft tendon interposition DRUJ salvage procedures, of which 4 experienced recurrent impingement and failed (50%). These cases subsequently required total DRUJ replacement (3 patients) or creation of a single-bone forearm (1 patient who preferred this salvage option vs total DRUJ arthroplasty).
Surgical Technique
Aptis DRUJ prosthesis is a modular implant comprising a radial plate, an ulnar stem, an ultra-high-molecular-weight polyethylene ball, a radial plate cover, and 2 radial plate cover screws. The procedure is usually accomplished under axillary block, antibiotic prophylaxis, and tourniquet control. Implant sizing is determined from scaled preoperative x-ray films (see Figure 2). The Aptis implantation technique used here has been well described in the literature.17-19
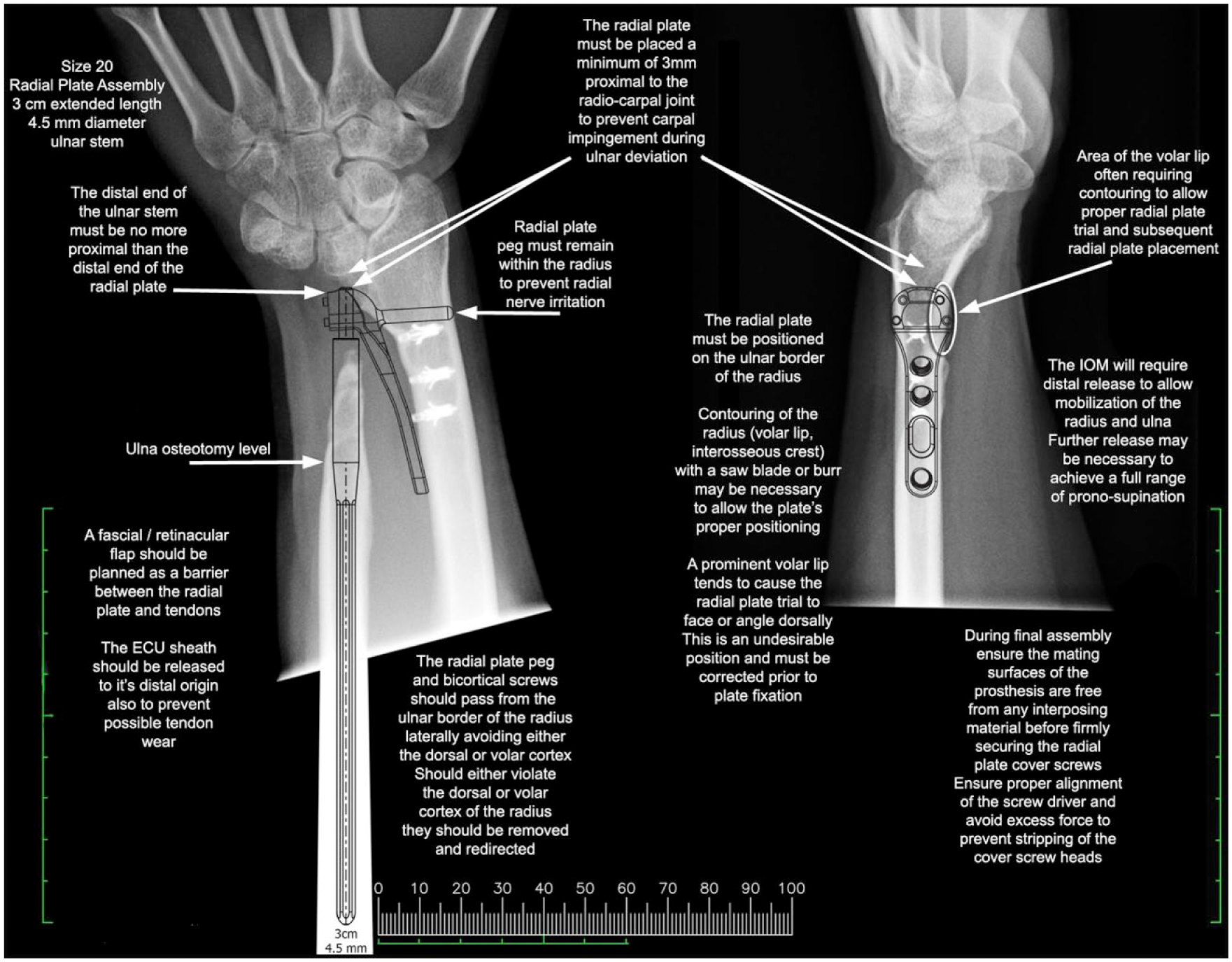
Preoperative customized template for total DRUJ arthroplasty operative planning.
The standard technique was modified to accommodate the incision to the presence of previous scars. The Achilles tendon allograft was identified and dissected prior to resection (Figures 3 and 4). Suture anchors were removed if accessible; we attempted to avoid further damage if they were not identified. Radial plate placement after allograft excision is depicted in Figure 5. Polyethylene ball placement and radial-ulnar component coaptation using the socket cover are depicted in Figures 6 and 7. Final x-ray studies confirm and document implant positioning (Figure 8); as evidenced here, the suture anchors are not always amenable to removal.

Exposure of Achilles tendon allograft.
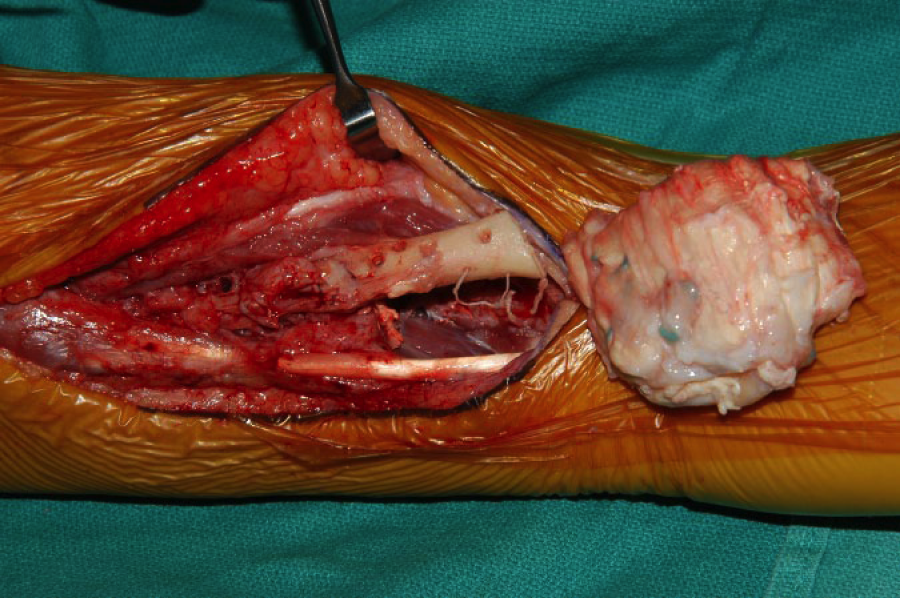
Resection of Achilles tendon allograft.
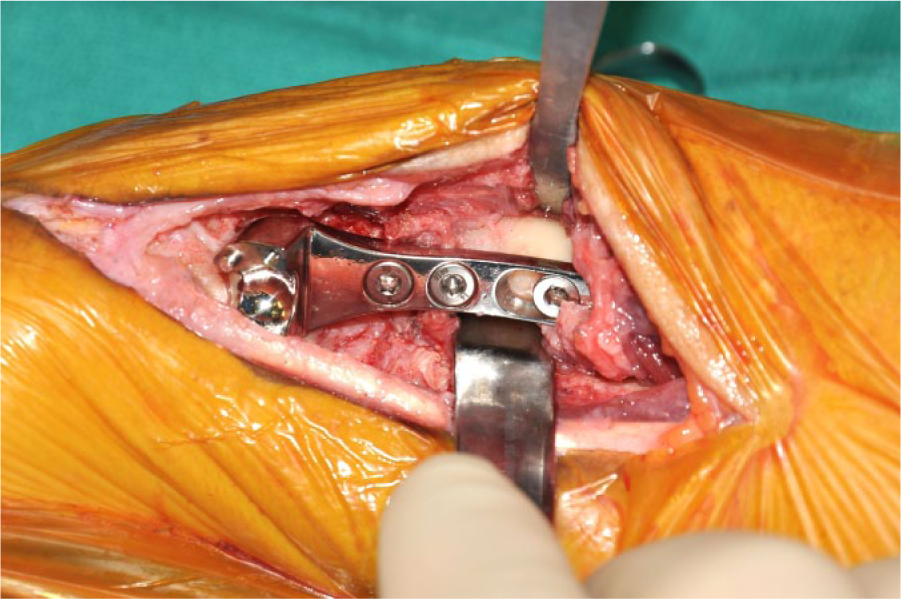
Radial plate in place.
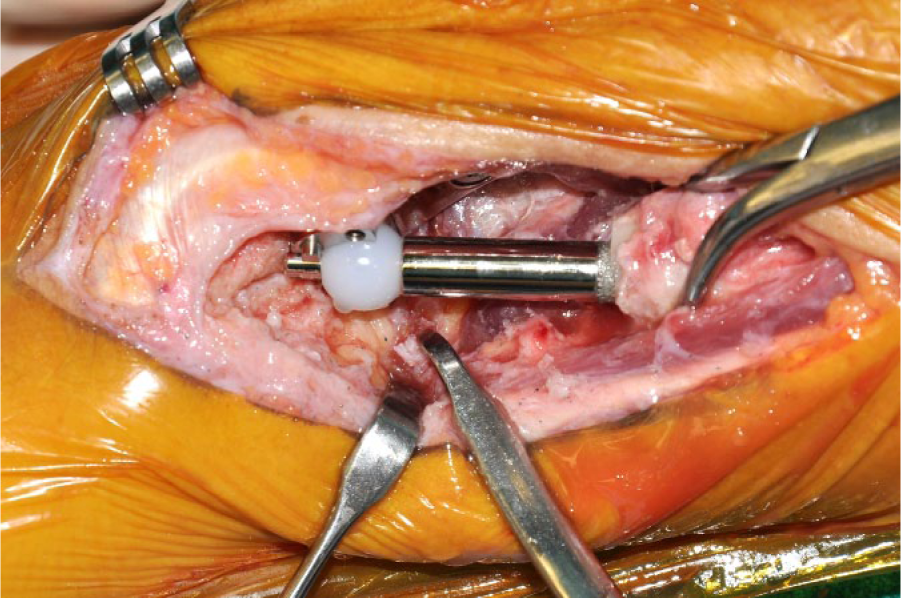
Ulnar component and polyethylene ball in place.
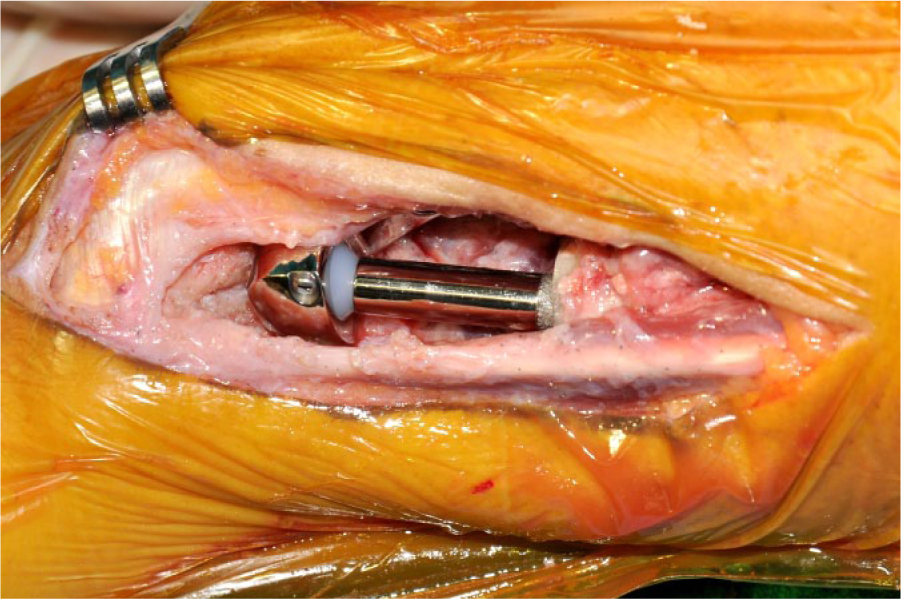
Socket cover in place constraining the implant.

Final x-ray study.
Later in the study, the implantation technique evolved to include harvest of an ulnarly based fascioretinacular flap during extensor tendon exposure. This flap is interposed between the prosthesis and the extensor tendons to prevent risk of subsequent extensor carpi ulnaris (ECU) tendonitis.
A soft dressing was applied for 2 weeks, allowing active range of motion immediately after surgery, once the regional block wore off. We use this protocol in with patients with extensive scar to prevent early contracture.
Follow-up
All patients were evaluated with the standardized protocol for DRUJ replacement both before and after surgery.
The DRUJ questionnaire comprises demographic information; previous procedures; Patient Rated Wrist Evaluation (PRWE) and Disabilities of the Arm, Shoulder and Hand (DASH) questionnaires; and postoperative satisfaction questions (in the postoperative follow-ups). Patient satisfaction with the procedure was assessed with direct questions and using an analog scale ranging from 0 (not satisfied at all) to 10 (completely satisfied). Clinic evaluation at each visit included pain measurement using a 10-point VAS, range of motion including the contralateral wrist, DRUJ stability, grip strength, and lifting capacity. Grip strength was measured in both hands using a Jamar II dynamometer (Sammons Preston, Inc, Bolingbrook, Illinois). Lifting capacity was measured in both upper extremities with the shoulder in neutral position and elbow flexed at 90°. The patient was asked to lift increasingly heavy dumbbells against gravity (2.3 kg [5 lb], 4.5 kg [10 lb], 6.8 kg [15 lb], and 9.1 kg [20 lb]), and posteroanterior and lateral x-ray views were obtained. Preoperative and postoperative values were recorded for comparison.
Results
Each patient presented with a markedly painful extremity after failed Achilles allograft arthroplasty (Table 2).
Summary of Patient Functional Scores, Prior Surgical Procedures, and Follow-up.
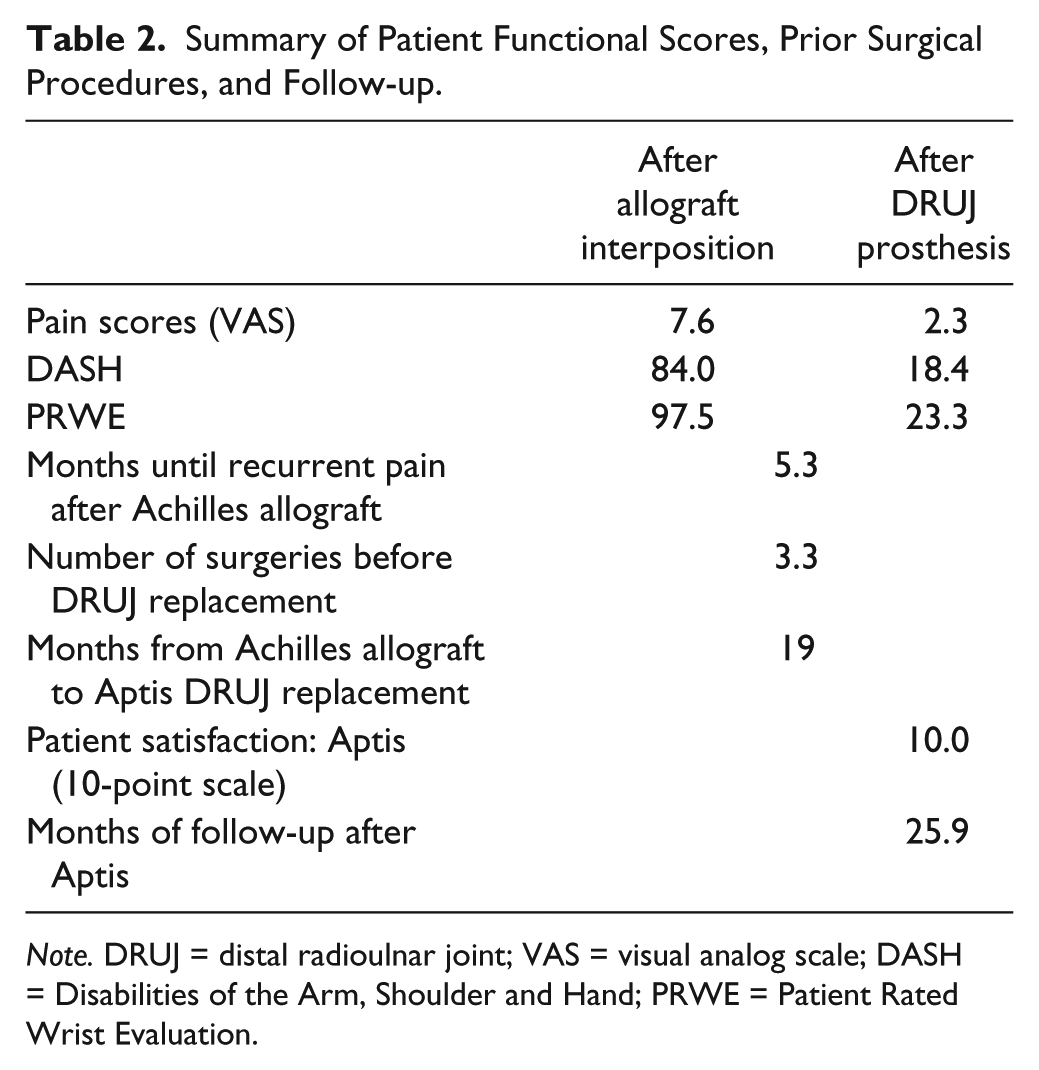
Note. DRUJ = distal radioulnar joint; VAS = visual analog scale; DASH = Disabilities of the Arm, Shoulder and Hand; PRWE = Patient Rated Wrist Evaluation.
After conversion to the Aptis DRUJ prosthesis, the pain, DASH, and PRWE scores all improved as shown in Table 2. After a mean follow-up of greater than 2 years (including 3 patients with less than that), no patient required implant removal. The mean range of motion improved although it was not the principal complaint of the patients (Table 3). Pain was relieved significantly as per VAS scores; DASH and PRWE scores also showed improvement in patients’ status (Table 2). Patient satisfaction was not recorded at all sites, but all that were surveyed rated their satisfaction as 10/10 at the latest follow-up after total DRUJ replacement. All of the patients stated that they would recommend this surgery to another patient and that they would request this prosthesis in the other wrist as a primary surgery if it sustained a similar injury (rather than trying the other procedures again).
Range of Motion (in Degrees).
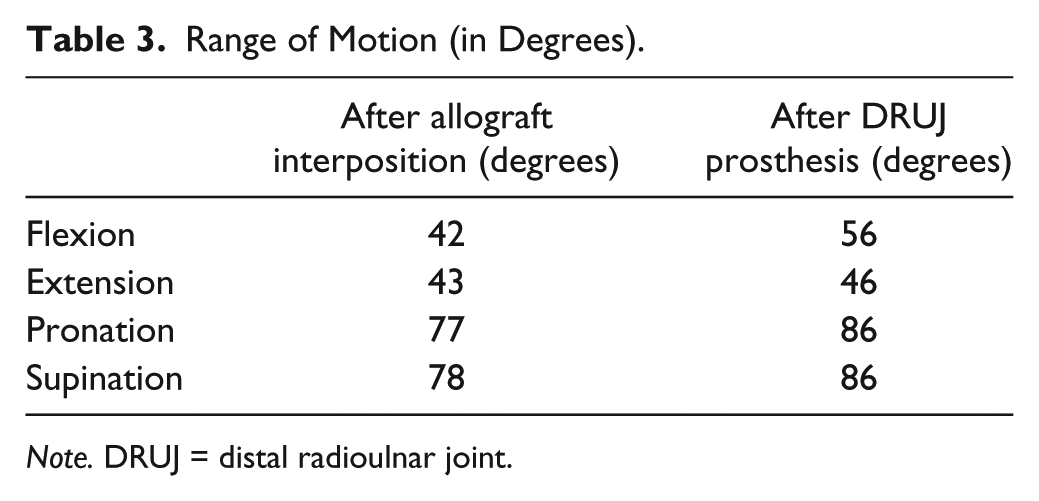
Note. DRUJ = distal radioulnar joint.
At the final follow-up after DRUJ prosthesis, all 7 patients demonstrated a stable DRUJ on clinical examination and weight-bearing x-ray studies, in contrast to their post–allograft arthroplasty (pre-DRUJ prosthesis) exams and imaging. Wrist and forearm motion improved postoperatively, as displayed in Table 3. Grip strength and lifting capacity improved as displayed in Table 4. Individual case data are summarized in Table 1.
Functional Strength.
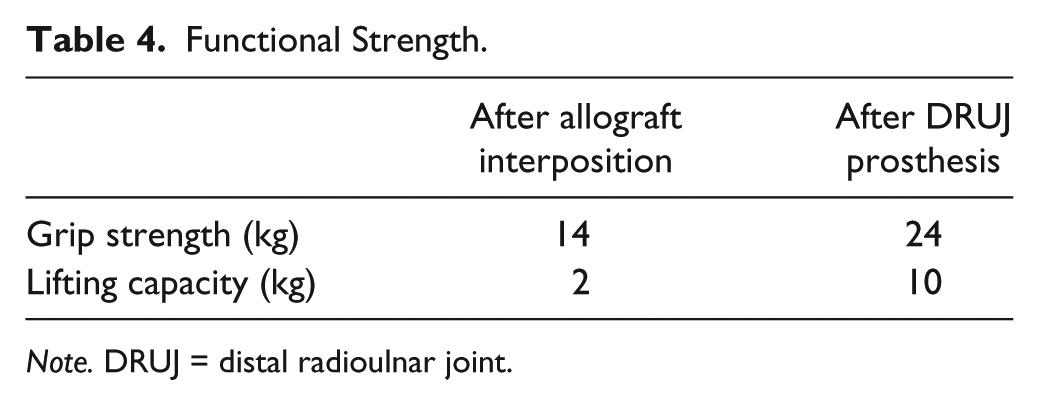
Note. DRUJ = distal radioulnar joint.
There were no major complications, but 2 patients developed ECU tenosynovitis several months after surgery. They both underwent ECU tenolysis, tenosynovectomy, and (in one case) a fascial graft from the abdomen. Incomplete relief resulted in a second surgery: an ECU wrap with a synthetic film (Seprafilm) in one case and a posterior interosseous neurectomy in the other case. At the final follow-up, both patients confirmed complete resolution of symptoms. In our current technique, a fascioretinacular flap is employed in the initial DRUJ replacement surgery as a barrier to prevent subsequent ECU irritation.
The radiographic evaluation showed no complications with the implants (including no signs of loosening) and maintenance of DRUJ congruity in all cases. These patients currently practice sports without impairment, as one plays softball and boating and another can do push-ups and plays golf.
Discussion
Distal radioulnar joint injuries may be very disabling. Several options are described in their management, but our current knowledge leads us to preserve the anatomy as far as possible. 5 Ablative procedures at the distal ulna may produce painful forearm instability resulting in decreased grip strength 25 and variable impairment of hand function. The loss of ulnar head support results in the development of painful dynamic radioulnar impingement. Ulnar impingement may produce erosive changes in the medial cortex of the radius, but otherwise radiographic findings may not be obvious without specialized views. 1 An easy way to diagnose and highlight impingement is with a weight-bearing cross-table posteroanterior radiograph (elbow flexed to 90° and forearm in neutral rotation). 12
Several techniques have been devised to restore forearm stability and reverse this disabling condition, but a lack of consensus still remains. 14 Many soft tissue procedures attempt to overcome secondary painful distal forearm instability, but none have provided consistent symptom relief nor return of stability. 25 The Achilles tendon allograft interposition arthroplasty was developed to relieve radioulnar impingement symptoms, theoretically avoiding the complications of a prosthesis.9,16,23 Although favorable results have been published, the problem of painful radioulnar convergence has not been completely resolved, as the patients of this study, all of whom received an Achilles allograft interposition, showed recurrence of their symptoms.
Sotereanos et al described their interposition arthroplasty with an Achilles allograft “pillow” 9 to maintain the radioulnar relationship and prevent painful convergence.9,16,22,23 Their last report included 26 patients (mean age, 43 years; mean follow-up, 79 months); results show pain relief by VAS and improvement in both forearm rotation and grip strength. This study had 2 complications requiring surgical treatment (radial shaft fracture and persistent pain). Three patients developed radiographic scalloping between the radius and the ulna. Although in one article Papatheodorou et al discussed the importance of cross-table weight-bearing radiographs to assess radioulnar convergence, 16 the study does not report the results of such radiographs in follow-up, so the magnitude of the true distal radioulnar convergence in these studies has not been published. Sotereanos et al described good results regarding improved motion and pain amelioration at rest. However, as the patients included in this article demonstrate, this technique cannot restore forearm anatomy and may not restore forearm stability. No other reports of this technique have been published.
Painful ulnar impingement is a real challenge. In most cases, the patients have undergone several prior procedures; no technique has demonstrated clinical superiority. 16 Currently, there is increasing interest in prosthetic options with many new designs of partial or total ulnar head prostheses, and total DRUJ prostheses. Ulnar head replacements (replacing only the ulna’s articular surface) have shown fair results. Their stability depends on the surrounding soft tissues’ integrity, which may be lacking as these patients typically undergo several prior surgeries. 15 The multiply operated forearm presents a unique challenge in which the surgical field is imbued with a heavy and treacherous scar burden obscuring natural tissue planes, compromising soft tissues available for coverage and closure. The restraining ligaments are often heavily scarred or resected in the multiply operated DRUJ. Similarly, the use of these implants in cases of radial sigmoid notch involvement or impaired wrist stabilizers is less likely to have good outcomes.
Conversely, results after total DRUJ replacement are very encouraging, even in the setting of the multiply operated forearm. Total DRUJ prostheses require neither integrity of soft tissue stabilizers nor an intact sigmoid notch. 8 The Aptis DRUJ prosthesis is a semiconstrained ball-and-socket joint, replacing all the 3 elements of the DRUJ (ulnar head, radial sigmoid notch, and ligamentous stabilizers). 11 It recovers lifting ability and allows longitudinal motion of the radius during forearm rotation, while restoring and maintaining an anatomic radioulnar relationship. In doing so, this total DRUJ prosthesis solves the difficult dilemma of dynamic radioulnar impingement. It allows full range of motion, immediate progressive weight bearing, and an early return to the patient’s activities. It is particularly useful in cases of failed, painful, and unstable distal ulna excision, or for failed partial prosthesis, as few viable options remain in these circumstances. 17 Although longer follow-up is necessary, the short-term and midterm results reported are very encouraging even in young and manual workers.2,4,6,17,19 Some complications of this implant have been published, but they can be avoided with careful surgical technique, as the later reports have shown.
In this study, we show the results of managing painful instability following Achilles tendon allograft interposition arthroplasty by replacement with the Scheker prosthesis. As noted here, soft tissue interposition techniques do not adequately prevent the radius from collapsing into the ulna, as these techniques cannot restore the support given by the ulnar head to the distal radius.
Furthermore, the failures of the tendon allograft interpositional arthroplasty technique presented in this study illustrate the dichotomy between the functions of tendon and cartilage, and the complications that can arise when one is used to replace the other. Articular cartilage is a highly specialized connective tissue functionally comprised primarily of water, proteoglycans, and perpendicularly oriented type II and IX collagen; its sponge-like configuration optimally facilitates transarticular load transmission through its unique spring-like ability to resist compressive forces.10,21 Conversely, tendons are largely comprised of type I collagen organized in a parallel configuration optimized to transmit tensile forces developed during muscle contraction to bone end points.7,13
As such, tendon lacks biomechanical features essential to the shock-absorbing function of cartilage—features it cannot deliver when used to prevent radioulnar convergence. The tendon allografts used for interpositional arthroplasty in our patients illustrate this point, as these grafts could not withstand the compressive forces across the DRUJ (forces that the native cartilage was designed to support and transmit across the joint).
All of our patients had worn out their interposed Achilles tendon allografts from repetitive grinding physiologic radioulnar compressive forces within a matter of months, producing recurrent impingement (noted preoperatively on imaging and confirmed intraoperatively). Of note, the literature reporting good results bases this evaluation on pronosupination and pain relief at rest; it fails to report lifting capacity—the main function of the forearm. As an alternative to tendon allograft interpositional arthroplasty, we therefore propose DRUJ implant arthroplasty for treatment of painful radioulnar convergence following distal ulnar ablation.
Footnotes
Authors’ Note
All authors contributed significantly to the development of this article.
Ethical Approval
This study was approved by the University of Louisville Institutional Review Board, CR-2738.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients being included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.