
Abstract
Keywords
Introduction
For patients with pisotriquetral (PT) osteoarthritis (OA), pisiform excision (ie, pisiformectomy) is an effective surgical method to relieve symptoms if conservative treatment fails.6,12 However, PT OA may be difficult to distinguish from other ulno-carpal problems. 11 In radiological evaluation of the wrist, lateral, anteroposterior, and semisupinated oblique views are often used to grade PT OA. By lack of a specific classification, 6 general radiologic OA parameters are used, but can be easily misinterpreted due to overlapping projection of carpal bones. 5
One OA parameter that is often used in orthopedics is the minimum joint space width (JSW), as a measure of joint space narrowing. 7 Patients with PT OA are also likely to show certain joint space narrowing. 6 However, the extent of joint space narrowing and its deviation from the JSW in normal anatomy is unknown. In this pathoanatomic study, we therefore compared the minimum JSW of patient wrists having PT OA with the minimum JSW in healthy wrists. To avoid problems with overlapping projection as observed in radiographs, we quantified the JSW using 3-dimensional (3-D) computed tomography (CT) images of the PT joint.
Materials and Methods
Study Design
We retrospectively screened patients suspected for PT OA for eligibility. Inclusion criteria were ulnar-sided wrist pain, surgical treatment with pisiformectomy, confirmation of PT OA based on intraoperative findings, and the availability of a preoperative CT scan of the affected wrists in neutral position. Exclusion criteria were nonconfirmed OA at surgery. We included 8 preoperative CT scans (Figure 1) from 7 patients (1 man; 6 women; average age, 44 years; range, 24-60) treated with a unilateral (n = 6) or bilateral (n = 1) pisiformectomy. As control group, we included bilateral CT scans of 10 healthy wrist pairs in neutral position from volunteers without wrist complaints or a history of injury to the wrist (2 men; 8 women; average age, 30 years; range, 28-40). This study was approved by our Human Research Committee. Informed consent was obtained from all individual participants included in the study.

Combined sagittal and coronal CT slices of a patient wrist visualizing the joint space between the Pi and Tr.
Modeling Technique and Evaluation
The 3-D CT surface models of the pisiform and triquetrum were created using custom made software (Figure 2a), which has been described previously. 10 We calculated the smallest distance between the points describing the pisiform and the points describing the triquetrum reflecting the minimum JSW (Figure 2b).
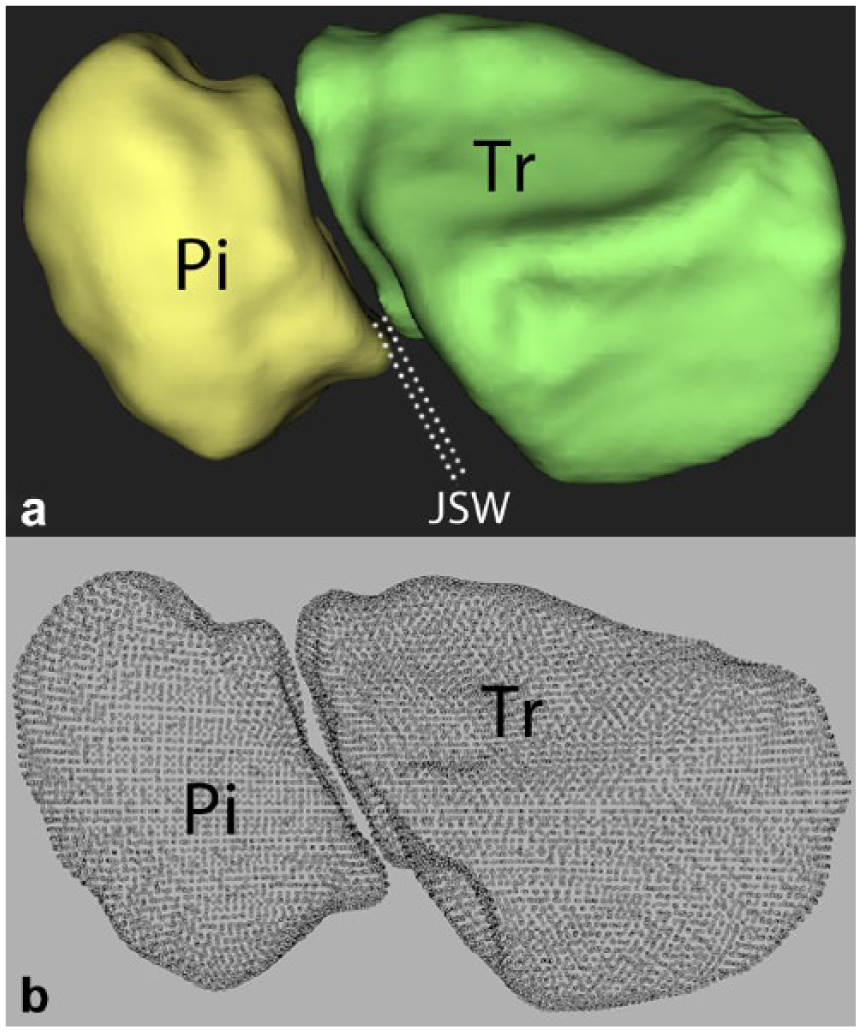
a, Virtual 3-dimensional CT surface models of both the Pi and Tr, visualizing the JSW. b, Minimum JSW was calculated based on the smallest distance possible between the points describing the pisiform and the points describing the triquetrum.
Statistical Analysis
Statistical analysis included determining the mean and standard deviation (SD) or median and interquartile range (IQR) of the JSW depending on data distribution. The Shapiro-Wilk test was used to test whether data were (non-)normally distributed. To compare patient and normal values, the student t test or Mann-Whitney U test was used, also depending on data distribution. A 5% significance level was used for the analysis.
Results
All data were nonnormally distributed. For patients, the median JSW (IQR) was 0.1 mm (0.0-0.2), and for healthy volunteers, 0.8 mm (0.3-0.9). The Mann-Whitney U test demonstrated a significance difference (P = .007).
Discussion
In this study, we compared the minimum JSW in the PT joint between OA patient wrists and healthy wrists. Our results demonstrated that the minimum JSW as measured on 3-D CT was significantly smaller in the OA patient wrists, indicating cartilage damage.
One previous radiologic study investigated the JSW in the PT joint in 10 healthy wrists using CT scans and reported a median value of 1.1 mm. 3 Another study using standard radiographs reported a mean value of 1.5 mm regarding the JSW in the PT joint. 4 In both studies, the reported values were obtained with the wrist in neutral position similar to our study, but were slightly larger than our reported normal values. This could be explained by a methodological difference; we calculated the smallest distance possible in an automated fashion, whereas the other studies were based on manual distance measurements. In the latter studies, however, no pathological values obtained from patients were included for comparison. Without such a direct comparison, it is difficult to assess whether measuring JSW has a potential to distinguish between OA and healthy PT joints, thus may be considered a clinically relevant parameter.
Regarding the patients in our cohort, the level of OA was likely to be influenced by many factors, such as patients’ activity level, previous therapy, and etiology, for example, rheumatic or posttraumatic. Due to the retrospective design of our study and the relative small sample size, we were unable to relate the quantified JSW to these patient-specific factors. Another limitation of the current study was that the healthy volunteers were generally younger than the patients. The healthy CT data were obtained from a historical control group available from previously conducted experiments. Ethical concerns and radiation safety issues kept us from repeating scans in older volunteers. Nevertheless, the average ages of both the patients and volunteers were lower than the usual age (~55 years) at which people start developing OA.1,2,9
Contrary to the symptomatic patient group described in the current study, some patients might not even seek medical attention despite having severe radiographic OA. OA of the PT joint can be a normal stage in aging 5 accompanied by symptoms and disability to which patients may adapt, for example, by lowering their functional demands for daily living. When considering surgery, surgeons should focus on the concordance of symptoms, signs—for example, confirmatory response injections—and radiologic imaging, rather than on using imaging abnormalities alone to motivate a surgical decision. 8
The applied 3-D CT technique described in the current study should not be seen as a clinical tool for examination of each patient with ulnar-sided wrist pain. The purpose of the current study was to investigate the clinical relevance of JSW evaluation in diagnosing cartilage damage. Radiography remains the imaging modality of first choice. We expect that the radiographic evaluation of the PT joint space has potential diagnostic value as joint spaces were significantly narrowed in patients in our 3-D evaluation. Due to absence of a gold standard for diagnosing PT OA, future clinical studies should focus on correlating radiographic features with clinical parameters and intraoperative findings.
Footnotes
Authors’ Note
The work of this study was performed at the Academic Medical Center, University of Amsterdam.
Ethical Approval
Approval of project MEC 2013_242 (use of volunteer data) and MEC W15_087 (use of patient data).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.