
Abstract
Introduction
Outcomes of digital nerve repair continue to be suboptimal despite the use of various repair techniques throughout history.11,19,22 Nerves in approximately 10% of hand injuries require surgery, 16 and it is estimated that only 50% to 80% of patients regain functional use of the hand after digital nerve repair. 21 An extensive amount of rehabilitation is often necessary and can have significant social and economic effects on the patient. The reasons for suboptimal outcomes are poorly understood but appear to be multifactorial, and various authors have proposed theories to explain the poor outcomes of primary nerve repair.
One theory implicates mechanical failure at the repair site leading to gapping and disordered nerve regeneration. A tension-free repair is the ideal, but Goldberg et al estimated that up to 4 N of load may be borne by a digital nerve. 3 Previous studies have investigated the tensile strength of direct nerve repairs.2,7 Giddins et al observed that the number of sutures crossing the coaptation site correlated with the tensile strength of the repair. 2 Repair site gapping in the early recovery period may encourage neuroma formation as the regenerating nerve fibers lose directional healing.
The other popular theory for poor outcomes implicates repair site biology as a mode of failure of digital nerve repair. The suture line created by nerve repair introduces the possibility of neuroma formation as well as intraneural fibrosis. Levinthal et al characterized repair site fibrosis in a histological analysis of nerve laceration repair in a canine model. 6 Martins noted in a rodent model of nerve repair that sutures create an inflammatory response at the repair site, limiting axonal regeneration. 10 Eliminating sutures or decreasing the number of sutures necessary to create a strong repair may be biologically favorable and could improve neural regeneration potential.
To date, there is no general consensus regarding the optimal suture size or configuration to use during primary digital nerve repairs. A recent survey of hand surgeons concluded that microsuturing is the gold standard for primary nerve repair, but 95% of respondents considered using alternate techniques that were less technically demanding, less time-consuming, and produced improved outcomes. 14 The same study found that conduit-assisted repair was the most common alternative method. This method allows axonal regeneration across 2 opposed nerve ends with minimal or no sutures at the coaptation site. 1 The epineural sutures placed at the proximal and distal nerve-conduit junction sites provide structural support. Fewer sutures at the repair site offer the advantage of less inflammation and intraneural fibrosis. The physical shape and space constraints inside the nerve conduit also may help to prevent neuroma formation. Besides a mechanical effect, the conduit may benefit nerve regeneration by a chemical effect by preserving neurotrophic growth factors.5,18 These trophic factors promote directional healing of the nerve and protect the nascent repair from perineural scarring.8,9 Both biologic and synthetic conduit materials from various sources have been used with varying success.
The current study seeks to address the question of digital nerve repair strength related to the size, number, and placement of sutures used during conduit-assisted primary digital nerve repairs. Many studies have analyzed tensile strength of direct repair2,7 and fibrin glue–based repairs.4,10,15,17 However, no work has investigated the effect of suture configuration in conduit-assisted digital nerve repairs. We hypothesized that repairs with 8-0 nylon suture would achieve a stronger repair than repairs with 9-0 nylon and that the number of sutures placed in the repair would directly correlate with its ultimate tensile strength. The goal of the study is to discover which repair technique best achieves a strong repair while limiting the amount of suture at the primary coaptation site.
Materials and Methods
Institutional review board approval was obtained for this study. All testing was performed within the Biomechanics Laboratory at Allegheny General Hospital during a 3-month period in 2016. Four fresh-frozen cadaveric hands were thawed to room temperature and the digital nerves from each finger were dissected and then transected at the proximal bifurcation of the common digital nerve and the distal trifurcation of the proper digital nerve. The 4 specimens were all from male donors with an average age of 58 year (range, 48-64 years). Saline was used to keep the specimens moist. Nerve sections of 5cm were prepared from the specimens, and the diameter of each was measured with calipers at the midpoint of each length. All nerve harvesting was performed by investigator N.B., and all further sample preparation was performed by investigator D.K. The nerves were divided into 11 different groups with 9 specimens per group and the same average diameter in each group. Nerves from each hand were distributed evenly among all groups so that nerves from each hand would not have only one type of repair. Groups were classified by the number of sutures at the coaptation site and at the conduit ends. The number of sutures at the coaptation site is designated with the first number and the number of sutures at each end of the nerve-conduit junction is the second number, followed by designations of suture size used at each site (ie, 8-0 or 9-0). For example, Group J [2(9-0)/4(8-0)] has two 9-0 nylon sutures at the coaptation and four 8-0 sutures at each end of the nerve-conduit junction for a total of 10 sutures (Figure 1).
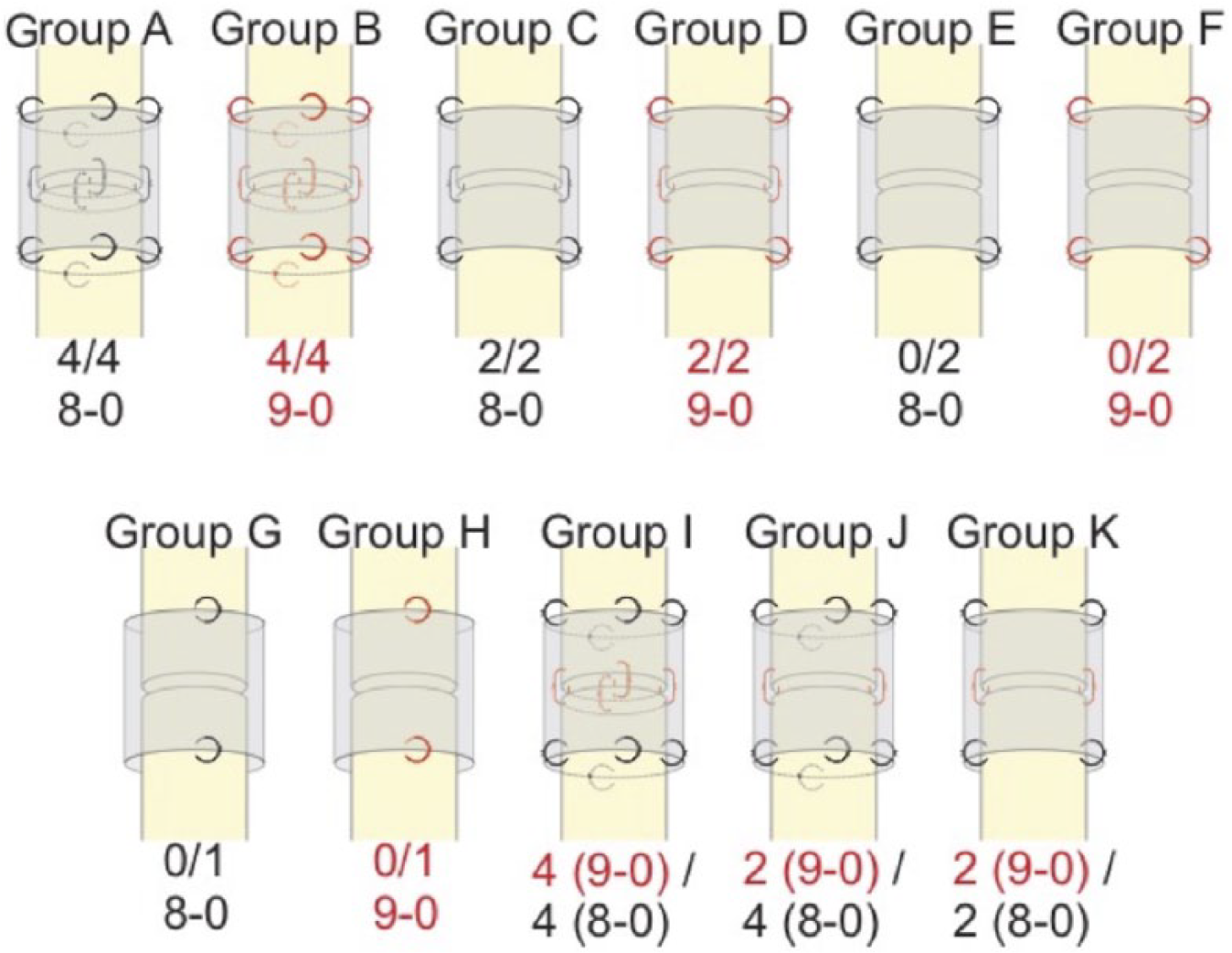
Diagrammatic representation of all the repair groups.
Digital nerve lacerations were created in each specimen with a No. 15 scalpel. Primary coaptation repairs were performed by placing simple 8-0 or 9-0 Nylon (Covidien, Chicopee, Massachusetts) epineural sutures under loupe (×2.5) magnification, 1 mm from the cut ends. Knots were tied using a surgeon knot and 4 subsequent single throws lying squarely. When 2 sutures were used at the coaptation site, they were placed 180° from each other. When 4 sutures were used, they were placed 90° to each other. The repaired nerves were then wrapped with Nerve Protector (AxoGuard, AxoGen, Alachua, Florida), which was used as described by manufacturer specifications. The nerve conduit was cut to 12 mm in length and 10 mm in width and bathed in saline prior to use to provide pliability. The nerve conduit was placed around the repaired nerve and trimmed to match the nerve diameter. The conduit was then folded around the nerve to form a tube, and a simple 8-0 nylon suture was placed at each end of the conduit where the leaflets overlapped; this suture did not include epineurium and was not counted as a nerve-conduit junction suture. The nerve-conduit sutures were performed in a similar fashion using either 8-0 or 9-0 nylon. The nerve-conduit sutures were placed 1 mm from the edge of the conduit and entered and exited the epineurium a distance of 0.5 mm proximal and distal to the edge of the conduit. If the group required no primary coaptation sutures, the nerve ends were placed end-to-end in the conduit and the conduit was sutured into a tube as previously described.
For biomechanical testing, approximately 16 mm of nerve at the free ends were glued to a 4-layer gauze pad with cyanoacrylate adhesive and allowed to set for 30 minutes: 15 minutes with the gauze pads under approximately 230 g of load to ensure a uniform bond and 15 minutes with the gauze pads uncovered to ensure that the cyanoacrylate was fully set. Specimens were kept moist at all times. The specimens were loaded into a tensile testing machine (Haake Mars II, Thermo Fisher Scientific, Inc, Waltham, Massachusetts; resolution 0.001N), and stainless steel clamps gripped the entirety of the gauze pads to secure the nerve from slipping. Specimens were preconditioned 5 times with a ramp load of 0.25 N, followed by loading to failure at 0.33 mm/s. Tension was recorded at 10 Hz.
A 2-way ANOVA was performed to determine whether number of suture or suture caliber affected the maximum load to failure (SPSS, IBM, Armonk, New York). A P value less than .05 was used to determine the validity of the null hypotheses. If a significant result occurred, Tukey’s post hoc test was used to determine where the significant difference existed within the significant factor. Furthermore, two 1-way ANOVAs over all 11 groups were performed to evaluate which construct’s load-to-failure values were statistically different, as well as to ensure that specimen diameters were not significantly different between groups.
Results
The 2-way ANOVA showed that increasing the number of sutures in the repair significantly increased the maximum failure load in all groups regardless of suture caliber used (P < .01) (Figure 2) The 2-way ANOVA also showed that suture size made a difference; 8-0 nylon repairs were stronger than 9-0 (P < .01) (Figure 3). Repair groups and their mean maximum failure strength are reported in Table 1. Repairs with the same Greek letter designation are not significantly different with regard to mean maximum failure load. The mean maximum failure load of all groups ranged from 0.80 N to 3.71 N. The strongest repair construct consisted of two 9-0 sutures at the coaptation site and four 8-0 sutures at each end of the conduit (group J). The weakest repair consisted of no coaptation site sutures and one 9-0 suture at each end of the conduit (group H). The maximum failure strength of repair groups with a total of 6 or 8 sutures did not significantly differ between groups regardless of suture configuration or suture caliber. The mean maximum strength of repair group E (no coaptation sutures, 2 conduit sutures at each end) demonstrated similar strength to repairs with 2 sutures at each end of the conduit and 2 coaptation site sutures (groups C, K, D, P > .05).
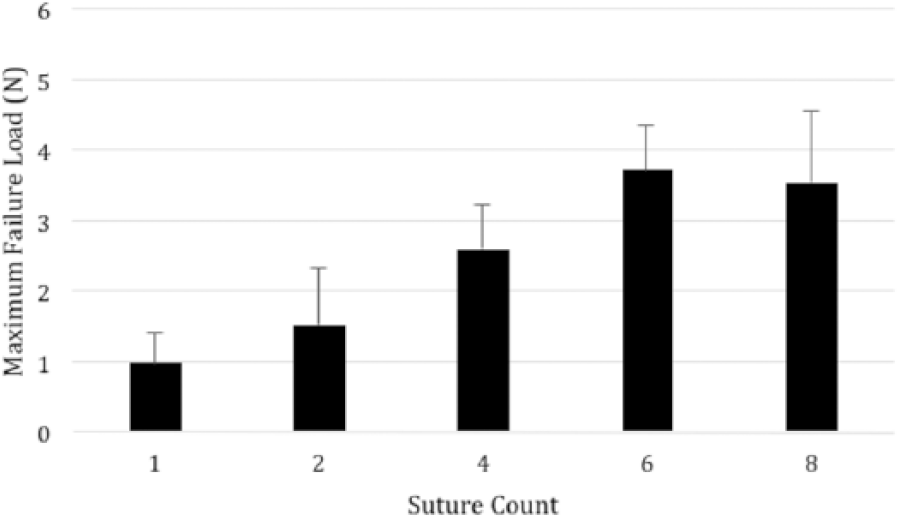
Bar graph showing maximum load to failure with varying total number of sutures. The 2-way analysis of variance showed that increasing the number of sutures increased the strength. In this analysis only the groups that had one type of suture caliber were included.
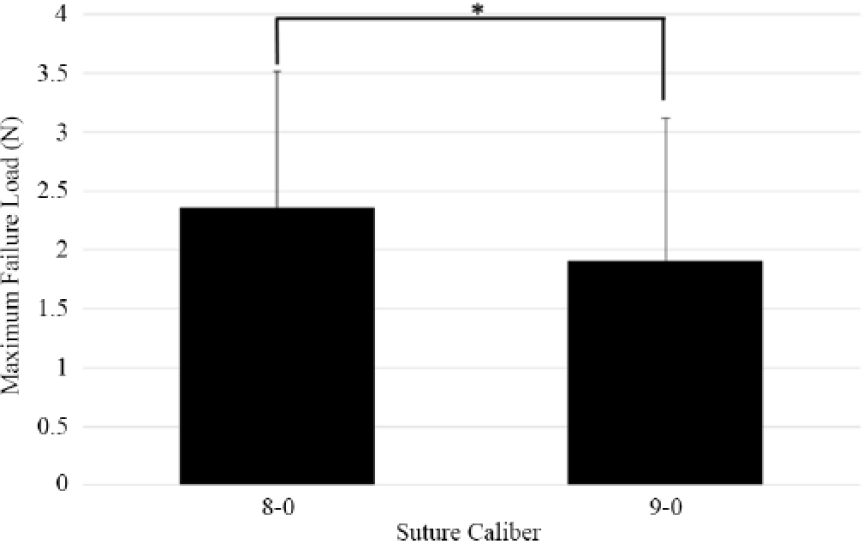
Bar graph showing 2-way analysis of variance of suture size; 8-0 nylon failed on average at 2.36 N, while 9.0 nylon failed on average at 1.91 N (P < .01).
Summary of Repair Groups With Mean Maximum Load to Failure.
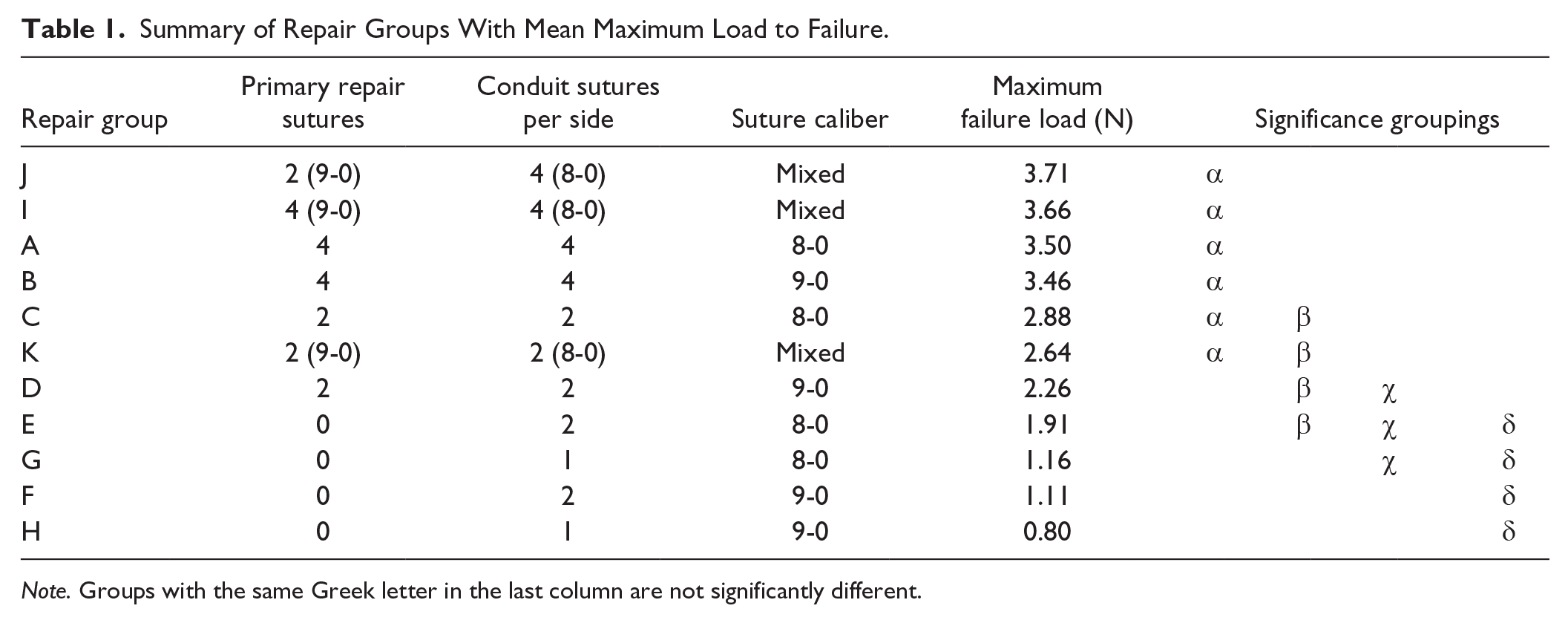
Note. Groups with the same Greek letter in the last column are not significantly different.
Discussion
This study is the first, to our knowledge, which investigates the biomechanical properties of primary nerve repair augmented with a nerve conduit. We have shown that, in general, larger suture caliber and more suture in the construct increased the tensile strength of the repair. The results from this study may help improve nerve repair outcomes if the cause of failure is due to weakness of the repair or inflammation from suture material.
In terms of mechanical strength, it has been shown in previous studies and in ours that increased suture at the coaptation site increases load to failure. It has also been shown that at 8 weeks post repair, repaired nerves only have 63% strength compared with control. 20 Unfortunately, there is no in vivo evidence that determines a critical amount of gapping and how that relates to histologic and clinical outcomes. 13 Goldberg et al found that a 4 suture repair with 8-0 nylon 1 mm from the nerve edge failed at 2.2 N, while the same construct with 9-0 nylon failed at 1.6 N. 3 They also found that the in situ digital nerve may be subject to 4 N of load. Therefore, it seems reasonable to strive for the repair technique with the highest tensile strength to protect the repair and allow neural regeneration. One of the primary findings of the study is that the number of sutures increases the strength of repair. This result seems intuitive and follows the same principles of tendon repairs. Another finding of the study is that using 8-0 nylon results in a stronger repair than 9-0 nylon. This again is intuitive. One point that needs to be clarified is that we performed a 2-way ANOVA to evaluate suture number and size, and we performed a 1-way ANOVA so that we could compare the failure loads of the different construct designs. So while it is true that number of suture and using 8-0 nylon gives a stronger repair, this does not mean in a single comparison between 2 groups it will necessarily hold true. Case in point is group J 2(9-0)/4(8-0) is statistically the same as group I 4(9-0)/4(8-0) even though it has 2 fewer sutures.
In terms of the biological factors affecting nerve healing, it is hypothesized that allowing trophic factors to accumulate at the repair site aids in healing. Therefore, the use of a nerve conduit is conceptually appealing as it may aid in containing these beneficial factors. In addition, there is evidence to show that increased suture at the repair site of a peripheral nerve increases the local inflammatory response and causes neural fibrosis. Logically, this process inhibits functional regeneration of nerves. Therefore, we should aim to decrease the amount of suture material at the repair site. The conduit-assistance technique allows the placement of suture away from the nerve injury site to the end of the nerve-conduit junction which will provide strength to the construct but keep the inflammation from suture at a less critical site away from the primary injury site.
Taking into consideration these known factors of nerve repair, the most ideal repair construct is one which maximizes tensile strength while minimizing suture material and takes the least amount of time to perform. In our model, this is represented by group K (two 9-0 sutures at the repair site and two 8-0 sutures at each nerve-conduit interface). The total number of sutures is 6 and the 2 sutures at the primary coaptation are the smaller caliber 9-0. J (2(9-0)/4(8-0)) may also be a reasonable repair because there is minimal suture at the repair site and the suture is smaller caliber; it is also the strongest construct of all those that were tested. The greatest number sutures (8) are outside the repair site, and this location of suture may or may not affect nerve regeneration. However, placing 10 sutures for a repair construct would be require a long period of the time and would be labor intensive. For this reason, this repair construct is not ideal.
There are several limitations to this study. First, it is a cadaveric model with nerve specimens removed from the body. Thus, the mechanical loads imparted on the specimens in our model may not accurately reflect the forces that repaired digital nerves experience in a digit, with surrounding soft tissues, under physiologic motions. We also only tested repair strength at time zero, and the effect of biologic healing on repair strength could not be assessed. Second, we only used one type of nerve conduit. There are many types of materials and brands of nerve conduits available on the market, which may have different properties than our model. Most importantly, the forces imparted to a digital nerve in vivo and the limits of gap formation for adequate nerve regeneration remain unknown. While the nerves are strained by finger extension and a gap may result, no details are scientifically available. A better understanding of the biology of nerve regeneration would help in the application of this work to clinical cases.
In conclusion, this is the first study to investigate maximum failure load of varying repair configurations in conduit-assisted primary digital nerve repairs. It is the senior author’s current practice to use group K when performing such repairs. This repair is not statistically different from the strongest repairs in the study, has the least number of sutures, and has a small caliber suture at the coaptation site.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that AxoGen, Inc, donated conduit for use in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by internal funds.