
Abstract
Introduction
Osteoarthritis of the hand affects a large percentage of the population and can lead to significant functional disability. 13 The proximal interphalangeal (PIP) joint is the second leading cause of hand pain and is one of the most common joints affected by degenerative arthritis.7,13 First-line therapy typically consists of nonsteroidal anti-inflammatory drugs, lifestyle modification, splinting, and steroid injections. When these more conservative measures fail to provide adequate or sustained pain relief, surgical intervention is considered. Various arthroplasty devices and techniques have been developed with the goal to offer pain relief without loss of functional range of motion (ROM).8,10,14,18-20,22
Among devices developed, the silicone implant has shown success since its development in the 1960s.2,8,16,25,26 Used frequently for chronic joint pain associated with rheumatoid arthritis, they are a reliable means of achieving pain relief and maintaining function. 17 Complications associated with silicone arthroplasty include stiffness, reactive synovitis, and joint instability. Implant fracture may also occur, but it is usually well tolerated and often does not require a revision procedure.9,24 Recent literature has continued to support the use of silicone implant arthroplasty for osteoarthritis of the PIP joint. 1 The objective of our study was to evaluate the clinical effectiveness of silicone arthroplasty for idiopathic osteoarthritis of the PIP joints of the hand.
Methods
We performed a retrospective review of all PIP arthroplasties performed at a single institution from 2005 to 2013 by authors GAB and JEI. Study protocol was approved by the institutional review board. Those with PIP arthroplasty were identified using CPT codes 26535 and 26536. Participant inclusion criteria were patients with idiopathic osteoarthritis and above 18 years of age. Exclusion criteria included history of rheumatoid or autoimmune-related arthritis, septic arthritis, or posttraumatic arthritis. The silicone implants used by the senior author during the study period included the Swanson implant (Wright Medical, Memphis, Tennessee) and the SBI implant (Small Bone Innovations, Morrisville, Pennsylvania), both silicone arthroplasty prosthesis.
A chart review was conducted to record demographic data and comorbidities including diabetes, connective tissue disease, tobacco use, and steroid injections. Preoperative and postoperative ROM, Disabilities of the Arm, Shoulder and Hand (DASH) scores, key pinch strength, grip strength, and pulp to palm distance were collected. Preoperative and postoperative pain scores on a 10-point visual analog scale (VAS) were also recorded. Using 4-point Likert scales, patient subjective evaluation of surgical success with respect to pain, deformity, function, and strength were obtained. Overall patient satisfaction and likelihood to have the intervention again given current outcomes were also determined. For the purposes of this study, patients were asked to return for a follow-up evaluation. Radiographs were obtained and reviewed. For participants who were unable to return for a follow-up visit, a survey, pain score, and DASH questionnaire were completed and returned by mail.
Preoperative and postoperative ROM, DASH, and VAS were compared and analyzed with a paired t test to identify statistically significant differences (P < .05). Mean key pinch and grip strength were compared between the operative and the contralateral unaffected hand of each patient also using a paired t test. Univariate and multivariate logistic regression models were used to determine predictors of revision surgery. Functional comparison of different finger arthroplasties was completed using analysis of variance.
Results
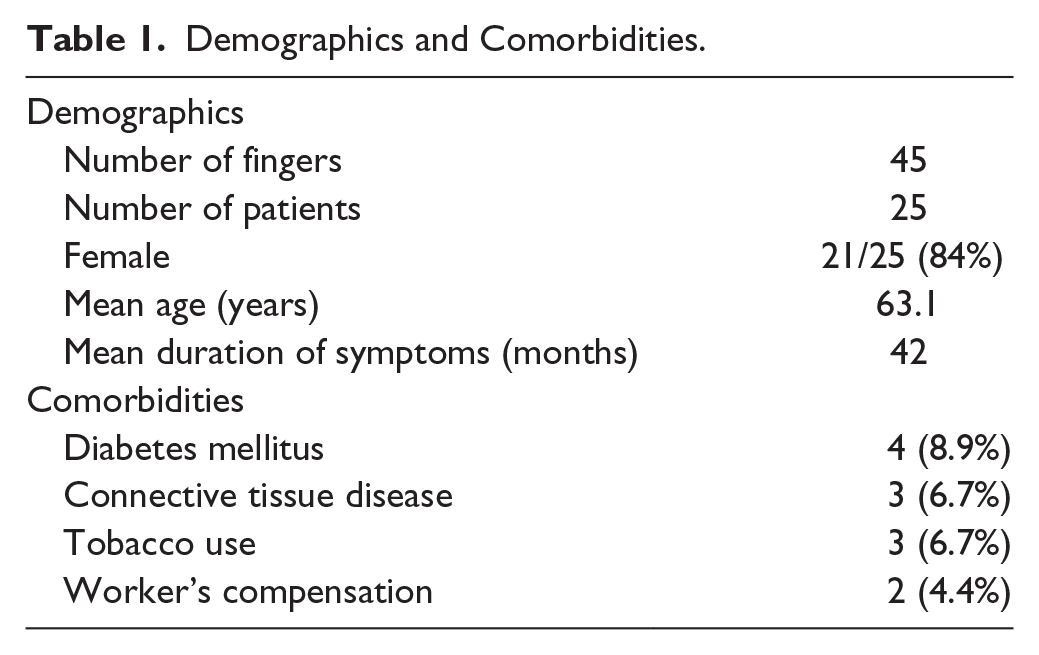
A total of 45 fingers in 25 patients were included in this study. Mean and median follow-up period was 3.5 and 3 years, respectively. Two participants mailed in surveys, as they could not present to clinic. Demographics and comorbidities are shown in Table 1. The most common finger affected was the long finger, 18, followed by ring finger, 15.
Demographics and Comorbidities.
There was no significant difference between preoperative and postoperative ROM (59.1° vs 59.2°). Analysis of variance showed no difference in postoperative ROM between finger groups. DASH scores, grip strength, and key pinch strength showed significant improvement postoperatively as seen in Table 2.
Range of Motion, Grip, Pinch, and DASH.
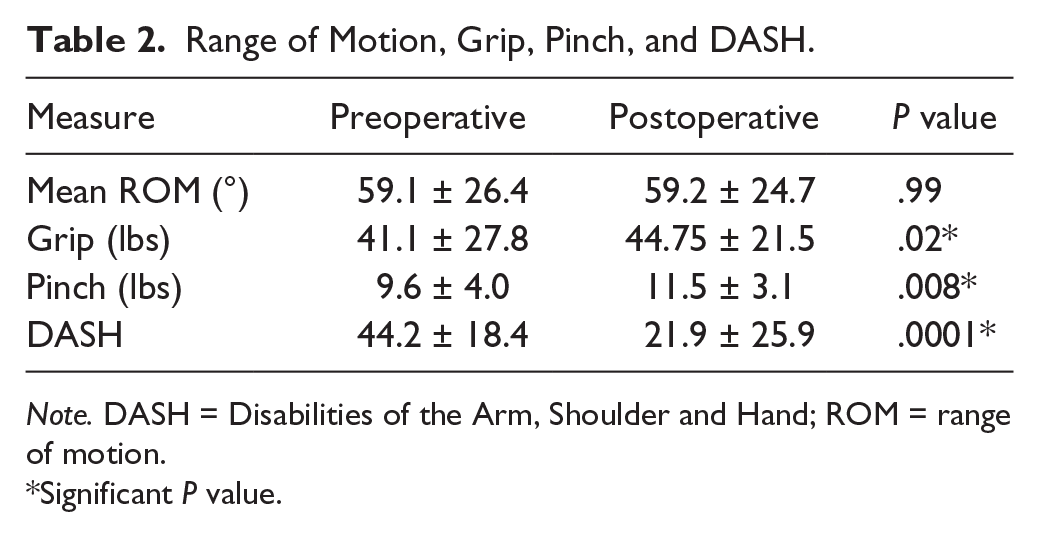
Note. DASH = Disabilities of the Arm, Shoulder and Hand; ROM = range of motion.
Significant P value.
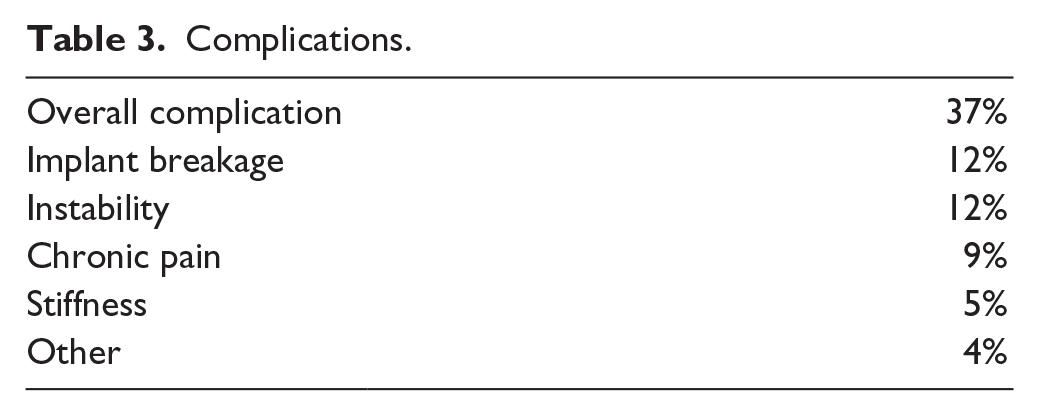
Overall complication rate was 37% and included stiffness, chronic pain, joint instability, deformity, implant breakage, and 20% of patients required revision surgery. Chronic pain was identified by chart review and defined as significant pain persisting beyond 1 year after the index procedure. Implant breakage was 12% based on review of radiographs (Table 3). Mean coronal deviation was 1° ulnar (range, 5° radial to 8° ulnar). Univariate logistic regression models showed that preoperative presence of noninsulin dependent diabetes predicted a 10 times higher odds of revision surgery (P = .07). Multivariate models did not yield any predictors of revision surgery. Types of implant included Swanson (44%) and SBI (56%). Univariate analyses showed no significant effect of the type of implant used or specific surgical digit on any of the outcomes measured.
Complications.
Analysis of patient questionnaires revealed significant subjective improvement in pain (7.4-1.9, P < .0001), deformity, function, and strength. Overall satisfaction was high at 84% with 91% stating that they would have the surgery performed again (Figures 1 and 2). There was no correlation between objective grip or pinch strength and subjective strength reports (r = 0.03, P = .85), and no correlation between radiographic or measured deviations and the subjective deformity reports (r = 0.20, P = .45).
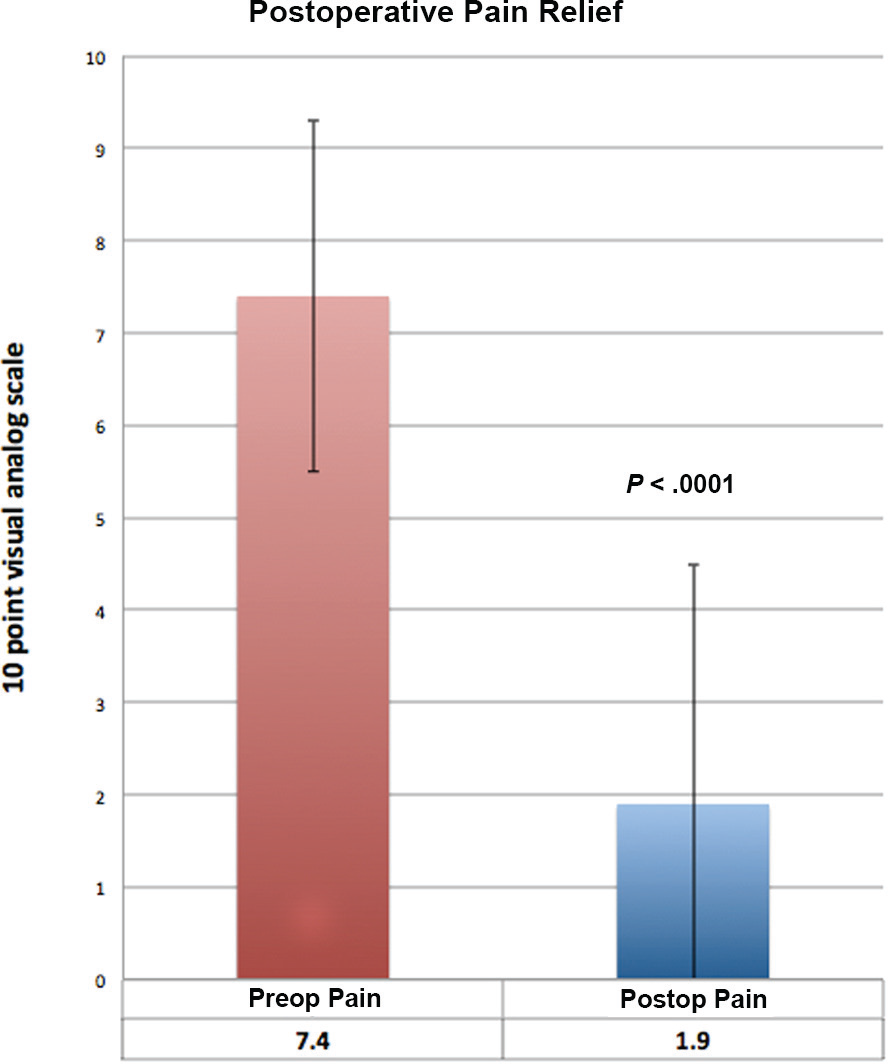
Preoperative and postoperative pain scores. A comparison of preoperative and postoperative subjective pain scores based on a Likert scale. Significant decrease in pain from 7.4 to 1.9 on a visual analog scale (P < .0001).
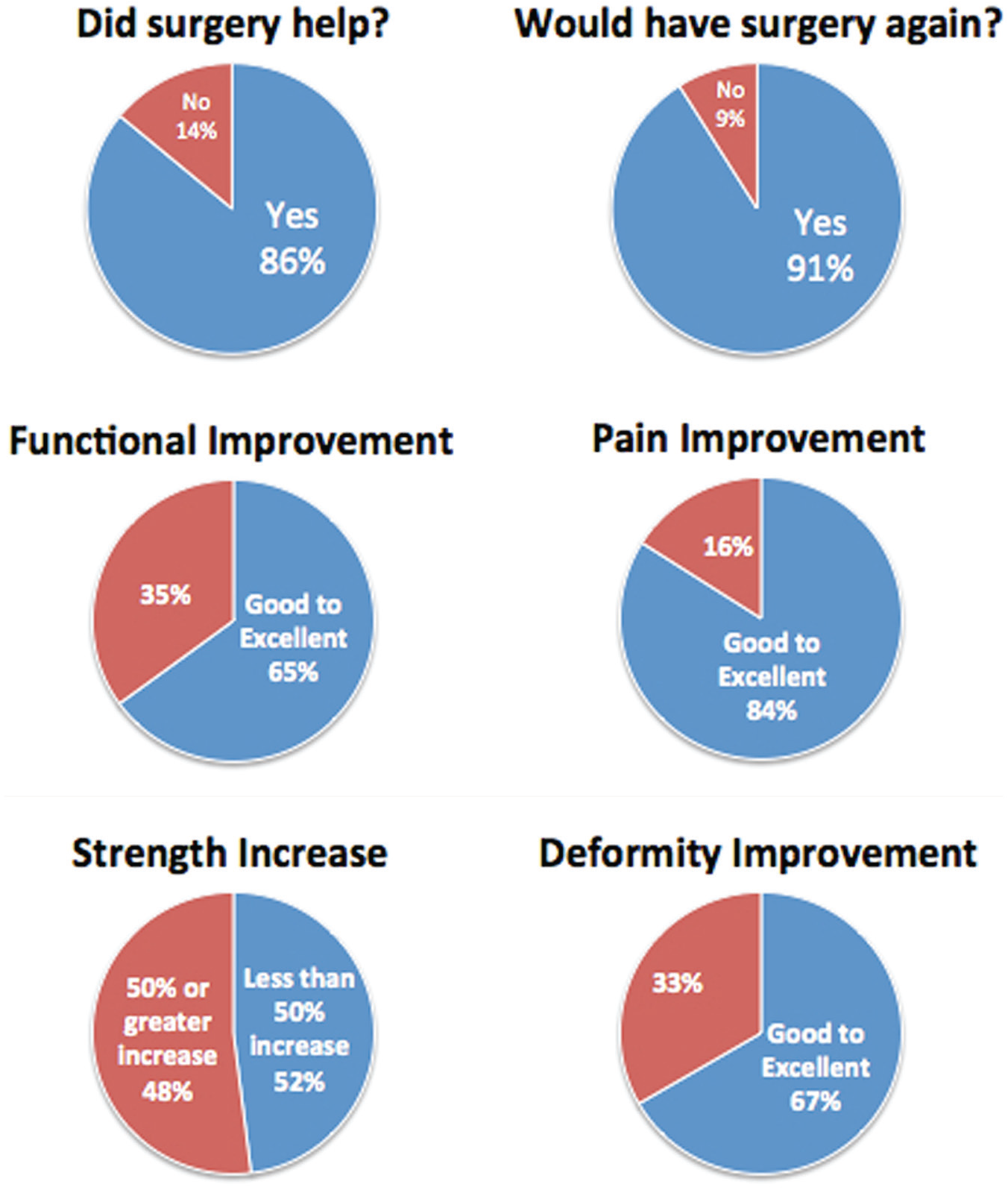
Subjective scores. Results of patient questionnaires show high level of satisfaction, excellent pain reduction, and improvements in function, strength, and deformity.
Discussion
The primary aim for arthroplasty of finger joints is to obtain pain relief while preserving motion. Merle et al showed in their series of 51 joints a preoperative to postoperative improvement in ROM from 38° to 63° with an average 3-year follow-up. 15 In a series of revision cases performed primarily for loss of range motion, Herren et al showed significant improvement from 33° to 71° with 4-year follow-up. 11 However, most studies, including ours, showed no significant change in preoperative and postoperative ROM.1,3,5,6,16,27 The average preoperative ROM in our series, 59.1°, was much larger than the ROM of these previous studies and likely the reason why there was no significant improvement.
There are limited data regarding effects of silicone PIP arthroplasty on grip and key pinch strength. Branam et al showed no significant improvement in grip strength postoperatively while Takigawa et al and Daecke et al showed small nonsignificant improvements.3,6,27 On the contrary, Merle et al reported an improvement in preoperative and postoperative grip strength (15.8 kg → 19.4 kg). 15 In our analysis, we found a significant improvement in grip strength from 17 kg preoperatively to 20.3 kg postoperatively.
Key pinch strength data are also variable with postoperative averages ranging from 1.4 to 5.6 kg in the literature.4,8,12,21 Takigawa et al found no significant difference in preoperative and postoperative key pinch strength. 27 We found a significant improvement in pinch strength of 0.9 kg. Postoperative grip and pinch values did not differ significantly from the nonoperative side.
Merle et al and Daecke et al showed significant improvement in preoperative and postoperative DASH scores (69.2 → 12.3 and 57 → 19, respectively).6,15 We found results similar to the literature showing significant improvement in DASH scores (44.2 → 21.9). This objective improvement in disability measurement is in line with our patients’ subjective reports of improved function.
The most common indication for PIP arthroplasty is debilitating pain and the silicone prosthesis has been shown to alleviate joint pain related to osteoarthritis. 4 Schneider et al, Pellegrini et al, and Dyer et al, all reported excellent pain relief in all of their patients in their series.8,21,23 Namdari et al had little to no postoperative pain in more than 75% of their patients. 16 Our study showed similar results with significant reduction of preoperative and postoperative pain (7.4 → 1.9).
Several studies have reported a majority of patients being very satisfied with their outcomes.1,11,16 Our study also assessed patient subjective measures of pain, function, strength, and deformity. About 84% of patients had good to excellent pain relief. Half of patients subjectively noted a greater than 50% increase in their strength. This was in line with our objective measures showing improved grip strength, but did not statistically correlate. Ultimately, 91% of our cohort stated that they would choose to have the surgery again.
The prevalence of implant deformity or failure as identified radiographically can be high with silicone implants. Fortunately, most are asymptomatic and have no resultant functional impact. Bales et al. showed radiographic evidence of deformity in 31 of 38 implant, 21 of which were fractured, but only 3 (7.8%) required revision. 1 Other studies have shown an average range of deviation or angulation between 10° and 17° in 24% to 55% of patients.3,11,15,16,27 Prevalence of implant fracture in the literature ranges from 9% to 55%.1,3,16,27 Takigawa et al showed the rate of implant fracture increases with time, with survivorship 98% at 2 years, 90% at 9 years, 80% at 10 years, 76% at 12 years, and 49% at 16 years. 27 Our results showed an implant fracture rate of 14% and a revision rate of 20%. Our evaluation of angulation showed a mean closer to neutral with a normal distribution of both radial and ulnar angulation. Without a prospective study following 100% of patients in the long-term, it is difficult to determine the incidence of any implant fracture with or without clinical significance. However, evidence suggests that only a low number of these deformity/fracture findings are actually clinically significant. A large review of silicone arthroplasties used for osteoarthritis, trauma, or rheumatoid cases showed an aggregate revision rate of 6% in 766 implants. 4 PIP silicone arthroplasties for osteoarthritis seem to have an average revision rate of 10% to 13%.1,15,27 Our revision rate was higher at 20% with indications for surgery being instability, persistent pain, and symptomatic implant failure. We did not find any difference in revision or complication rate between digits. Specifically, the results of our study do not support the common notion that the index finger, which withstands high forces during pinch, has a higher likelihood of failure after arthroplasty. Interestingly, among preoperative demographics and comorbidities, noninsulin dependent diabetes showed to be a near significant predictor of revision surgery with an increased odds ratio of 10. This finding is similar to those of Wagner et al in metacarpophalangeal arthroplasties, who found diabetes as risk factor for periprosthetic fractures. 28
While this study is limited by retrospective design, our results support silicone arthroplasty as an effective tool for osteoarthritis of the PIP joint. Our study shows that this procedure effectively diminishes pain while preserving ROM and increasing pinch/grip strength. Patients report being highly satisfied with the procedure. Diabetic patients should be properly counseled prior to surgery as this subgroup is at risk for revision surgery.
Footnotes
Acknowledgements
The authors would like to acknowledge Denise Buyna for her assistance in coordinating this study.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study was a retrospective cohort study and does not contain any experimentation on humans or animal subjects.
Statement of Informed Consent
As this was a retrospective cohort study, no informed consent was needed to carry out this study as no individual participants were investigated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.