
Abstract
Introduction
Fractures of the distal radius are a common upper extremity presentation in the emergency department. Distal radius fractures (DRFs) account for one-sixth of all fractures seen in patients treated in the emergency department in the United States 1 and are the most common upper extremity fracture. 2 The role of concurrent injuries in patients treated for DRFs is poorly elucidated. A recent nationwide study showed that DRF patients with a recent history of myocardial infarction or congestive heart failure, dependent status, hypertension, and American Society of Anaesthesiologists (ASA) class III/IV were at significantly higher risk of complications after open reduction and internal fixation. However, concurrent fractures were not considered as a risk factor. Concurrent upper extremity fractures have been associated with worse functional recovery and a prolonged length of stay in hip fracture patients.3,4 The authors sought to determine whether concomitant remote injuries not localized to the fractured extremity were associated with worse outcomes after management of DRFs.
Materials and Methods
A retrospective cohort study of all consecutive DRFs treated at a university plastic surgery division from 2010 to 2015 was performed. Data were obtained from electronic records on patient presentation and demographics such as age, sex, obesity, smoking, hand dominance, occupation, and concurrent injuries. Radiographic imaging, patient management, and postoperative outcomes were also analyzed. Fracture pattern was classified using the AO DRF classification method, and radial height, radial inclination, and volar tilt were measured. Patients were followed up at 2 weeks, 6 weeks, 3 months, and 6 months in outpatient clinic with radiography. Outcomes measured included postoperative complications and pain scores. Complications assessed included infection, tendon rupture, contractures, malunion, and nonunion. Pain was assessed using the visual analog scale (VAS 0 = no pain, VAS 10 = severe pain). Clinic follow-ups at 2 weeks, 6 weeks, 3 months, and 6 months were reviewed. Pain level, radiographic imaging patterns of healing of the distal radius, and complications were recorded.
The data were analyzed with standard statistical methods, including frequency tables and measures of central tendency and dispersion, univariate analysis of associations with chi-square tests, and multivariate regression as appropriate. Statistical significance was reported as P < .05. All analyses were performed using SPSS version 14 (SPSS Inc, Chicago, Illinois).
Results
A total of 181 DRFs in 176 patients were treated from 2010 to 2015. Ninety-seven patients (53.6%) were female. Women were more likely to be older and men younger in keeping with the published literature, 5 as shown in Figure 1.

Age histogram by sex.
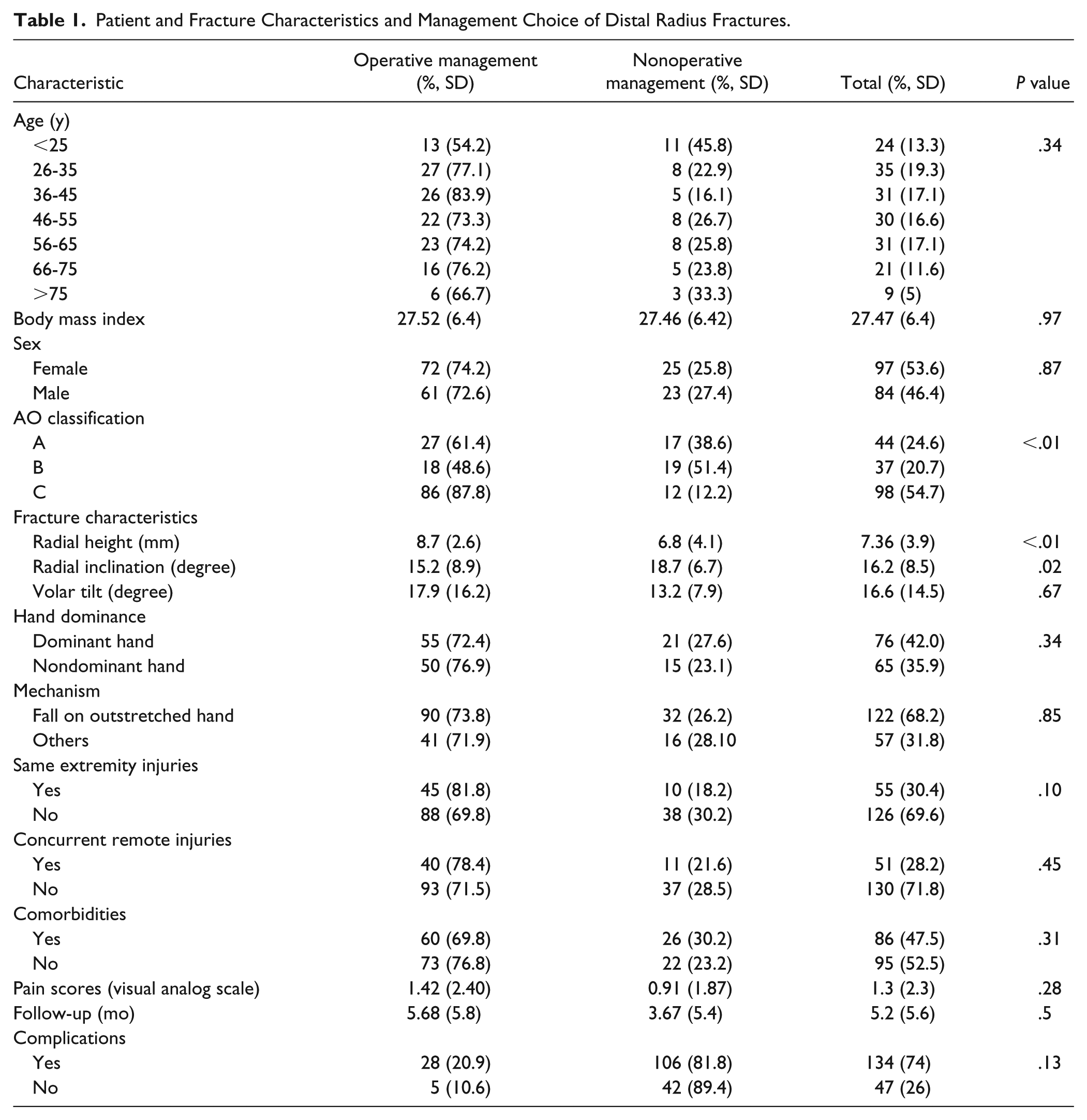
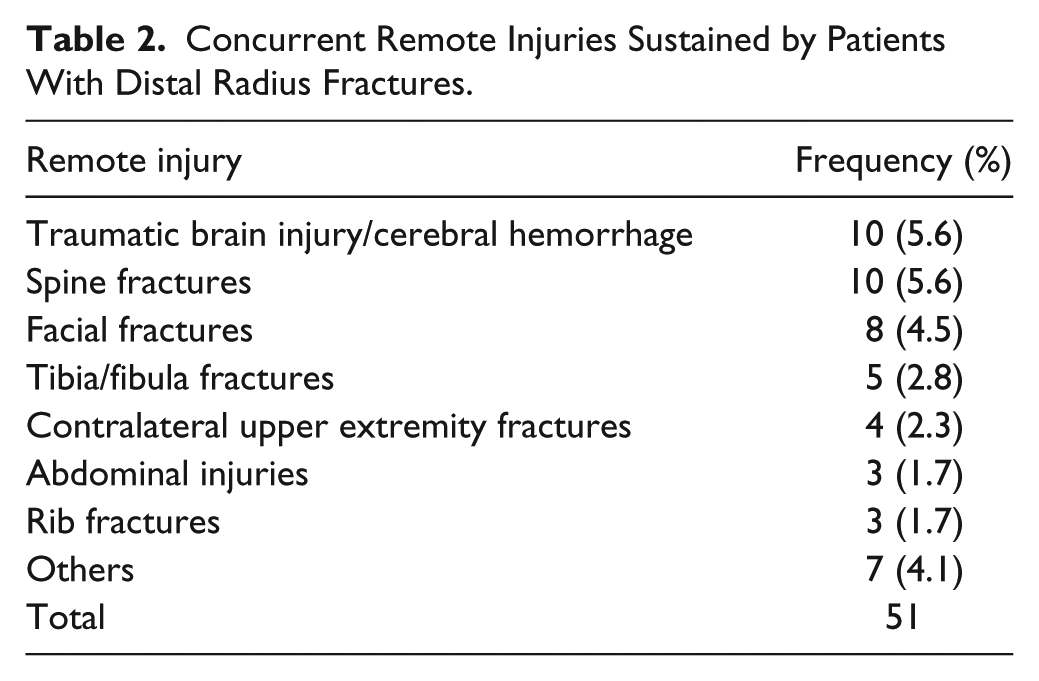
Forty-eight fractures (26.5%) were managed nonoperatively with casting, 12 (6.6%) with closed reduction and pinning, and 119 (65.7%) with open reduction and plating. One patient was treated with external fixation and pinning, and another with open reduction and pinning. The mean follow-up was 5.2 months. The complication rate was 18.2%. The majority of fractures were complete intra-articular—class C 54%, followed by classes B and A. There was no significant difference in complications between patients managed operatively and nonoperatively (P > .05) as shown in Table 1. Fracture classification and radial height were significantly associated with operative treatment. Fifty-one (28%) patients presented with concurrent remote injuries. These are listed in Table 2.
Patient and Fracture Characteristics and Management Choice of Distal Radius Fractures.
Concurrent Remote Injuries Sustained by Patients With Distal Radius Fractures.
The most common complication was persistent pain in 5 patients, followed by median neuropathy, loss of reduction, arthritis, and distal radioulnar joint instability (Table 3). After controlling for age, body mass index, hand surgeon, and other confounders, concurrent remote injury was associated with a significantly increased risk of complications (P = .04, odds ratio: 6.03, 95% confidence interval: 1.05-34.70) (Table 4)
Complications After Distal Radius Fracture Management.
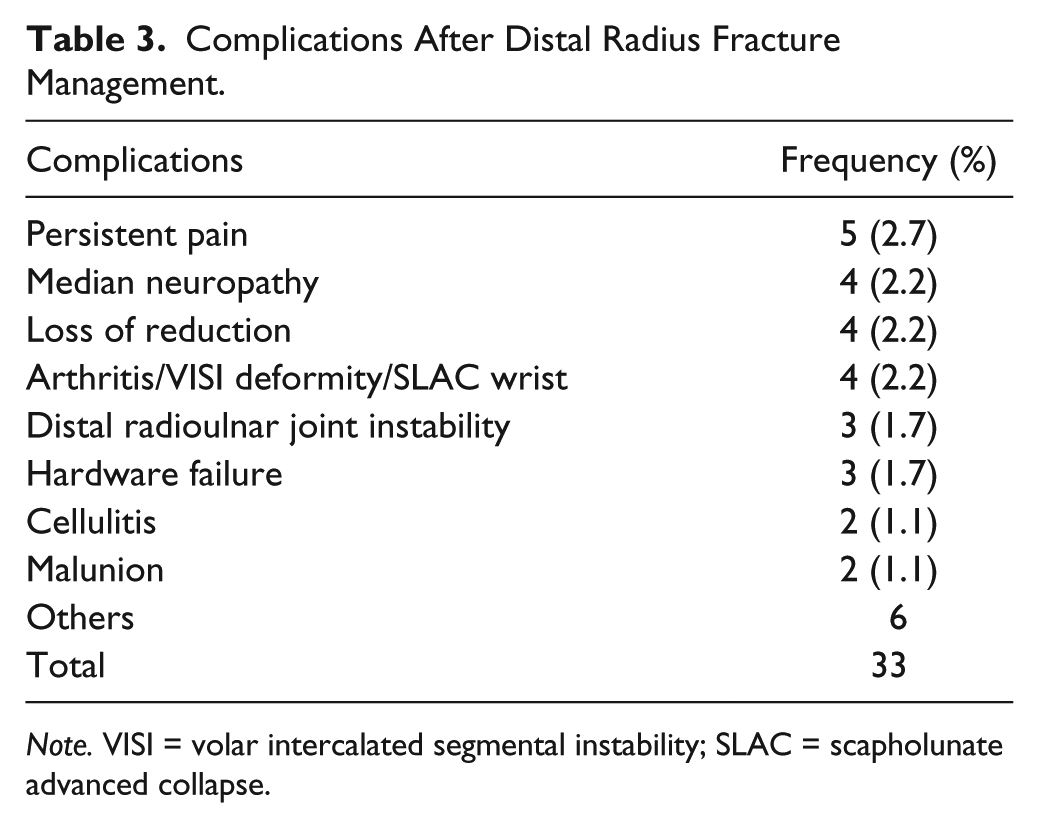
Note. VISI = volar intercalated segmental instability; SLAC = scapholunate advanced collapse.
Multivariable Analysis of Predictors of Complication After Distal Radius Fracture Management.
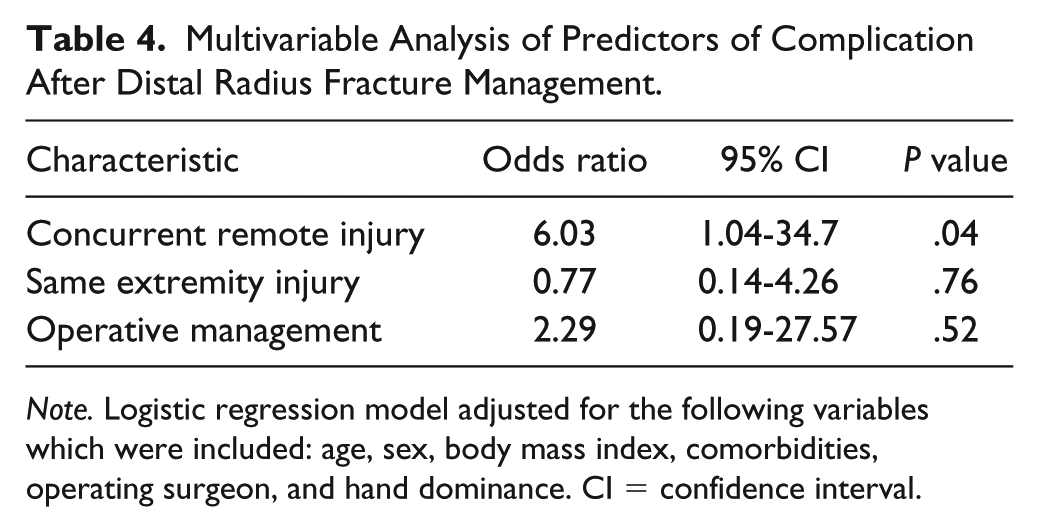
Note. Logistic regression model adjusted for the following variables which were included: age, sex, body mass index, comorbidities, operating surgeon, and hand dominance. CI = confidence interval.
Discussion
In this retrospective cohort study of all DRFs managed at an academic plastic surgery service for over 5 years, we compared complications after management in patients with and without concurrent remote injuries at the time of presentation. Our results show a 6-fold increase in complication rate among the group with concurrent remote injuries, even after adjusting for operating surgeon, method of treatment, and severity of fracture. Also, there was no significant difference in complication rates between patients managed operatively and nonoperatively.
There is a paucity of studies examining the influence of concurrent injuries on outcomes after DRF treatment. A 2014 study of 721 patients with DRFs showed longer patient stays among the 124 patients (17.2%) with any concomitant fractures, but did not evaluate any other outcomes. 6 In the study, other fractures of the same extremity as the distal radius were classified as concurrent injury. Classifying the same extremity injury as concurrent injury makes it difficult to isolate the effect of the DRF from that of the concurrent injury as the treatment of one may be influenced by the other.
A British study comparing patients with hip fractures only to those with hip and DRFs showed a longer inpatient stay in the concurrent injury group but no statistically significant difference in mortality. 4 However, the authors did not compare the patients with concurrent fractures to those with DRFs only and did not examine complications. Another retrospective matched study of 33 elderly patients with concurrent hip and wrist fractures with matched isolated hip fracture patients showed a trend toward longer hospital stay and treatment cost among the concurrently injured patients. 7 In contrast, another study of 402 patients with hip fractures did not find any statistical difference between the 22 patients with concurrent fractures when length of hospitalization, complications, in-hospital mortality, and function were assessed. 8
Di Monaco et al have also examined rehabilitation outcomes after concurrent hip and wrist injuries. An initial study found no significant difference in recovery outcome measured with Barthel index scores after treatment for hip fractures only compared with hip and upper extremity fractures. 3 However, a later study found a worse functional recovery and a prolonged length of stay in the subgroup of hip fracture patients who sustained a concomitant fracture at the proximal humerus, but not at the wrist. 9 We did not examine rehabilitation outcomes in our study but anticipate that patients with concurrent injury would have poorer rehabilitation outcomes, given the higher rate of complications in this group.
Our study had an operative treatment rate of 73%, which is higher than previously reported rates for DRFs. 10 This is likely to be due to our center’s role as a referral center for the entire state of South Carolina. As shown by the rate of class C fractures, most of our patients were those with higher severity fractures, and as such, fracture severity was the only variable associated with operative treatment in our patient population.
The main limitation of our study is its retrospective nature and the propensity for recall bias and misclassification. However, most of the variables were entered in the patient prospectively, and follow-up rates were similar for patients treated operatively and nonoperatively with more than 3 months of average follow-up in each group. Another limitation is the concern for generalizability of our findings to patients in other centers. The rate of concurrent injury in this study is similar to that found in the analysis of all Medicare beneficiaries in the United States in 2007 in the Waljee et al study (28% vs 30%), suggesting that our population resembles this national sample. 10
Our study findings suggest that the risk of complications after treatment in DRF patients with concurrent remote injuries is markedly increased, and surgeons would do well to factor this risk into patient expectation counseling, treatment decision-making, and rehabilitation protocols.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Written consent was obtained from the institutional review board of the Medical University of South Carolina (MUSC-IRB number Pro-00036447).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.