
Abstract
Introduction
Fractures of the proximal interphalangeal (PIP) joint can cause finger stiffness and loss of function and may result in symptomatic posttraumatic osteoarthritis. 1 Treatment of PIP joint fractures remains difficult. The goals of treatment are to establish a congruent joint and restore gliding joint motion.2,3 Many surgical treatments have been described, including open reduction and internal fixation,4-6 closed reduction and extension block pinning,7-9 use of an external fixator,10-14 volar plate arthroplasty,15,16 and hemi-hamate arthroplasty.17-20 No consensus exists on the optimal treatment. In general, published results are modest.
Stiffness and postoperative arthrosis are commonly reported. But the rate of reoperation after these injuries is not well understood because clinical series are small and it is difficult to amass enough patients for study. Long-term reporting is problematic because there is a large loss to follow-up. Database study supplemented by record review can capture larger cohorts of patients, which allows for statistical treatment of data and may be useful in evaluating hard clinical events such as reoperation. This approach can provide insight into whether some factors—such as comorbidities, fracture characteristics, and surgical treatment methods—affect clinical results more than others.
The purpose of the study was to determine the reoperation rate and what factors are associated with reoperation after operative treatment of PIP joint fractures.
Materials and Methods
Subjects
After institutional review board approval, we used Current Procedural Terminology codes (20900, 26740, 26742, 26756, 26776, 26785, 26535, 26536, 26860, 26861, 26862, and 26863) to identify all patients with potential operative treatment of a PIP joint fracture in our institutional database (N = 1778), followed by selecting the cases with an open or closed middle or proximal phalangeal fracture using International Classification of Diseases, Ninth Revision codes (816.01, 816.03, 816.11, and 816.13; n = 826). We included all patients with a fracture involving the PIP joint. We confirmed the diagnosis by manually reviewing the electronic records and all available radiographs. Patients were treated by 35 hand specialists at 3 urban hospitals between January 2004 and December 2015. We identified 154 patients with operative treatment of fractures involving the PIP joint. Three patients had 2 fingers with PIP joint fractures, and 2 patients had 3 fingers with PIP joint fractures (N = 161).
All data were collected from the medical records, including sex, age at the time of surgery, race, comorbidities (diabetes, smoking, and body mass index), cause of injury (specifically described as sports injury, other impact, sharp, crush, or other), affected side, fractured phalanx (proximal, middle, or both), injury severity (associated tendon, nerve, and/or vascular injury), type of surgery (open reduction, internal fixation, percutaneous pinning, hemi-hamate graft, arthrodesis, static external fixation, volar plate arthroplasty, dynamic external fixation, extension block pinning, or prosthesis), immobilization duration in days, follow-up duration in months, hospital, surgeon, reoperation, both days between injury and visit to a hand surgeon, injury and initial treatment, and reoperation. Fracture location was defined as volar, dorsal, lateral, or pilon based on radiographic or operational findings. Fracture location was defined as “other” if there was a segmental loss or a bipolar injury or another similarly difficult to classify fracture. For a few variables, such as comorbidities, dominant hand, cause of injury, and fracture type, we did not have complete data because they were not consistently recorded in the record. In these situations, we recorded and analyzed what we had available.
Radiographs
Cases for radiographic review were included for measurement when adequate lateral view radiographs were available (n = 73). All measurements were performed independently by 2 researchers, and the third researcher (an orthopedic hand surgeon) resolved any conflicts. To calculate articular involvement, fragment size, and the size of the intact surface were measured on a lateral view for volar lip fractures and on an anteroposterior (AP) view for lateral fractures. For pilon factures, the view (lateral or AP) that gave us the best representation of the fracture was used. Fragment displacement was measured by calculating the amount of fragment displacement described as a percentage of the total articular surface (Figure 1). Because the calculations were relative measures, this eliminated the need to calibrate measurements or scale radiographs. Congruency of the joint was evaluated by 3 independent reviewers who analyzed anonymized radiographs and assessed the joint for subluxation.
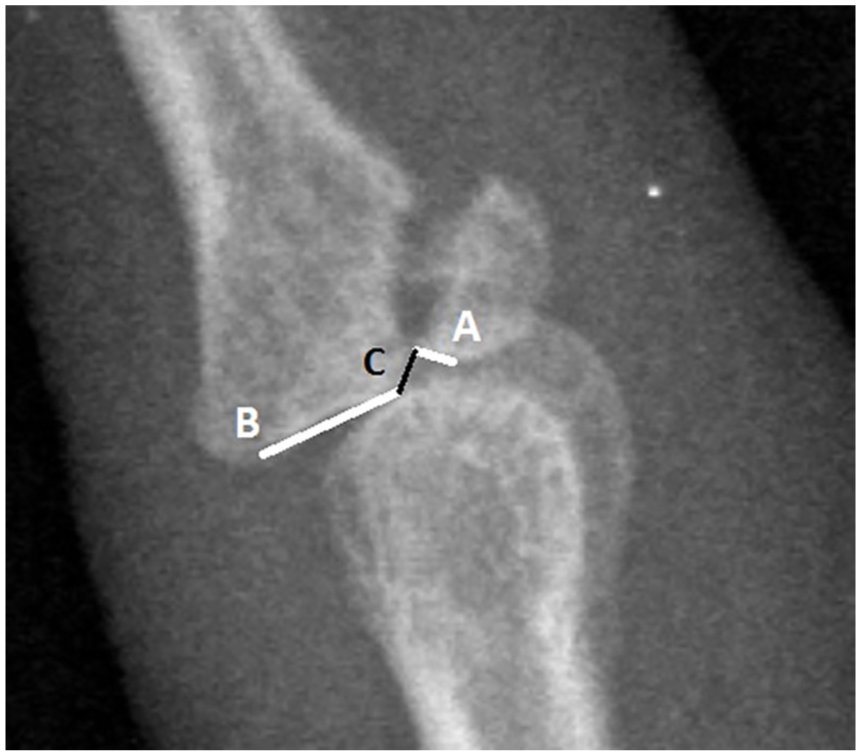
Articular surface involvement (%) is calculated by dividing the fragment size (A) by the total articular surface (A + B). Fragment displacement (%) is calculated by dividing the fragment displacement (C) by the total articular surface (A + B).
Statistical Analyses
The number and percentages of categorical variables and the mean and standard deviation (SD) of continuous variables were calculated. In bivariate analysis, Fisher exact test was used for categorical variables and Student t test was used for continuous variables. A value of P < .05 was considered statistically significant. To mitigate confounding, variables with P < .10 in bivariate analysis were inserted in a multivariable logistic regression model to identify factors independently associated with reoperation of the PIP joint fracture.
A multivariable logistic regression analysis was performed to study factors associated with residual subluxation while accounting for other variables with a P < .10 in bivariate analysis. The area under the receiver operating characteristic curve was calculated, and the Hosmer-Lemeshow test was used to assess model fit for both multivariable logistic regression models.
A subanalysis was done to assess factors associated with revision surgery of only closed fractures by performing a similar bivariate and multivariable analysis.
Demographic Data
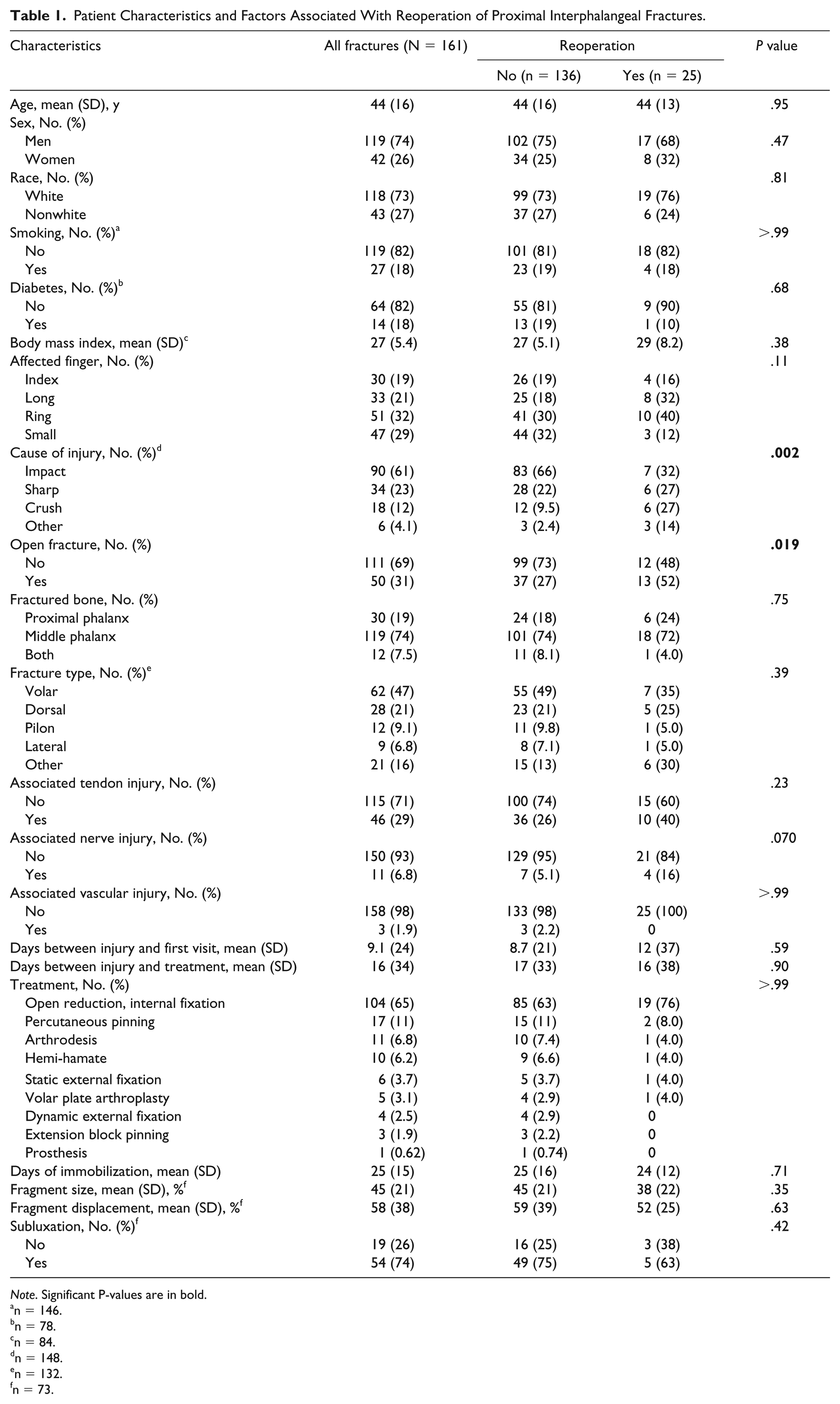
Of the 161 fingers that underwent operative treatment of a PIP joint fracture, 119 were those of men (74%). The mean age was 44 years (SD = 16; 95% confidence interval [CI] = 41-46), and most patients were Caucasian (n = 118; 73%). In 81 fingers (55%), the nondominant hand was affected. The index through small fingers were roughly equally affected. The majority of the PIP joint fractures (61%) were caused by impaction, of which 42% were sports-related. Fifty fractures (31%) were open. Open reduction and internal fixation was the most performed surgery (65%). Forty-six PIP joint fractures had an associated tendon injury, 11 had nerve injury, and 3 joints had an associated vascular injury that needed repair. Sixty-two joints (47%) had a volar base of middle phalanx fracture (Table 1).
Patient Characteristics and Factors Associated With Reoperation of Proximal Interphalangeal Fractures.
Note. Significant P-values are in bold.
n = 146.
n = 78.
n = 84.
n = 148.
n = 132.
n = 73.
Results
Of the 161 PIP joint fractures, 25 (16%) underwent reoperation (Table 1). In bivariate analysis, there was a statistically significant difference in the rate of reoperation in (1) open fractures (P = .019) and (2) the cause of injury (P = .001). Only 7 impact injuries (including 1 sports injury) underwent reoperation (7.8%), whereas 64% of the crush injuries underwent reoperation. No significant differences were seen in the measurements (fragment size and displacement) performed on the radiographs (Table 1).
In multivariable logistic regression analysis, open PIP joint fractures were independently associated with reoperation (P = .040; odds ratio = 5.7; 95% CI = 1.1-30; Table 2).
Factors Independently Associated With Reoperation of Proximal Interphalangeal Joint Fractures.
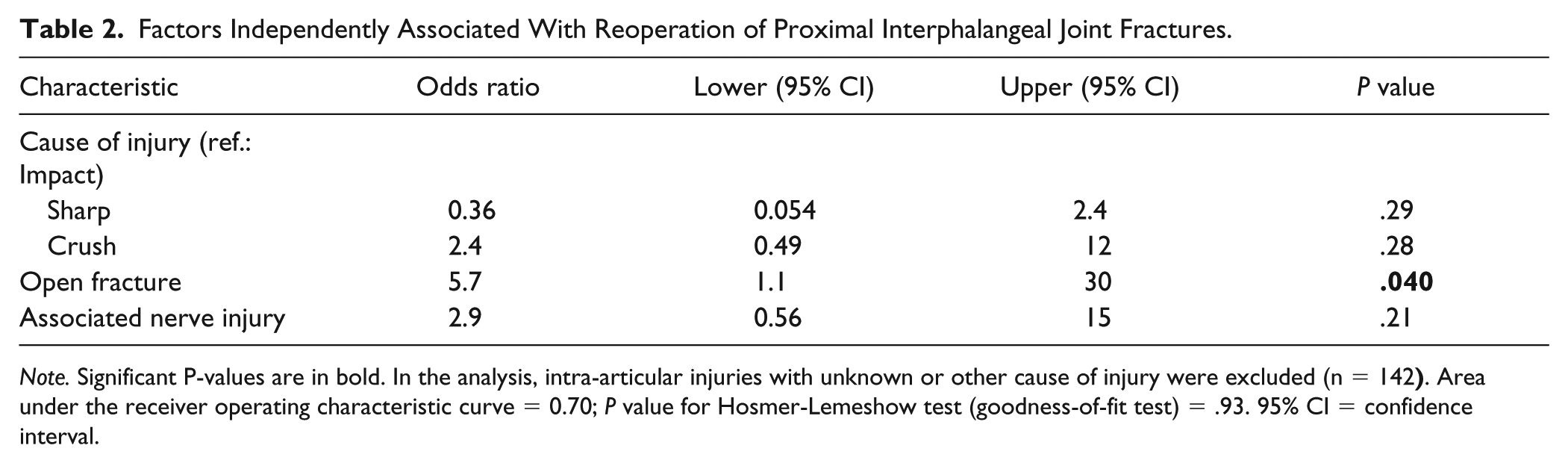
Note. Significant P-values are in bold. In the analysis, intra-articular injuries with unknown or other cause of injury were excluded (n = 142
Reoperations
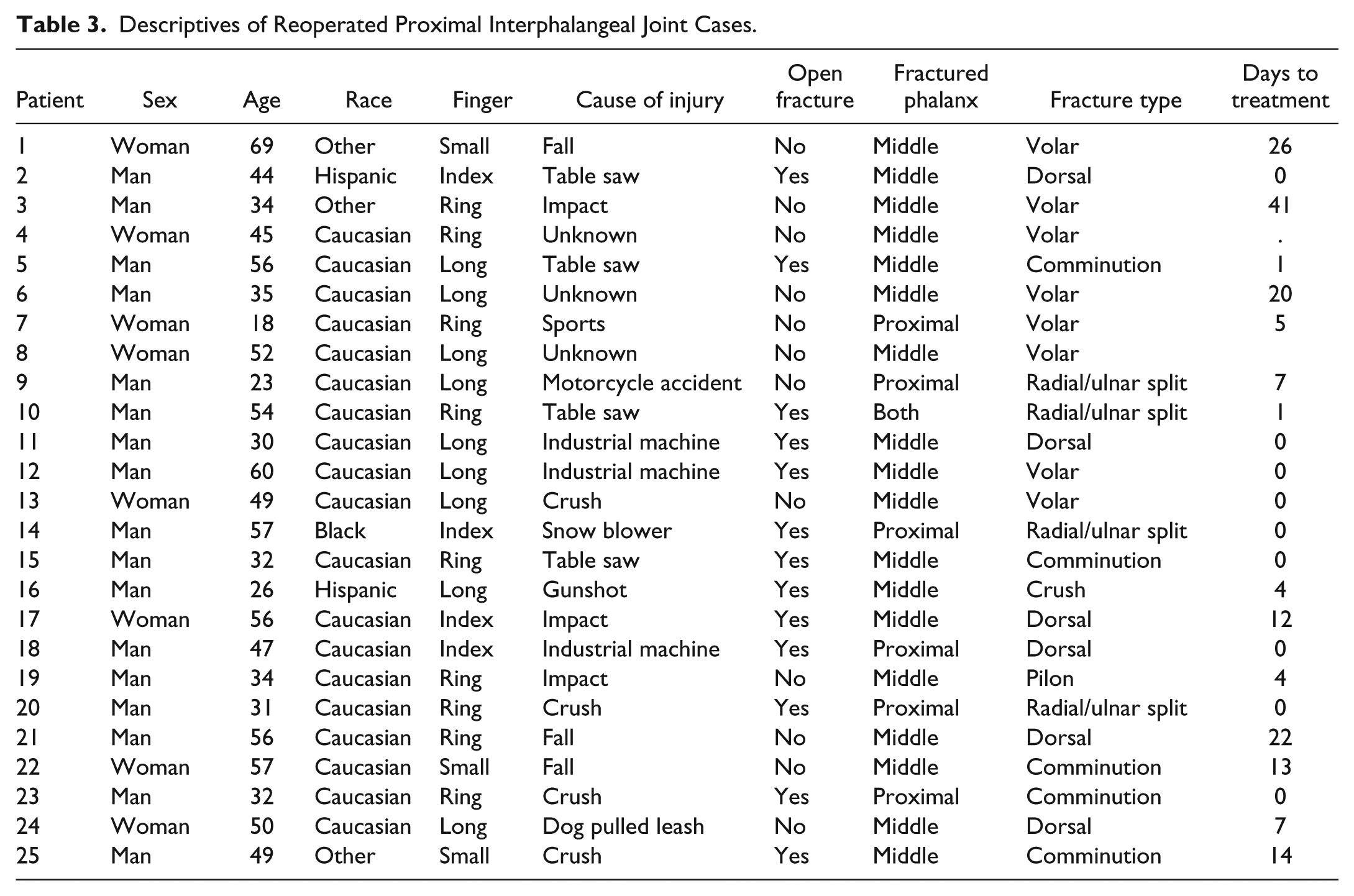
Eight (32%) of the 25 patients who underwent reoperation had more than one revision operation. The mean time to reoperation was 7.5 months. Ten patients underwent reoperation for joint stiffness. Four patients underwent reoperation for persistent subluxation. Revision surgery consisted of silicone arthroplasty in 5 patients and arthrodesis in 5 patients (Tables 3 and 4).
Descriptives of Reoperated Proximal Interphalangeal Joint Cases.
Descriptives of Reoperated Proximal Interphalangeal Joint Cases (Continued).
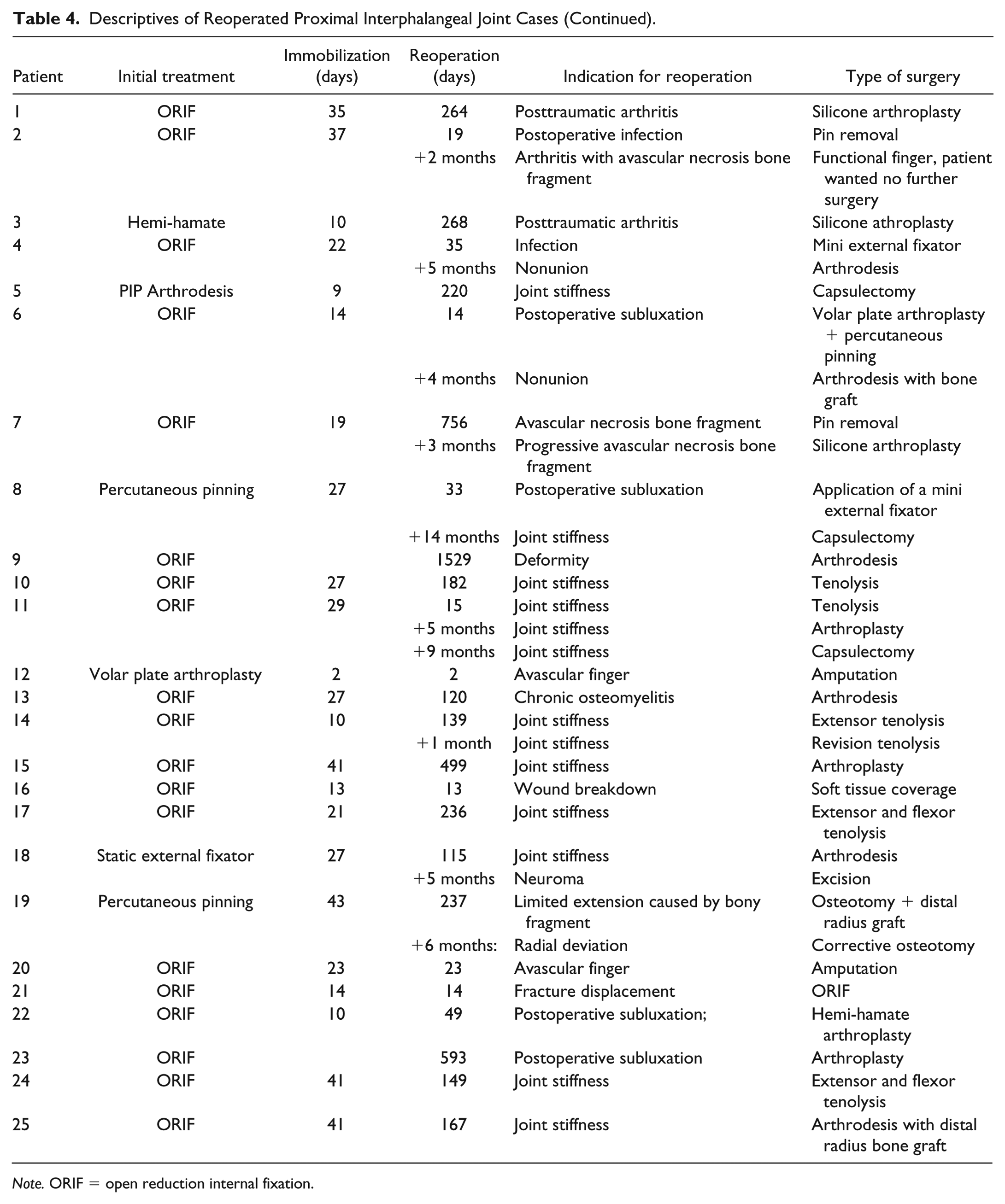
Note. ORIF = open reduction internal fixation.
Subanalysis
Twelve (11%) of 111 closed fractures underwent surgery. Affected finger and cause of injury were of borderline significance (P = .070 and P = .052, respectively; Table 5). However, in multivariable logistic regression, neither of these factors were independently associated with revision surgery (Table 6).
Patient Characteristics and Factors Associated With Reoperation of Closed Proximal Interphalangeal Fractures.
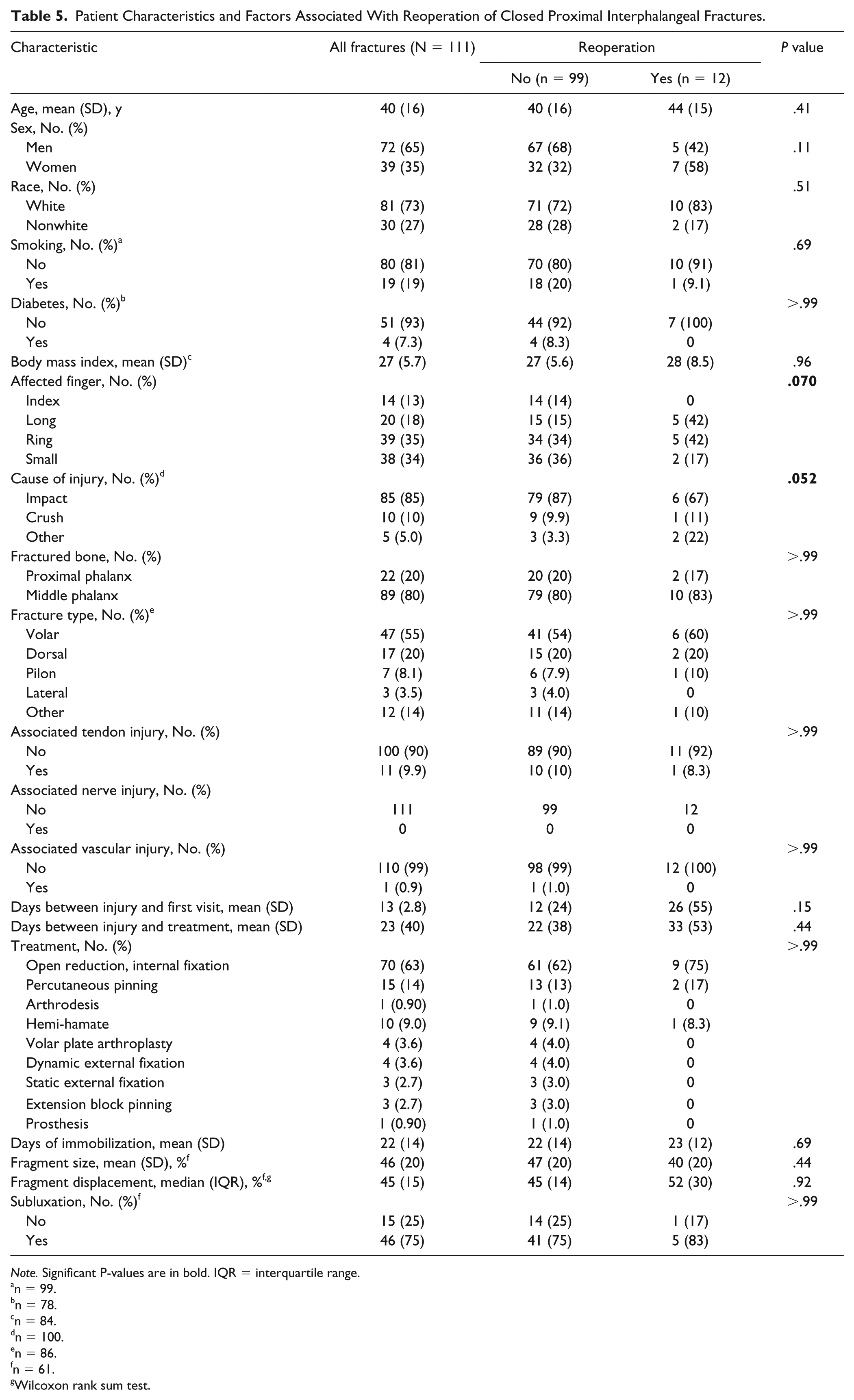
Note. Significant P-values are in bold. IQR = interquartile range.
n = 99.
n = 78.
n = 84.
n = 100.
n = 86.
n = 61.
Wilcoxon rank sum test.
Factors Independently Associated With Reoperation of Closed Proximal Interphalangeal Joint Fractures.
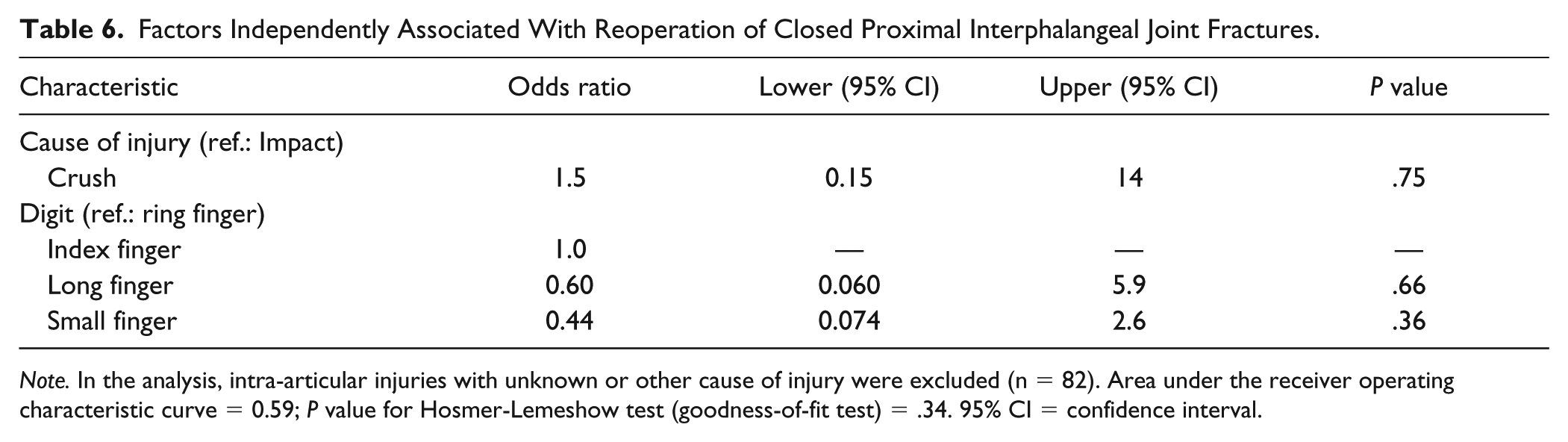
Note. In the analysis, intra-articular injuries with unknown or other cause of injury were excluded (n = 82). Area under the receiver operating characteristic curve = 0.59; P value for Hosmer-Lemeshow test (goodness-of-fit test) = .34. 95% CI = confidence interval.
Discussion
The purpose of this study was to gain insights into revision surgery after operatively treated PIP joint fractures. Overall, soft tissue injury dominates the risk of reoperation. We found a reoperation rate of 16% and that open fractures were independently associated with reoperation. No factors were associated with revision surgery of only closed fractures.
There are several limitations to this study. First, as with any database study, the results depend on coding accuracy. However, as the codes are inclusive, and all codes were verified by reviewing the medical record, we believe that we minimized these potential errors. Second, we chose to study all PIP joint fracture dislocations that presented to our institutions. This gives enough statistical power to look at general injury characteristics such as open fracture, injury mechanism, and involved digit. Third, forty-five percent of the volar fractures had adequate preoperative radiographs for quantitative measurements. We chose not to include inadequate radiographs because rotational artifact can substantially affect the results. There is no good way to standardize fracture size measurement. Although they can be helpful for identifying fracture lines, oblique views would not be standardized, and it seems that among most fractures the consistent views one can obtain are a lateral or an AP. In any quantitative radiographic study, there will be a limitation where there will be rotation of fragments. The assessment of subluxation is subjective; however, we mitigated this problem by having 3 independent hand surgeons assess subluxation. Fourth, although stiffness was the most common indication for reoperation, there was no uniform threshold stiffness for reoperation. Reoperation is dependent on patient and surgeon preference and may be influenced by insurance or workers’ compensation status.21,22 Fifth, follow-up for a database study is poorly defined. On one hand, follow-up can be defined as the time of initial treatment to final visit; on the other hand, follow-up spans the time of initial treatment to the time of database query if one assumes that most patients would present to the initial treating physician if complications arose. It is unclear how many patients sought care elsewhere. In our cohort, we found that 3 patients treated at one institution switched to the other institution, suggesting that movement between institutions is not that common and most patients continued care at the treating institution. Sixth, although this type of database study does not focus on usual patient-validated outcomes or range of motion, it allows statistical analysis of hard treatment events such as reoperation that cannot be identified by smaller cohorts focusing on usual outcome measures. Statistically significant associations are more robust than general observations, and outcomes such as reoperation have real clinical and financial impacts. The merits of careful database study should not be dismissed because of the absence of traditional metrics, and insights gained about reoperation can stand independently from validated outcome measures or range of motion data. Finally, there were a large number of surgeons included with varying degrees of experience. Some complications may be attributable to technical limitations, but on the contrary, the findings are more generalizable to hand surgery practice than a study focused on the results of a limited number of highly experienced surgeons.
Nearly one-third of all included injuries were open fractures, 26% of which underwent revision surgery. The odds of undergoing revision surgery were 6 times higher in open fractures compared with closed fractures. One patient underwent revision surgery due to postoperative infection after 19 days. Two patients had avascular digits necessitating amputation. It is reasonable to assume that open fractures are usually more severe injuries and seem to have more problems with infection and stiffness. 23 Nerve injury was a significant factor in bivariate analysis, which may represent the severity of soft tissue injury. In our study, tendon injury requiring repair and vascular injury were not significant factors associated with reoperation.
With various techniques of treating PIP fracture dislocations, joint stiffness was reported to be one of the most common complications of PIP joint injury.1,15,19,20,24,25 Stiffness of the joint was the most common indication (40%) for reoperation in our cohort. Seven patients were initially treated with open reduction internal fixation. Two of them underwent further revision surgery because of persistent stiffness. We did not find a difference in immobilization time between those who underwent reoperation compared with those who did, but we did not have power to demonstrate statistical equivalence. In contrast, Watanabe et al 26 found after operative treatment of pilon and dorsal PIP fracture dislocations that PIP range of motion after operative treatment was associated with age, time before starting motion, and involvement of an ulnar digit.
Most clinical series reporting on PIP joint fracture dislocations report a high prevalence of radiographic arthrosis. A later query of the same database may also give insight into whether the reoperation rate increases over time or remains stable. It is possible that patients with stiff but congruent joints underwent reoperation because they had a chance to improve, whereas patients with stiff but incongruent joints were primarily observed because it was unclear whether an operation for stiffness would be beneficial because the joint incongruity would dictate range of motion.
The reoperation rate after PIP joint fracture dislocation is dominated by soft tissue injury. Patients should be counseled that stiffness and persistent subluxation are common complications, and that about 1 in 6 patients undergo reoperation usually to address these issues.
Footnotes
Ethical Approval
The Institutional Review Board of our institution approved this study under protocol #2009P001019/MGH
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.