
Abstract
Introduction
Intraoperative fluoroscopy is an important tool for the orthopedic surgeon. In particular, the mini C-arm has gained popularity compared with the large C-arm due to its ability to independently operate the equipment, smaller physical size, and decreased cost. Although it is widely believed that the mini C-arm exposes the surgeon to smaller amounts of radiation, evidence is mixed.1,2 Recently, several studies have suggested that the mini C-arm subjects the surgeon to as much, if not more, radiation than the large C-arm.1,2 This is likely due to proximity to the beam in cases in which the mini C-arm is used. Although the full clinical significance of this radiation exposure remains unknown, it is well documented that the risks of radiation include malignancies, genetic abnormalities, and cataracts.3,4 Furthermore, orthopedic surgeons have been shown to be at increased risk of malignancies secondary to prolonged radiation exposure. 5
Although protective shielding is often used for the thyroid, groin, and eyes, evidence suggests that the hands receive the highest radiation exposure compared with other sites.1,2,6,7 Upper extremity surgery may pose a particularly increased radiation exposure to the surgeon’s hands in that manual positioning of the extremity is often required to obtain adequate imaging. Various methods of shielding the hands from radiation exposure are currently available and generally fall into 1 of the 2 categories: radiation-attenuating gloves and creams applied directly to the hands under standard surgical gloves. Despite evidence that protective gloves reduce hand exposure,2,8 widespread adoption has not been observed. Furthermore, to the authors’ knowledge, no study has attempted to directly compare the radiation-attenuating effects of the various hand-shielding options.
The purpose of the current study was to evaluate the degree to which radiation exposure to the surgeon’s hands is decreased with various commercially available shielding products.
Materials and Methods
Institutional review board approval was not necessary as no living subjects or patient medical records were studied.
Model Position
An anthropomorphic surgeon model (MD-HMB2FK; Roxy Display, Inc., East Brunswick, New Jersey) was used to simulate a surgeon sitting at a stand-alone hand table (Figure 1). Model placement was standardized in all tests performed in the study. A sawbones model of a patient’s wrist with a distal radius volar plate (2.4 mm LCP; Synthes, Paoli, Pennsylvania) was supinated and placed in the center of the hand table. The surgeon model’s hands were placed proximal and distal to the plate such that the index distal phalanges were separated by 15 cm and were equidistant to the crosshair laser projection that marks the center of the radiation beam. Neither hand was directly visible in the beam in any test. All distances were measured prior to performing each arm of the study with a metal ruler.
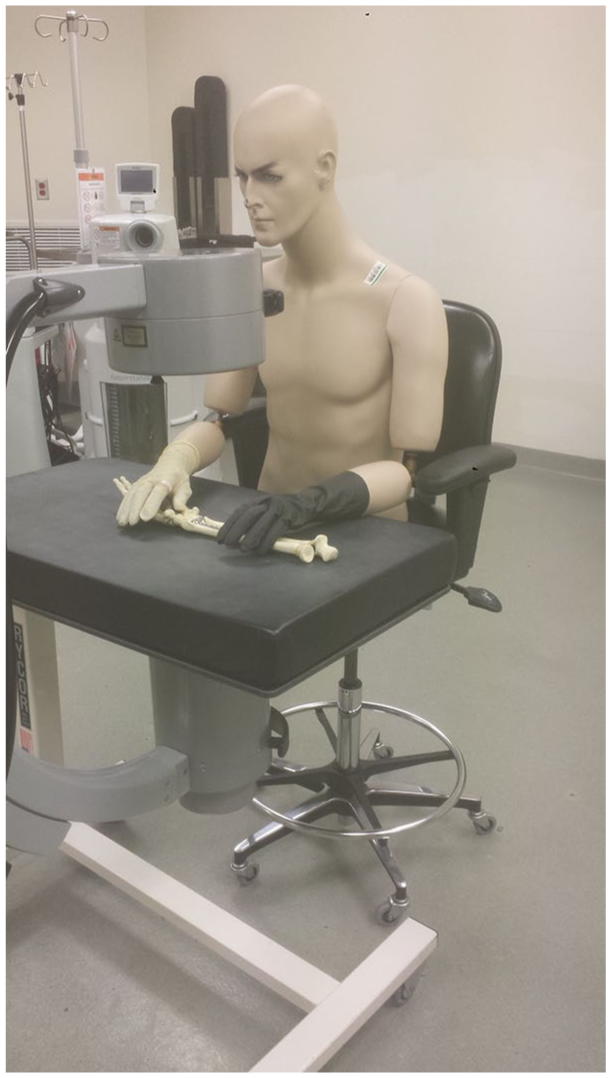
Experimental setup with anthropomorphic surgeon model.
Protection and Dosimeter Placing
Six different radiation-attenuating shielding options were examined (Figure 2). In all arms of the study, the right side served as the control side, and the right index finger dosimeter was placed on the proximal phalanx beneath a single polyisoprene surgical glove (Protexis PI; Cardinal Health, Waukegan, Illinois). The left side served as the study side, and the index finger dosimeter was placed beneath the proximal phalanx:
Two standard polyisoprene surgical gloves (double glove);
A single lead-free, metal-oxide glove with 0.18 mm fingertip thickness (Radiation Attenuating Surgical Gloves; International Biomedical, Austin, Texas);
A single lead-free, metal-oxide glove with 0.35 mm fingertip thickness (Attenuator-X; Shielding International, Madras, Oregon);
A single leaded glove with 0.20 mm fingertip thickness (Revolution Light; Infab Corporation, Camarillo, California);
A single leaded glove with 0.32 mm fingertip thickness (Revolution Medium; Infab Corporation); and
Radiation-attenuating cream applied (Ultrablox; BLOXR Solutions, Salt Lake City, Utah) and covered with a standard polyisoprene surgical glove.
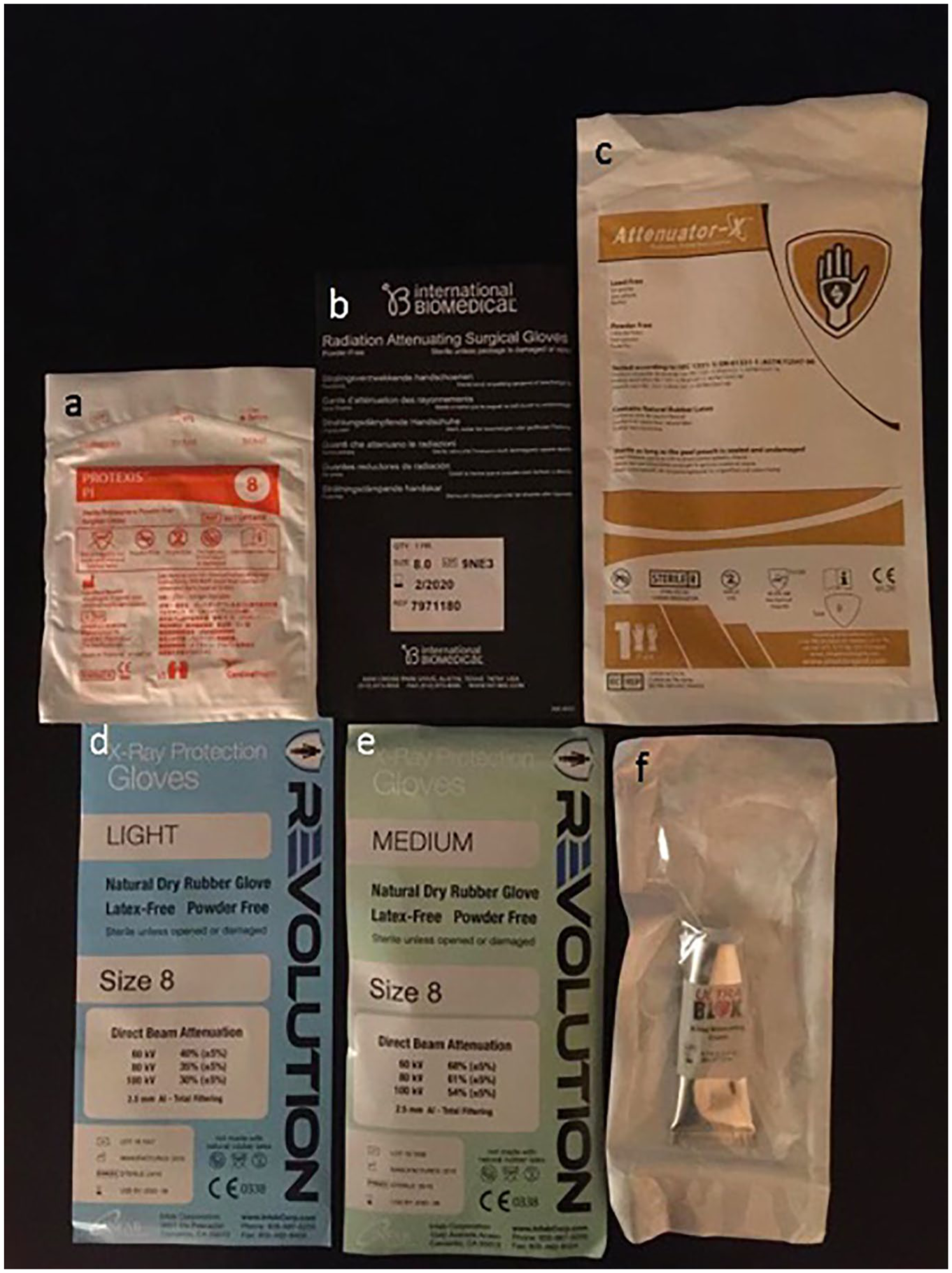
Hand-shielding products.
All gloves in the study were size 8. The cream was applied directly to the mannequin hand as per the manufacturer’s specifications.
Fluoroscope Position
The same mini-C arm (HD 1000-0004; OrthoScan, Scottsdale, Arizona) was used and positioned identically in all arms of the study. The fluoroscope was configured vertically with the source 25 cm above the sawbones model. The device was set to 60 kVp, given the typical voltage for imaging at our institution ranges between 50 and 60 kVp. The current linked automatically to voltage levels at 0.074 mAs. Each test scanned the distal radius for 15 continuous minutes. This time period was necessary to produce sufficient radiation for measurement with the dosimeters. Based on a mean fluoroscopy time of 60 seconds at our institution for a volar distal radius plating procedure, this time period represents the cumulative exposure of approximately 15 surgical cases requiring fluoroscopy. Each comparison was run 3 times and then averaged for statistical comparison.
Statistical Analysis
Descriptive statistics were performed including unpaired t tests.
Results
The results of the average of 3 runs for each comparative bilateral hand irradiation are tabulated in Table 1, including average, range, and t-test statistical significance. The right hand (control arm) had a single polyisoprene surgical glove as a control, and the average radiation exposure absorbed by the dosimeter was 44.8 mrem (range, 30-54; SD = 9.2 mrem). In contrast, the experimental arm using the various radiation-attenuating options averaged a radiation absorption by the dosimeter of 18.6 mrem (range, 14-26; SD = 4.7 mrem).
Radiation Exposure for the Each Test in the Study.
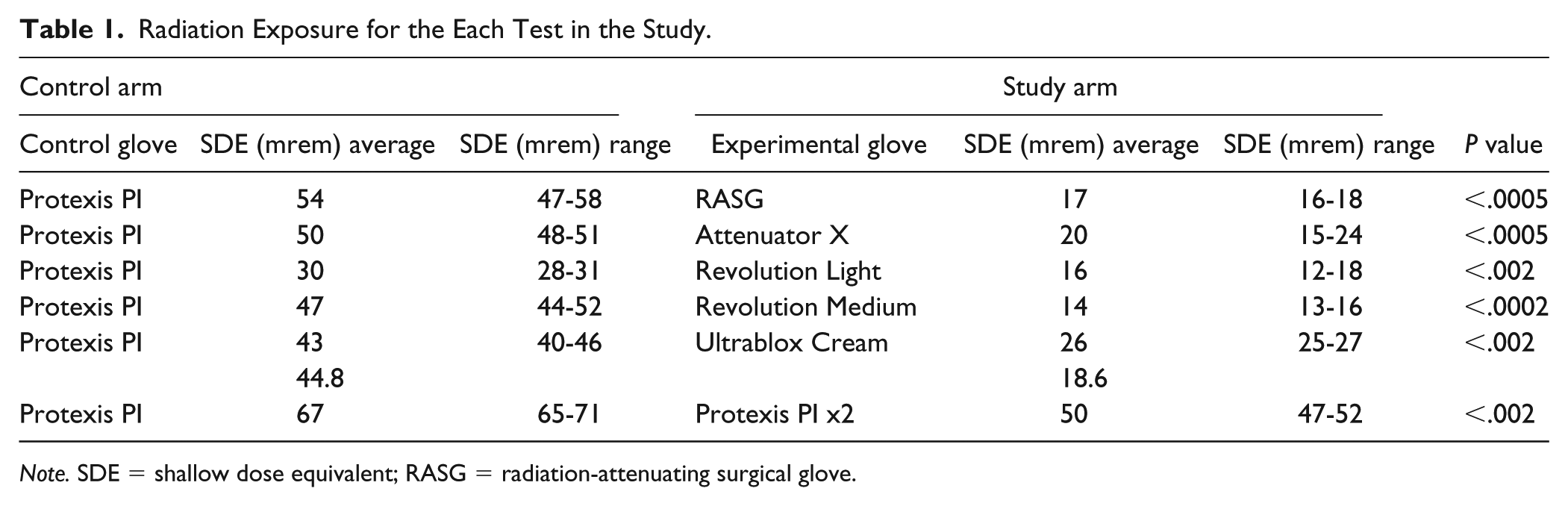
Note. SDE = shallow dose equivalent; RASG = radiation-attenuating surgical glove.
Moreover, each radiation-attenuating option was found to result in statistically significant lower radiation absorption than a single polyisoprene surgical glove. Interestingly, even double-gloving a standard polyisoprene surgical glove resulted in a decrease in radiation exposure from 67 to 50 mrem, relative to a single glove (last column of Table 1). However, even double-gloving (50 mrem) still resulted in more radiation exposure than all other radiation-attenuating options individually (range, 14-26 mrem).
Discussion
The literature is replete with studies demonstrating the effects of ionizing radiation and includes genetic instability, malignancies, cataracts, dermatologic conditions, and delayed wound healing.3,4,9-11 The International Commission on Radiological Protection (ICRP) sets annual dose limit guidelines for occupational radiation exposure at various anatomical sites.12,13 The basis for these recommendations comes from observations from prior exposure events, including atomic bomb survivors, nuclear accident survivors, and medical exposures. This methodology relies on extrapolating data from high-dose single-event radiation exposures to long-term low-dose occupational exposures.
The ICRP currently recommends a maximum of 50 rem of occupational radiation exposure to hands annually. 13 Although multiple recent studies have highlighted the increased level of radiation exposure to surgeon’s hands,2,6 the data suggest that it would be challenging to approach the recommended annual dose limits. The effects of consistently high, but submaximal, radiation exposure are not known. There are 2 main hypotheses with respect to the deleterious effects of radiation exposure. The first is that there is a threshold phenomenon, and only upon crossing the threshold are detrimental effects observed. The second is that damage incurred by radiation exposure is cumulative over a lifetime and cannot be reversed.1,14,15 The latter theory is of potential concern to the orthopedic surgeon in which consistently high, submaximal, doses are experienced annually over the course of a multidecade career.
Several recent studies have emphasized the high levels of radiation exposure to the orthopedic surgeon’s hands. Singer 6 evaluated the radiation exposure to 5 surgeon’s hands across 81 procedures distal to the wrist that involved mini C-arm fluoroscopy. He showed that the hands were exposed to an average of 20 mrem/case, which was significantly higher than the fluoroscope manufacturer predictions and was the equivalent of 1 chest radiography to the hands per case.
Another recent, prospective, intraoperative study compared the surgeon’s hand exposure between the large and mini C-arms. 1 The average hand exposure was 5 mrem/case in those in which the large C-arm was used and 11 mrem/case for those using the mini C-arm. The authors conclude that in a practical setting, the mini C-arm may not be a safer alternative to the large C-arm as previously believed.
In a simulated distal radius model, Hoffler and Ilyas 2 found that hand radiation exposure was not significantly different between the mini and large C-arms and was 13 times higher than exposure at other anatomical sites, including the eye, thyroid, chest, and groin. The authors recommend the routine use of protective equipment for the hands in cases in which fluoroscopy is used.
Although many commercial radiation-attenuating hand-shielding options are available, their widespread implementation has not been observed. The underuse of these products is likely multifactorial in nature. Many surgeons may be unacquainted with these options and/or may find them inconvenient. Other possible reasons include the belief that protection is unnecessary due to current dose limit guidelines as well as concerns over product cost and loss of manual dexterity and fine touch.
Multiple studies have shown the efficacy of different hand-shielding options. Wagner and Mulhern 8 evaluated 4 different types of radiation-attenuating gloves. These included 2 lead-based, 1 tungsten-based, and 1 “unknown proprietary” material. They reported a large variation in exposure reduction, from 7% to 48%, depending on the glove and energy level of the beam. The authors maintain that keeping hands out of the direct beam should be the primary means of decreasing hand exposure.
Hoffler and Ilyas 2 showed a nearly 70% reduction in hand exposure with the use of a single radiation-attenuating glove (RayShield Radiation Resistant Glove X-1; AADCO Medical, Randolph, Vermont). The hands were the only anatomical site in their study in which the protected dosimeter showed a statistically significant reduction in exposure.
The current study looks to expand on these prior findings and determine the degree to which various commercially available hand-shielding options decrease hand radiation exposure. We present a model of surgeon exposure during volar plate fixation of a distal radius. The fluoroscope configuration used is typical for distal radius fracture surgery. Although some surgeons use alternative configurations, which can influence radiation exposure, the current report focused on the effect of hand-shielding equipment in a single configuration.
Radiation-attenuating gloves generally fall into 2 main categories based on production material: lead-based and metal-oxide–based. Within these categories, gloves are manufactured with increasing fingertip thickness. We chose to study gloves from both categories and selected various thicknesses that would represent those used by a hand surgeon. Although dexterity with these gloves is a concern, and may be influenced by glove thickness, subjectively the authors believe that many of the gloves evaluated in this study would be adequate for everyday surgical use. Objective satisfaction is beyond the scope of this report.
To our knowledge, there is only one manufacturer of radiation-attenuating cream. The cream is primarily composed of a bismuth oxide ceramic powder and either may be applied directly to the hands and covered with a sterile glove or may be applied on top of a sterile glove and covered with a second glove. It carries the theoretical advantage of minimizing the concern for dexterity and loss of tactile sensation experienced with the gloves.
As previously noted, one of the concerns likely limiting the use of hand-shielding options is product cost. The average cost per pair of radiation-attenuating gloves in the present study was $38. Similarly, the cost of the radiation-attenuating cream was $41 per tube, which provides enough products for one surgical case. This compares to approximately $5 per pair of standard latex surgical gloves that was used as the control. The cost for these options has the potential to decrease with bulk purchasing but would still represent a substantial cost increase over nonshielding options and may potentially be prohibitive for surgical centers.
The current study showed a wide range of radiation exposure in the control arm (mean, 48.5 mrem; range, 30-67 mrem). There are several factors that may contribute to this variation. There is the possibility of variability in the setup. The ruler used to confirm the testing conditions was accurate to 1 mm. Even small variability in the setup can have profound impact on the radiation exposure when the measurement is at the immediate edge of the fluoroscopic beam. The testing conditions may also produce inconsistent scatter from the hand table, the sawbones/plate construct, and the opacity of the radiation-attenuating study arm. Despite this variation, the mean output of the control group in the current study (48.5 mrem) compares favorably with the mean dose to the hand in a prior study (46.5 mrem) performed by Hoffler and Ilyas 2 with identical model position, sawbones model, and dosimeter placement.
This study has some limitations. Only 1 configuration of the mini c-arm unit was used. Radiation to surgeon’s hands has been shown to differ based on fluoroscopy configuration. Furthermore, different placement of the hands in relation to the source and receiver may influence the attenuating properties of the products. The model’s hands in this study were placed in a clinically relevant but static position that may not mimic actual surgical conditions, but afforded consistency of comparison and analysis. Only 1 mini c-arm unit was used, and all tests were run at a single power setting. While this provided a control across the study, different c-arms may emit variable amounts of radiation. Finally, in vivo scatter may influence exposure rates differently than in this sawbones study.
Standard precautions should be practiced when using intraoperative fluoroscopy to minimize radiation exposure to the hands, including altering fluoroscopic and surgeon position, limiting radiation intensity and overall exposure time, and ensuring the hands remain out of the direct beam. This study showed that radiation-attenuating hand-shielding options decreased exposure by up to 70% (average, 59%; range, 25%-70%). All hand-shielding options decreased hand exposure relative to the control. These products represent a simple method to further protecting the surgeon from intraoperative radiation exposure.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Patients were not enrolled in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.