
Abstract
Introduction
Volar plating for distal radius fractures is an established and common surgical technique for fixation of both extra-articular and intra-articular distal radius fractures. The pronator quadratus (PQ) muscle covers the volar aspect of the distal radius. This muscle serves as a critical landmark during deep surgical dissection. Multiple techniques ranging from complete muscle detachment to minimally invasive partial detachment exist to access the fracture site deep to the PQ to perform internal fixation. The most distal identifiable structures in this dissection are the volar wrist ligaments, which insert on the most distal portion of the volar aspect of the radius. There is no literature, to our knowledge, regarding the anatomical relationship between these ligaments and the PQ. Furthermore, there are a paucity of data regarding the consequences of injury to the volar wrist ligaments during volar locked plating.
Anatomical studies have described ligaments of the wrist in 2 groups, extrinsic and intrinsic. 1 The extrinsic ligaments connect the distal radius and ulna to the carpal bones, whereas the intrinsic ligaments serve as a connection between the carpal bones. For the purpose of this study, we focused on the volar extrinsic ligaments, which include the radioscaphocapitate, the long radiolunate, and the short radiolunate ligaments. It is generally accepted that the volar ligaments in combination with the dorsal wrist ligaments play the key role in wrist stabilization. 2 Therefore, it can be inferred that disruption of these structures may lead to carpal instability.
We identified the PQ as a constant anatomical landmark used by most surgeons during volar locked plating for distal radius fractures, among other indications. The origin of the volar wrist ligaments on the distal radius has not been well studied. Thus, we seek to evaluate the relationship between the volar wrist ligaments and the distal border of the PQ.
Materials and Methods
Thirteen embalmed cadaveric hands were included. For each hand, a standard flexor carpi radialis (FCR) volar approach was used. The FCR was bluntly dissected free and retracted to reveal the PQ. Care was taken to remove surrounding fat and connective tissue to visualize the entirety of the PQ muscle, including its insertion. Then, the FCR was released from its fibro-osseous tunnel to identify the volar wrist capsule and the ligaments.
Once the radius had been exposed, the midpoint between the radial and ulnar border of the radius was identified (Figure 1). At this point, the proximal insertion of the volar wrist ligaments was visually demarcated. If there was difficulty determining the insertion point visually, an 18-gauge needle was used to facilitate its identification. Beginning just distal to the midpoint between the radial and ulnar border of radius, a needle was inserted into the radiocarpal joint. By aiming dorsal and perpendicular to the longitudinal axis of the bone, we identified the radiocarpal joint. Then, the needle was slowly marched proximally until the needle was directly on bone without any intervening ligaments, which was determined by a change in tissue character.
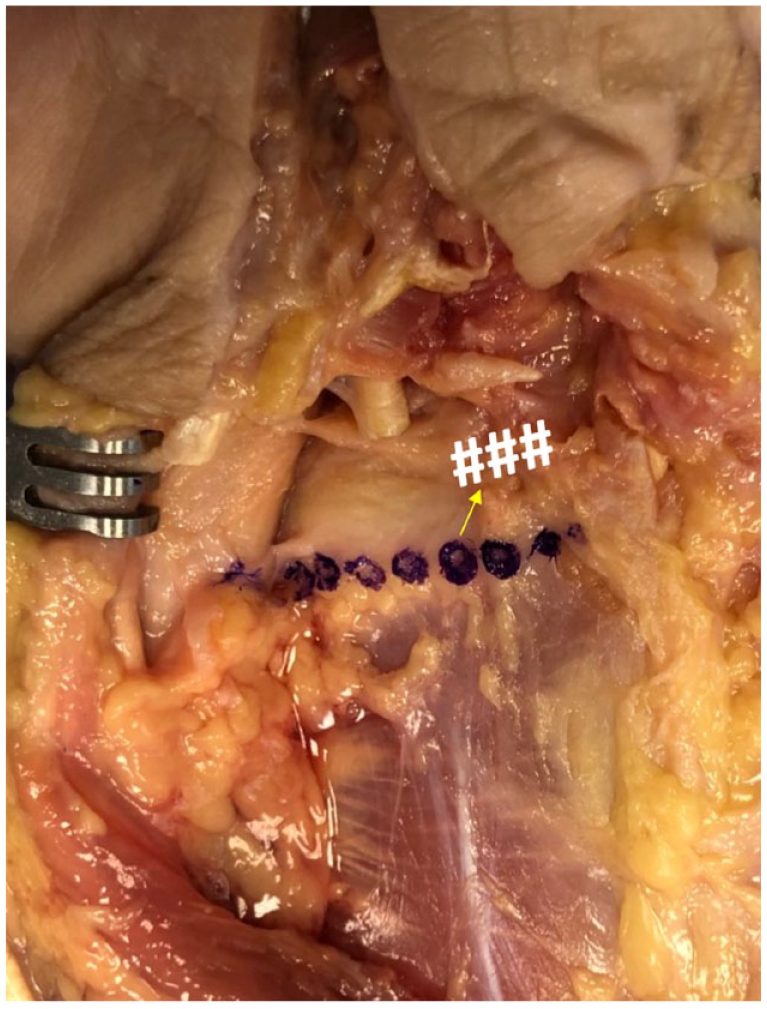
Cadaveric wrist dissection through a flexor carpi radialis approach. Distal border of the pronator quadratus is indicated by purple dots. The ### show the insertion of the volar wrist ligaments. The arrow indicates measured distance between the two.
The distance between the distal edge of the PQ and the proximal insertion of the volar wrist ligaments was measured with a ruler and recorded. This process was then repeated for every cadaveric hand.
Internal review board approval is not required for cadaveric studies at our institution.
Results
The average distance between the distal border of the PQ and the proximal insertion of the volar wrist ligaments was 5 mm, ranging from 3 to 7 mm, with a standard deviation of 2 mm.
Discussion
In this cadaveric study, we found the distance between the distal PQ and the proximal volar wrist ligament insertion to be quite close. Subperiosteal stripping distal to the PQ muscle can potentially disinsert the proximal origin of the volar wrist ligaments. It is therefore important to avoid significant subperiosteal stripping of the radius distal to the insertion of the PQ.
The volar wrist ligaments are crucial to maintaining appropriate carpal biomechanics. They have been shown to provide 61% of the restraint to the dorsal translation of the carpus and 48% to the palmar translation of the carpus when compared with dorsal ligaments. 2 They also provide a key restraint to ulnar subluxation of the carpus. Thus, it is not surprising that traumatic rupture of the ligaments can lead to carpal instability. 3 One study by Kamal and Ruch 4 suggests that postoperative scarring of the volar wrist ligaments after volar plating in distal radius fractures may lead to limitations in wrist extension. Ulnar translation of the carpus is a difficult problem to repair following open reduction internal fixation of distal radius fractures and is potentially initiated by compromise of the volar wrist ligaments. 5 Thus, quantifying the distance between the proximal origin of the volar wrist ligaments and a stable anatomical landmark, such as the distal extent of the PQ muscle, would be helpful for practitioners desiring to avoid disruption of the volar wrist ligaments.
This study has limitations. The preservation technique of the cadavers may have distorted the native anatomy, although care was taken during dissection to obtain the most accurate measurements. The number of specimens is also small, and a large-scale study could help confirm our results. We also did not have demographic data available for the cadavers used in this study, which could have been used to analyze results by age and sex. We also did not measure the distance from the articular surface of the radius to the proximal origin of the volar wrist ligaments. In future anatomical and biomechanical studies, the longitudinal width of the volar wrist ligament insertion on the distal radius and the amount of disruption before instability will be investigated.
Conclusion
In this study, we describe the distance between the distal edge of PQ and the proximal origin of the volar wrist ligaments. Subperiosteal stripping of the tissues distal to the PQ should be judicious to preserve the volar wrist ligaments. Further research to evaluate the clinical significance of such disruption is warranted. We believe that an understanding of this anatomical relationship will be useful to surgeons when repairing distal radius fractures.
Footnotes
Acknowledgements
The authors would like to thank those who made this study possible through contributing their bodies to science. We express our sincere gratitude and appreciation for the privilege of learning from these individuals.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This cadaveric study was carried out to a high ethical standard.
Statement of Informed Consent
No consent was needed for this cadaveric study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.