
Abstract
Introduction
Perioperative pain control is important to both patients and surgeons, and the current opioid epidemic highlights the need for pain management strategies to decrease or eliminate the use of opioid medications in the perioperative period. Administration of antiinflammatory agents perioperatively has been shown to lower pain scores and reduce opioid consumption in the immediate postoperative period after various orthopedic procedures.1-3 A multimodal approach to pain management can also decrease the likelihood of admission and length of hospitalization 4 and has become widespread in other orthopedic fields.
However, the efficacy of perioperative intravenous (IV) acetaminophen and/or ketorolac in hand surgery is not well studied. An increasing amount of literature is being produced regarding multimodal strategies for perioperative pain control, specifically regarding upper extremity procedures, but there is no current standard of care for intraoperative therapies. Surgeries are much less invasive than in other orthopedic subspecialties, so patients likely have less postoperative pain. Both IV acetaminophen and ketorolac have relatively low-risk safety profiles, but if these medications do not improve perioperative pain and opioid use in the hand surgery population, then the risks of the medications, albeit rare, may not outweigh the potential benefits.
The purpose of this study was to determine if perioperative administration of IV acetaminophen and/or IV ketorolac decreases postoperative pain and opioid consumption after endoscopic carpal tunnel release. We hypothesize that there is no difference in postoperative pain or opioid consumption for endoscopic carpal tunnel release after the perioperative administration of IV acetaminophen and/or IV ketorolac.
Materials and Methods
This study was randomized, double-blind, and placebo-controlled. It was approved by our local institutional review board, PRO14110464, and registered with Clinicaltrials.gov, NCT02313675. Patients were recruited from the clinical practice of the senior author and enrolled in the study if they consented to undergo endoscopic carpal tunnel release. The following exclusion criteria were used: current pregnancy, allergy to acetaminophen or ketorolac, medical contraindication to acetaminophen or ketorolac, preoperative/current use of opioids, history of IV drug abuse, and workers’ compensation.
The Investigational Drug Service (IDS) at our institution randomized subjects using a blocked computerized randomization protocol. The 4 treatment arms were as follows: placebo (Group 1), IV acetaminophen (Group 2), IV ketorolac (Group 3), or both IV acetaminophen and IV ketorolac (Group 4). The dose of IV acetaminophen was 1000 mg, and the dose of IV ketorolac was 10 mg. All patients and the surgeon were blinded to the medication given, as IDS dispensed the medications in opaque syringes. The medications were administered 5 minutes prior to skin incision.
All patients were treated according to the same protocol for intraoperative anesthesia and pain control. Patients were placed under sedation by the anesthesiologist using a standard weight-based dose of propofol and maintained on light sedation using a standard weight-based titration of propofol. After adequate sedation, the senior author injected a mixture of 5 mL of lidocaine 1% without epinephrine and 5 mL of bupivacaine 0.5% without epinephrine into the surgical field for intraoperative procedural anesthesia. All carpal tunnel releases were performed using a single incision endoscopic technique.
All patients received the same postoperative prescriptions for pain management: acetaminophen 1000 mg by mouth every 8 hours, naproxen 500 mg by mouth every 12 hours, and oxycodone 5 mg by mouth every 6 hours as needed for severe pain rated as more than 7 out of 10 on an 11-point pain scale (0-10). Each oxycodone prescription was for 20 tablets with no refills. Patients received pain surveys on the day of surgery, and they were instructed to complete the surveys every 8 hours for 7 days after surgery. Patients were also instructed to record the number of oxycodone tablets they consumed each day.
An a priori power analysis determined that 11 subjects per treatment group were required (total of 44 patients) to detect a difference in the 11-point pain score of 1.0 between groups. Data analysis included calculation of descriptive statistics with frequency counts and percentages for categorical variables and measures of central tendency (means, medians) and dispersion (standard deviations, ranges) for continuous variables. Analysis of variance and Kruskal-Wallis tests were used to compare mean pain scores and opioid consumption between groups.
Results
A total of 58 patients were screened from October 2015 to April 2017 to enroll 44 in the study (Figure 1). There were no differences among groups with respect to age and sex (Table 1).
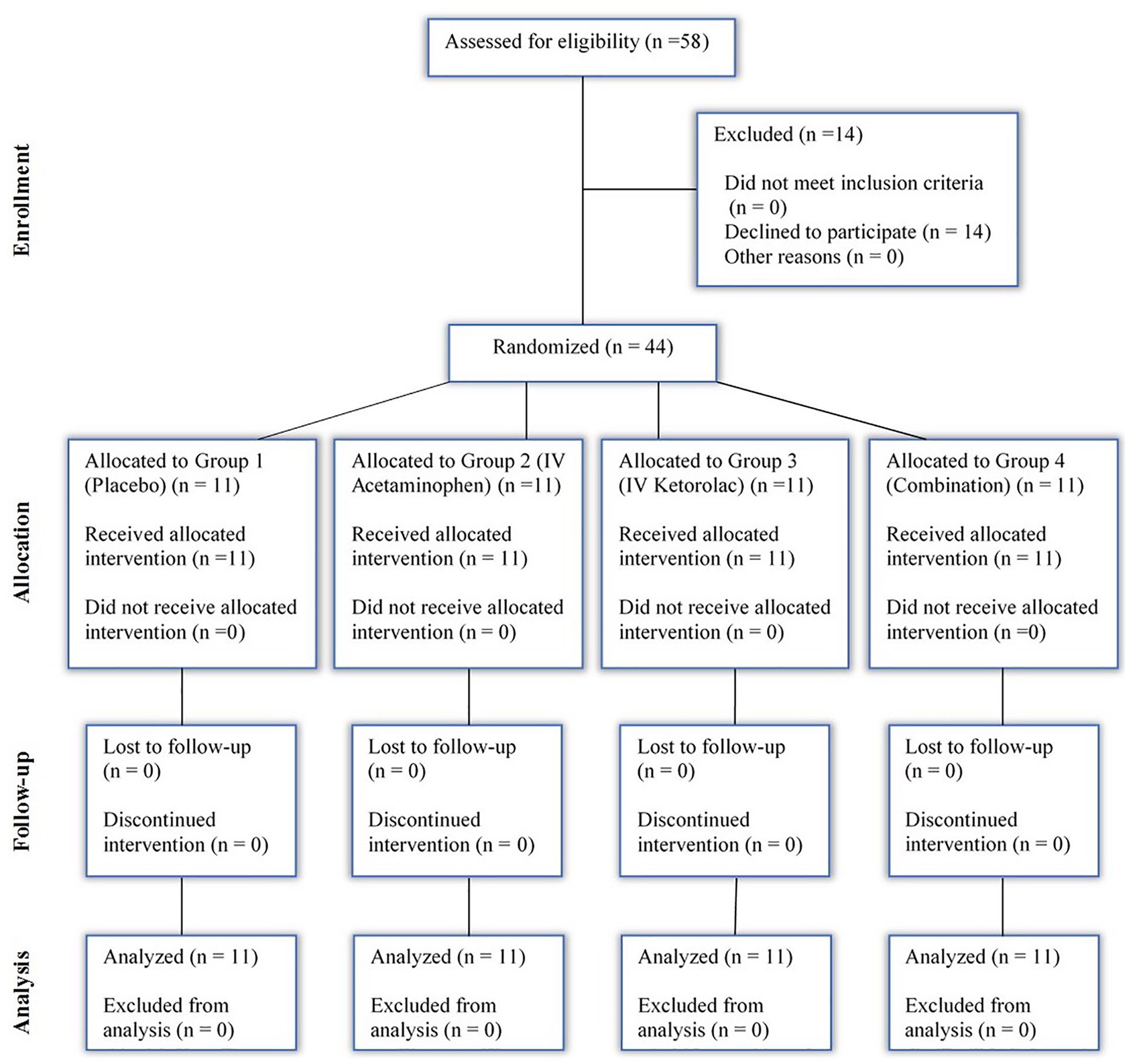
CONSORT diagram showing flow of participants through each stage of randomized trial.
Demographic Comparison of Groups.
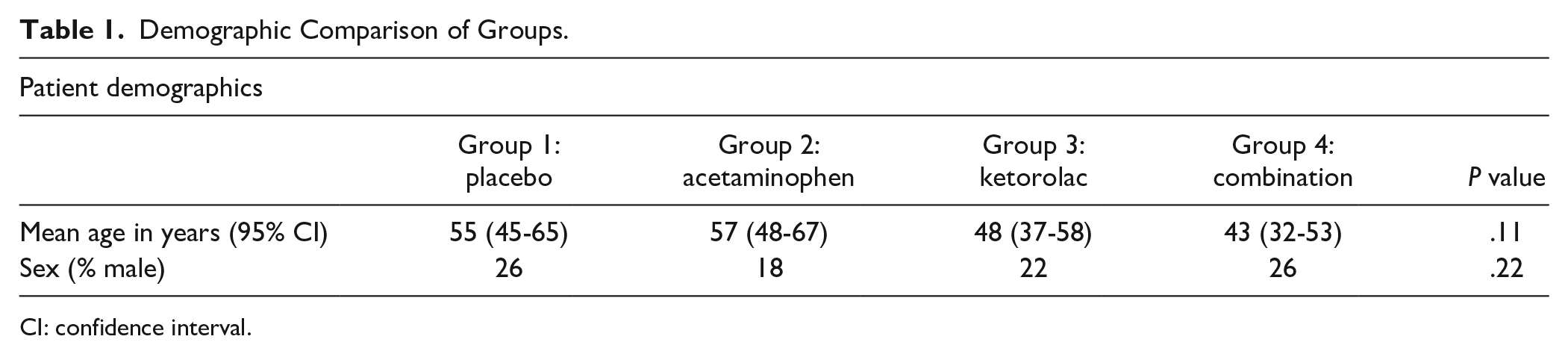
CI: confidence interval.
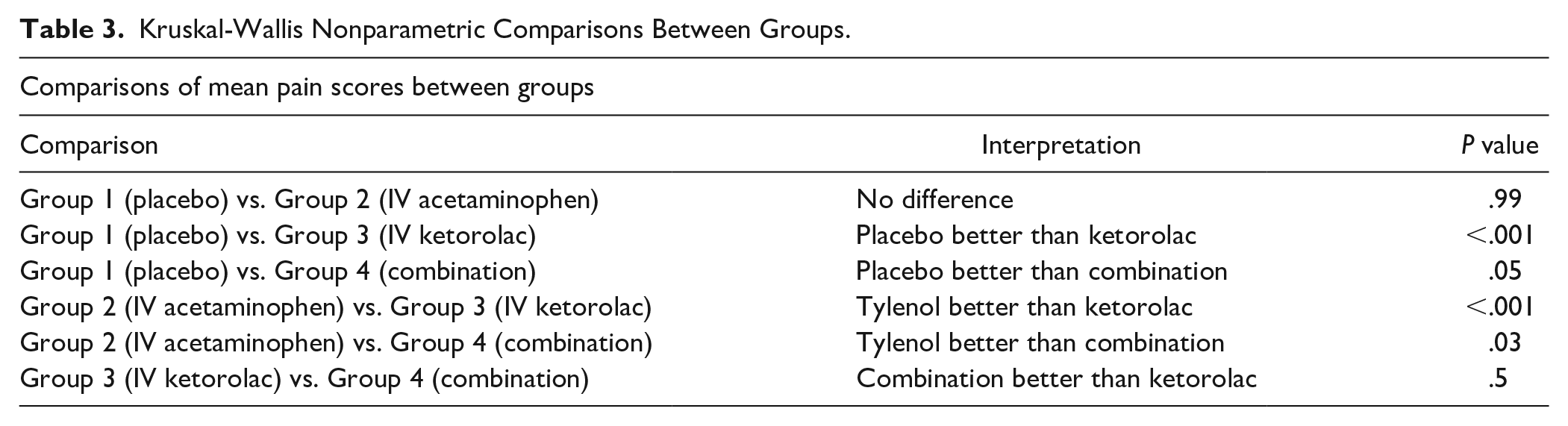
Mean pain was statistically different between groups (Table 2). Mean 11-point pain score over the 7-day study period was 2.0 (95% confidence interval [CI], 1.7-2.3) in the placebo group, 2.0 (95% CI, 1.7-2.3) in the IV acetaminophen group, 2.9 (95% CI, 2.6-3.2) in the IV ketorolac group, and 2.7 (95% CI, 2.3-3.0) in the IV acetaminophen and IV ketorolac combination group (P < .001). Patients in the IV acetaminophen group reported less pain than those in the IV ketorolac group (P < .001) and combination group (P = .03). There was no difference in mean pain scores between the IV acetaminophen and placebo groups (P = .99). Those patients in the placebo group also reported less pain than those in the IV ketorolac (P < .001) and combination groups (P = .05) (Table 3).
Mean and Median Pain Scores.
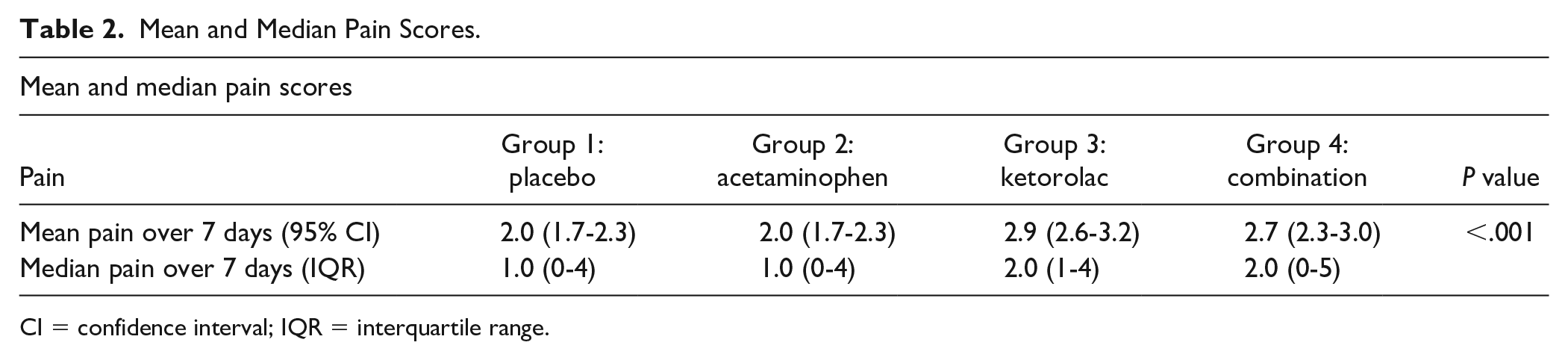
CI = confidence interval; IQR = interquartile range.
Kruskal-Wallis Nonparametric Comparisons Between Groups.
There was no difference in pain the night of surgery (Figure 2). Daily mean pain scores were not different among groups for the first 5 days after surgery. The placebo and acetaminophen groups demonstrated less pain than the ketorolac and combination groups on postoperative days 6 (P = .001) and 7 (P = .02) (Table 4).
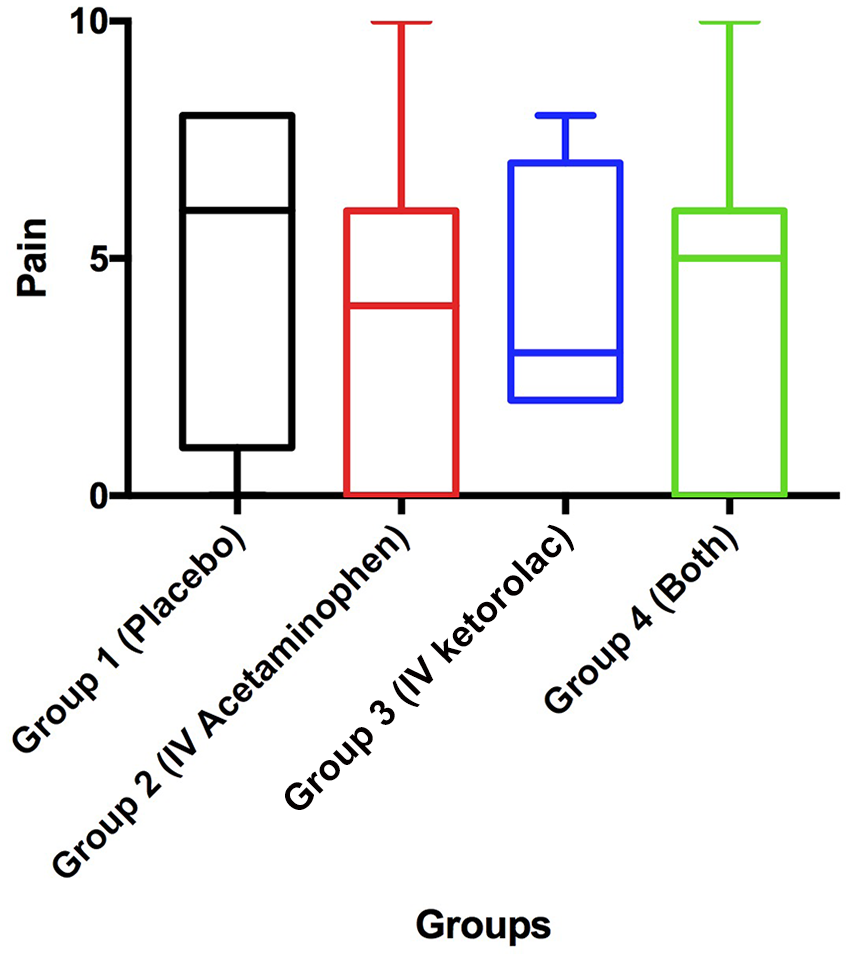
Postoperative day 0 10pm pain score by group.
Daily Mean Pain Scores.
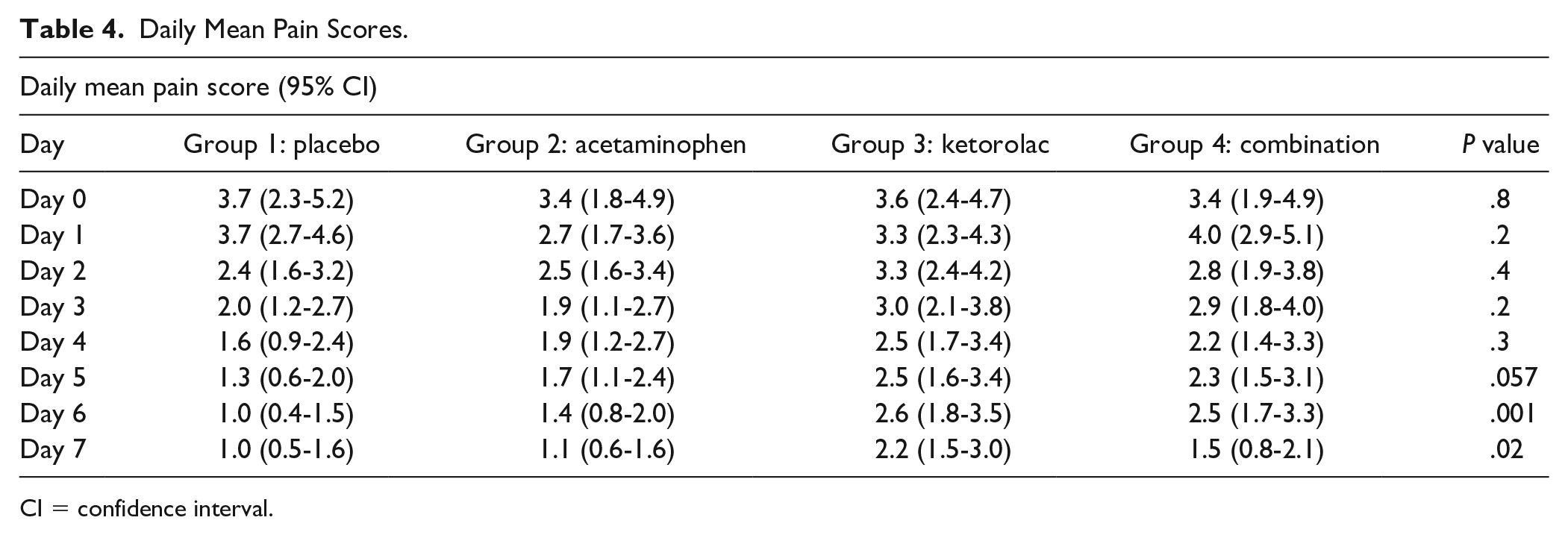
CI = confidence interval.
Of the 44 patients enrolled in the study, 22 (50%) did not take any opioids after surgery. The maximum number of oxycodone tablets consumed was 20, and the mean was 5 tablets over the first 7 postoperative days. Patients who took no opioids reported a mean pain score of 1.4 (95% CI 1.2-1.6), while patients who took opioids had a mean pain score of 3.1 (95% CI 2.9-3.3) over the 7-day course of the study (P < .001). Patients administered IV acetaminophen consumed fewer opioids on postoperative day 0 than those in the combination group (P = .029). They also had lower daily mean opioid usage (0.2 tablets per day) over the first 7 postoperative days when compared to placebo (0.7 tablets per day, P = .02), IV ketorolac (0.7 tablets per day, P = .01), and a combination of IV acetaminophen and IV ketorolac (1.0 tablets per day, P < .001) (Table 5). Patients in the IV acetaminophen group stopped taking opioids sooner with a daily mean of 0 tablets per day on both postoperative days 6 and 7, though this did not reach statistical significance.
Daily Mean Opioid Intake.
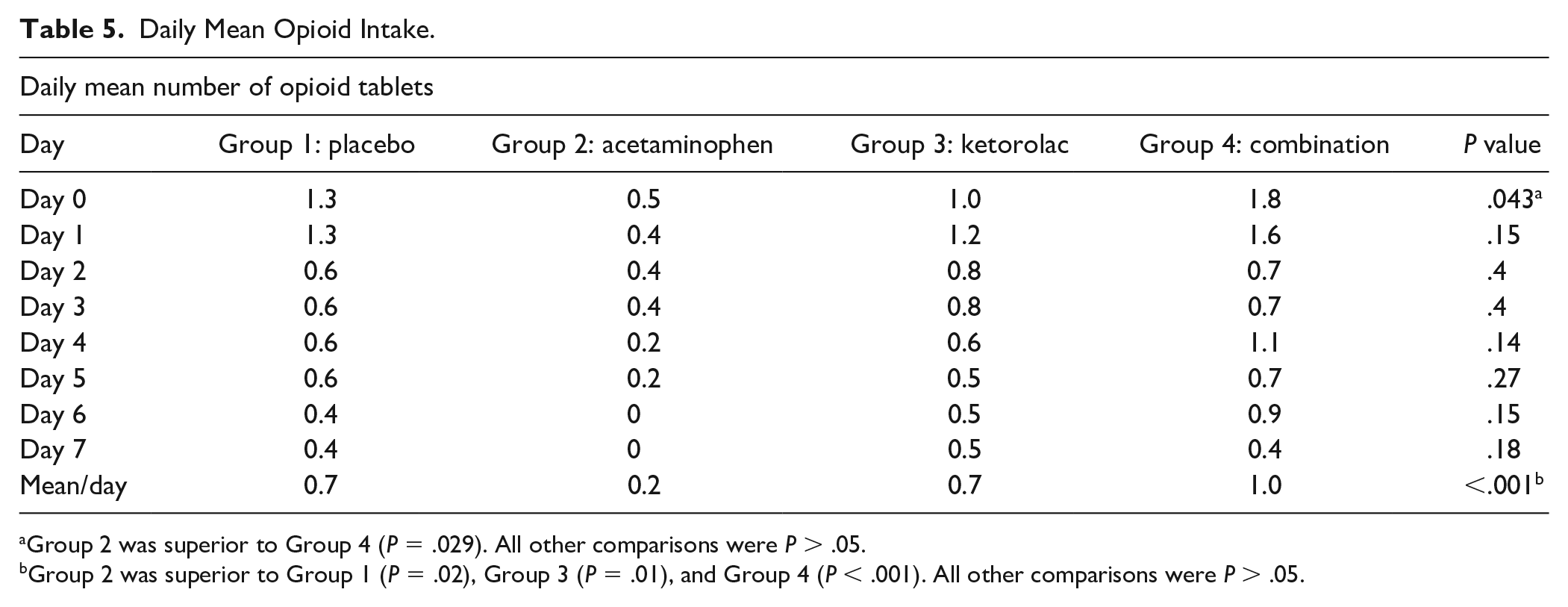
Group 2 was superior to Group 4 (P = .029). All other comparisons were P > .05.
Group 2 was superior to Group 1 (P = .02), Group 3 (P = .01), and Group 4 (P < .001). All other comparisons were P > .05.
Discussion
This study adds to a growing amount of literature supporting a multimodal approach to pain management after upper extremity procedures.5-8 Ketonis et al 5 review anesthesia options and postoperative analgesia that could help minimize narcotic consumption. Others have studied the use of nonsteroidal antiinflammatories (NSAIDs) such as celecoxib or oral ketorolac and its effect on postoperative pain.6,7 A recent study by Ilyas et al examined whether there was a difference in pain levels or medication consumption when using ibuprofen or acetaminophen compared to oxycodone after either endoscopic or open carpal tunnel release performed under local anesthesia without sedation. They point out that the minimal clinically important difference for pain score after carpal tunnel release is unknown, but a score difference of 1.0 has been reported in the anesthesiology literature when considering a broader range of procedures, with a pain score of 3.3 or less considered acceptable by the patient. They recommend using nonopioid medications for pain management and prescribing no more than 5 to 10 pills, regardless of medication choice. 8 In a systematic review of postoperative pain strategies in hand surgery, Kelley et al 9 determined it is beneficial to begin treating pain preoperatively and present an algorithm combining multiple strategies for pain control, including acetaminophen, NSAIDs, opioids, nerve blocks, and neuropathic medications, in a stepwise fashion based on patient and procedure characteristics.
In our study, the local anesthetics used to infiltrate the surgical field likely contributed to the similar pain scores reported on postoperative day 0. Lidocaine 1% without epinephrine has an onset of action from 2 to 5 minutes and a duration of 1 to 2 hours, while bupivacaine 0.5% without epinephrine has an onset of action from 5 to 10 minutes and a duration of 4 to 8 hours. 10 We did not specify the time of day that each surgical procedure was completed thus cannot delineate when the local anesthetic likely wore off, but it may have positively impacted pain control in patients for the majority of postoperative day 0.
IV acetaminophen specifically has been studied in general surgical populations and after major orthopedic procedures. Its onset of action is 5 to 10 minutes with peak analgesic effect at 1 hour postadministration and duration of analgesic effect of 4 to 6 hours. 11 Though there was no difference in mean pain scores between the placebo and IV acetaminophen groups in our study, patients who were administered IV acetaminophen consumed fewer mean opioids per day. All patients in the group stopped taking opioids sooner than those in all other groups with an average of 0 tablets consumed per day on postoperative days 6 and 7, though this did not reach statistical significance. In a recent Cochrane review of single dose IV acetaminophen for postoperative pain, participants receiving IV acetaminophen required 26% less opioid over 4 hours and 16% less over 6 hours than those receiving placebo. 12 Similarly, a multicenter evaluation of IV acetaminophen following hip and knee arthroplasty found significant differences in time to rescue medication and actual consumption in the IV acetaminophen group compared with placebo. 13 In our study, patients who were administered a combination of IV acetaminophen and IV ketorolac consumed more opioids on the day of surgery than those administered only IV acetaminophen. IV ketorolac has a similar but slightly delayed pharmacodynamic profile compared to that of IV acetaminophen, with an onset of action of approximately 30 minutes, peak analgesic effect of 2 to 3 hours, and duration of analgesic effect of 4 to 6 hours. 14 Given the short duration of an endoscopic carpal tunnel release, this slight delay in action and peak could potentially contribute to the difference in number of opioid tablets consumed on postoperative day 0, though it is difficult to reason why the addition of ketorolac to acetaminophen would increase opioid intake outside of it being a random finding.
These differences were small, but they are supportive of using IV acetaminophen for perioperative pain control following endoscopic carpal tunnel release, especially with the current emphasis on responsible prescribing and importance of minimizing opioid use. However, these results may be more clinically relevant if the study was broadened to include more patients or those undergoing more invasive or painful procedures to see if they held true on a larger scale. Additionally, the idea that patients with improved pain control in the immediate postoperative period, which here could be quantified as opioid intake on postoperative day 0, would then have better pain profiles multiple days later, as in lower daily mean pain scores or opioid intake, has not been investigated in upper extremity surgery as far as we were able to find in the literature. Cho et al 15 stated that postoperative pain can be discouraging for patients and asked whether the presence of severe pain immediately postoperative influences pain outcomes, but in their analysis of a group of patients undergoing vertebroplasty, they found that pain scores in the first 4 hours after surgery did not correlate with either short- or long-term pain relief. It is an interesting question whether superior analgesia immediately after surgery could predict how a patient does in the several days following. Otherwise, it is difficult to associate differences in pain or opioid consumption with a specific medication beyond its duration of action.
This study also highlights the tendency for surgeons to overprescribe opioids following upper extremity surgeries,16-22 as half of our patients did not consume any opioids. Patients consumed a mean of 5 tablets over the first 7 postoperative days, yet each patient received a prescription for 20 tablets. These numbers are consistent with other studies in the literature, with mean postoperative opioid consumption numbers cited as 3.0 to 4.3 pills after carpal tunnel release. 18 Gauger et al 19 recently analyzed several articles on opioid use after upper extremity surgeries and found that surgeons tend to prescribe 2 to 5 times more opioids than patients actually consume. In a prospective evaluation of opioid consumption patterns, Kim et al 20 identified specific prescribing guidelines after they determined surgeons prescribed approximately 3 times the number of opioid pills consumed by their patients. They recommend limiting the number of pills prescribed to ≤10 for soft tissue and ≤20 for fracture or joint procedures in the hand and wrist, ≤15 for soft tissue and ≤20 for fracture or joint procedures in the elbow and forearm, and ≤30 for upper arm and shoulder procedures in addition to careful consideration of characteristics such as patient age and anesthesia type. Stepan et al 23 also found that educating prescribers on the opioid epidemic as well as state and federal laws concerning opioid prescribing practices significantly decreased the amount of opioids prescribed following ambulatory hand surgery. Similarly, Ilyas et al 8 discuss how excessive prescribing practices can lead to diversion of medications and that even opioid-naïve patients can develop continued opioid use months after surgery.
Limitations of our study include recall bias, as data were collected through patient surveys regarding pain and opioid consumption. Pain surveys were distributed to patients on the day of surgery, and they were instructed to complete the surveys every 8 hours for 7 days after surgery as well as record the number of oxycodone tablets consumed per day. Nonopioid medications, acetaminophen 1000 mg by mouth every 8 hours and naproxen 500 mg by mouth every 12 hours, were prescribed postoperatively on a scheduled basis, but we do not know if patients took these as prescribed and thus cannot conclude how they may have impacted pain profiles. We did not monitor pain scores specifically within the first 6 hours postoperation, which would most closely report the efficacy of each medication after a single dose. Additionally, recording the time to first rescue medication could help elucidate the mean pain response for the patients in each treatment group and if pharmacokinetics of IV acetaminophen and/or IV ketorolac impacted pain scores or opioid consumption on postoperative day 0.
We did not follow any negative reactions to the medications administered, but this could shift the risk-benefit profile. Pain on infusion is one of the most commonly cited adverse events with IV acetaminophen. However, a 2016 Cochrane review found similarly low rates of pain on infusion with IV acetaminophen versus placebo, with 3% of participants receiving IV acetaminophen and 1% of participants receiving placebo reporting pain. They found that adverse events, such as malaise, hypotension, or increased hepatic enzymes are rare, ranging from 1/1,000 to 1/10,000. Additionally, subgroup analysis demonstrated that IV acetaminophen actually reduced rates of nausea and vomiting compared to placebo. 12
This study could easily be expanded to include more patients undergoing endoscopic carpal tunnel release by the senior author and thereby increase the power of our results. Compared to other orthopedic procedures, endoscopic carpal tunnel release likely does not induce severe pain, so the methodology could also be applied to more invasive upper extremity surgeries after which patients tend to experience increased pain levels in order to determine whether the conclusions we reached remain valid. The results of this study emphasize the utility of IV acetaminophen in postoperative pain control and the importance of limiting opioid prescribing following endoscopic carpal tunnel release.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The senior author has received a grant from the American Foundation for Surgery of the Hand (AFSH) and a grant from the National Institutes of Health (Grant Number UL1-TR-000005).