
Abstract
Introduction
Thumb carpometacarpal (CMC) joint arthritis affects up to 15% of adults over the age of 30 1 and approximately 10% of all middle-aged women. 2 A trial of conservative treatment, including activity modification, hand therapy, splinting, and steroid injections, is commonly encouraged before pursuing operative intervention.3-5 However, there is no established treatment algorithm for thumb CMC arthritis, and the extent to which different conservative measures are used is driven by the physician–patient relationship. Therefore, preoperative healthcare utilization for thumb CMC arthritis is quite variable and influenced by provider and patient choice. Given the national focus on patient-centered care, many studies of healthcare utilization fail to evaluate value from the patient’s perspective, especially in conditions such as thumb CMC arthritis, for which treatment is driven by subjective processes.
As insurance reimbursement changes, patients are beginning to bear the burden of healthcare costs through rising deductibles, co-insurance, and co-payments. Recent media coverage has brought to light this phenomenon with growing concerns over patients paying more for their healthcare including the prices of pharmaceuticals. 6 Some speculate that these out-of-pocket (OOP) expenses may lead to inequities in access to care 7 and delays in treatment.8,9 With healthcare costs in the United States continuing to grow, some insurers have turned to capitation, offering 1 physician reimbursement for each enrolled patient regardless of the amount of services rendered, in contrast to the fee-for-service (FFS) model. Capitated insurance plans provide patients with a designated group of providers and facilities, which may limit the choice in physicians. 10 However, these plans may improve access to care and patient satisfaction. 11 Within these different insurance models, little is known regarding the financial burden placed on patients for treatment of conditions in which nonoperative treatment varies and treatment decisions can be subjective.
Given the variable treatment course for thumb CMC arthritis, the influence of insurance type and capitation on preoperative resource utilization, cost, and OOP expenses warrants closer investigation. Understanding the presurgical cost sharing stratified by insurance type for patients with multiple treatment options, such as those with thumb CMC arthritis, will inform policymakers regarding the financial burden placed on patients. Therefore, the purpose of this study is to examine the effects of capitation on OOP expenses for the surgical and presurgical care for patients receiving surgery for thumb CMC arthritis. Furthermore, we aim to characterize preoperative resource utilization and total costs stratified by insurance type.
Materials/Methods
Data Source
Patients were selected from the Truven MarketScan Research Databases, including the Commercial Claims and Encounters Database and the Medicare Supplemental and Coordination of Benefits database, from 2009 to 2016. These databases include insurance claims from employee-sponsored health plans and Medicare Advantage or Medicare supplemental insurance plans, which capture inpatient and outpatient healthcare encounters, prescription drug usage, and patient-level costs for over 245 million unique patients. 12 Patient data are encrypted and de-identified, allowing for longitudinal tracking of patients. Because of the de-identified nature of the database records, this study qualified for exempt status from the institutional review board.
Cohort Selection
The study cohort comprised patients aged 18 years or older, with a diagnosis of hand osteoarthritis who underwent trapeziectomy, trapeziectomy with ligament reconstruction and tendon interposition, CMC joint arthrodesis, or CMC joint prosthetic replacement between January 1, 2011 and December 31, 2016. We identified patients using Current Procedural Terminology (CPT) codes and International Classification of Disease, Ninth Revision and Tenth Revision, Clinical Modification diagnosis codes (ICD-9/ICD-10) (Supplemental Appendix A). To capture preoperative resource utilization, we ensured that all patients were continuously enrolled in the database for at least 2 years prior to the surgical intervention. We excluded patients who changed their type of insurance plan during the study period. Patients with a diagnosis of wrist osteoarthritis, carpal fracture, fracture nonunion, avascular necrosis, and rheumatoid arthritis in the 2 years prior to undergoing surgery were excluded from our cohort. Figure 1 illustrates the inclusion and exclusion criteria for the study.
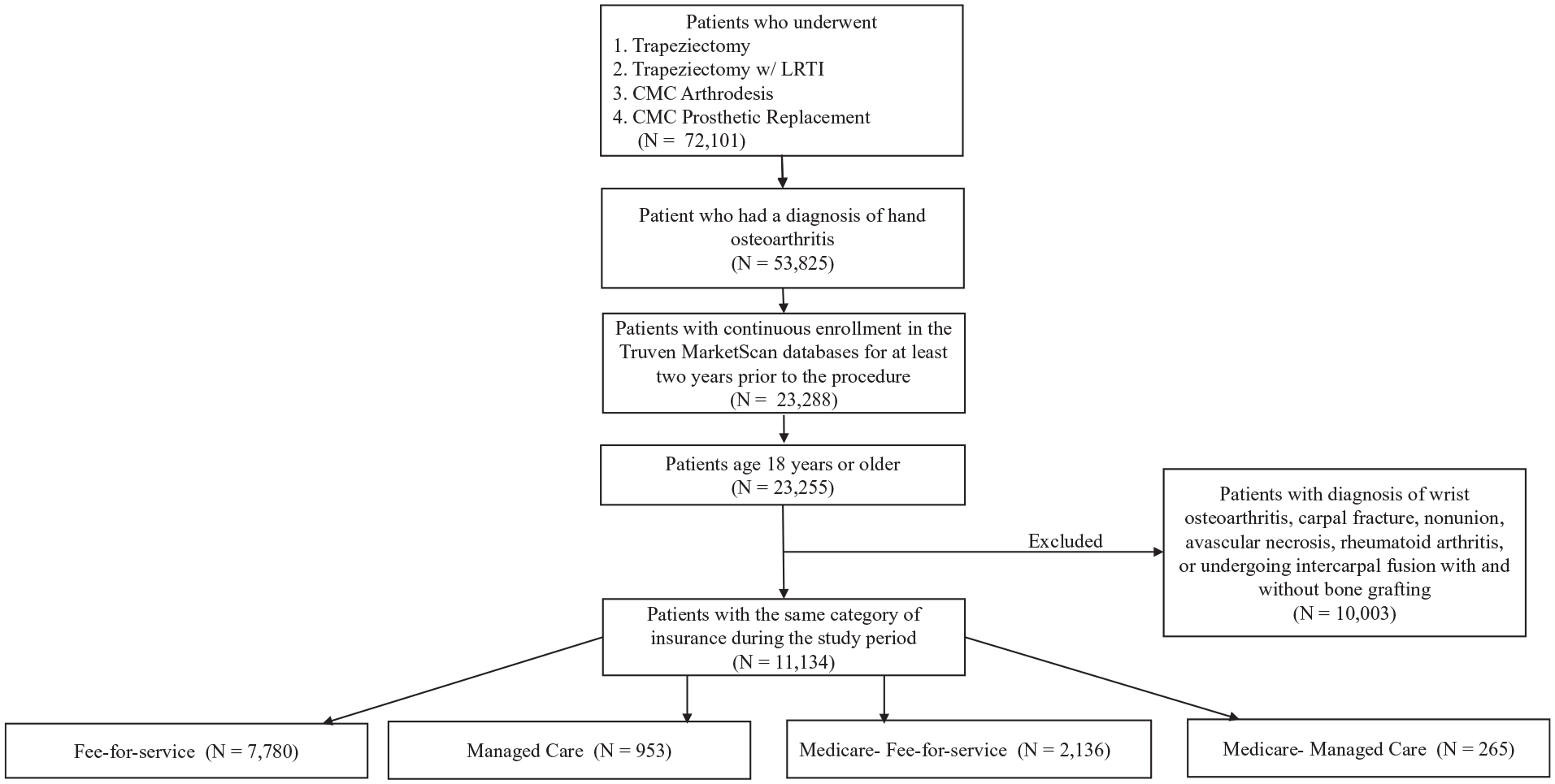
Inclusion and exclusion criteria for cohort selection.
Dependent Variables
The outcome of interest included cumulative OOP spending for surgery and nonoperative treatments during the 2 years before surgery for CMC arthritis. OOP spending comprised the cost of care that the patient incurred including co-payments, deductibles, and co-insurance payments. This definition was chosen because these OOP expenses change with healthcare utilization. We also collected cumulative cost data and resource utilization information during the 2-year presurgical episode and surgical encounter. We inflation adjusted all costs to 2016 dollars. Resource utilization data comprised of the number of clinic visits, number of emergency department visits, number of radiographic studies, number of nonoperative treatment modalities (ie, occupational therapy visits), and number of corticosteroid injections using ICD-9/ICD-10 diagnosis and procedure codes and CPT codes (Supplemental Appendix B). Relevant encounters were associated with a diagnosis of hand arthritis to ensure accurate assessment of preoperative utilization.
Explanatory Variables
We collected patient-specific data including sociodemographic characteristics and comorbidities. Variables of interest included sex, age, median household income in the area of residence, insurance type, and geographic region. Insurance type was separated into 4 groups: FFS, managed care (MC), Medicare-fee-for-service (Medicare-FFS), and Medicare-managed care (Medicare-MC). MC consisted of health maintenance organizations and preferred provider organizations that were either partially or fully capitated. FFS comprised basic or major medical plans, comprehensive plans, exclusive provider organizations, point-of-service, preferred provider organizations without capitation, and consumer-driven health plans. We calculated the Elixhauser comorbidity score for each patient as a surrogate for health status using ICD-9 and ICD-10 codes.13,14 Additionally, smoking status, obesity, and diabetes mellitus diagnoses were gathered for each patient.
Analyses
Given the likely clinical differences between Medicare and non-Medicare patients, we compared FFS to MC and Medicare-FFS to Medicare-MC. We examined the association between insurance type and the outcomes of preoperative resource utilization, total cost, and OOP spending prior to surgery for thumb CMC arthritis using the chi-square test and Fisher exact test for categorical variables and the Wilcoxon rank sum test for continuous variables.
We then created a log-transformed generalized linear model to predict the proportional change in OOP expenses based on independent patient characteristics. The primary outcome in the model was cumulative OOP expenses for the surgical and presurgical care 2 years prior to undergoing surgery for thumb CMC arthritis, controlling for patient characteristics. In the model, covariates included insurance type, sex, age, median household income, and geographic region. The regression coefficients represent cost ratios, which are the multiplicative change in the outcome (OOP expenses) compared to the reference group (eg, a regression coefficient of 1.10 would represent a 10% increase in the predicted outcome compared to the reference group). Significance level was set at P < .05 for all analyses. Analyses were performed using SAS 9.4 (Copyright © SAS Institute Inc., Cary, North Carolina).
Results
A total of 11 134 patients received surgery for thumb CMC arthritis between 2011 and 2016 and met the inclusion criteria for our study. Of these patients, 7780 (70%) had FFS insurance, 953 (9%) had MC insurance, 2136 (19%) had Medicare-FFS insurance, and 265 (2%) had Medicare-MC insurance. The mean preoperative time from diagnosis of thumb CMC arthritis to surgery was 11 months (standard deviation: 8), and the median time was 10 months (interquartile range: 3-19). Table 1 describes the patient demographic and clinical characteristics stratified by insurance type. When comparing FFS to MC and Medicare-FFS to Medicare-MC, gender, age, and Elixhauser comorbidity score were statistically similar among the groups. Geographic variation was significantly different between FFS and MC (P < .001) and between Medicare-FFS and Medicare-MC (P < .001).
Sociodemographic Characteristics of Patients Undergoing Surgery for CMC Arthritis, N = 11 134.
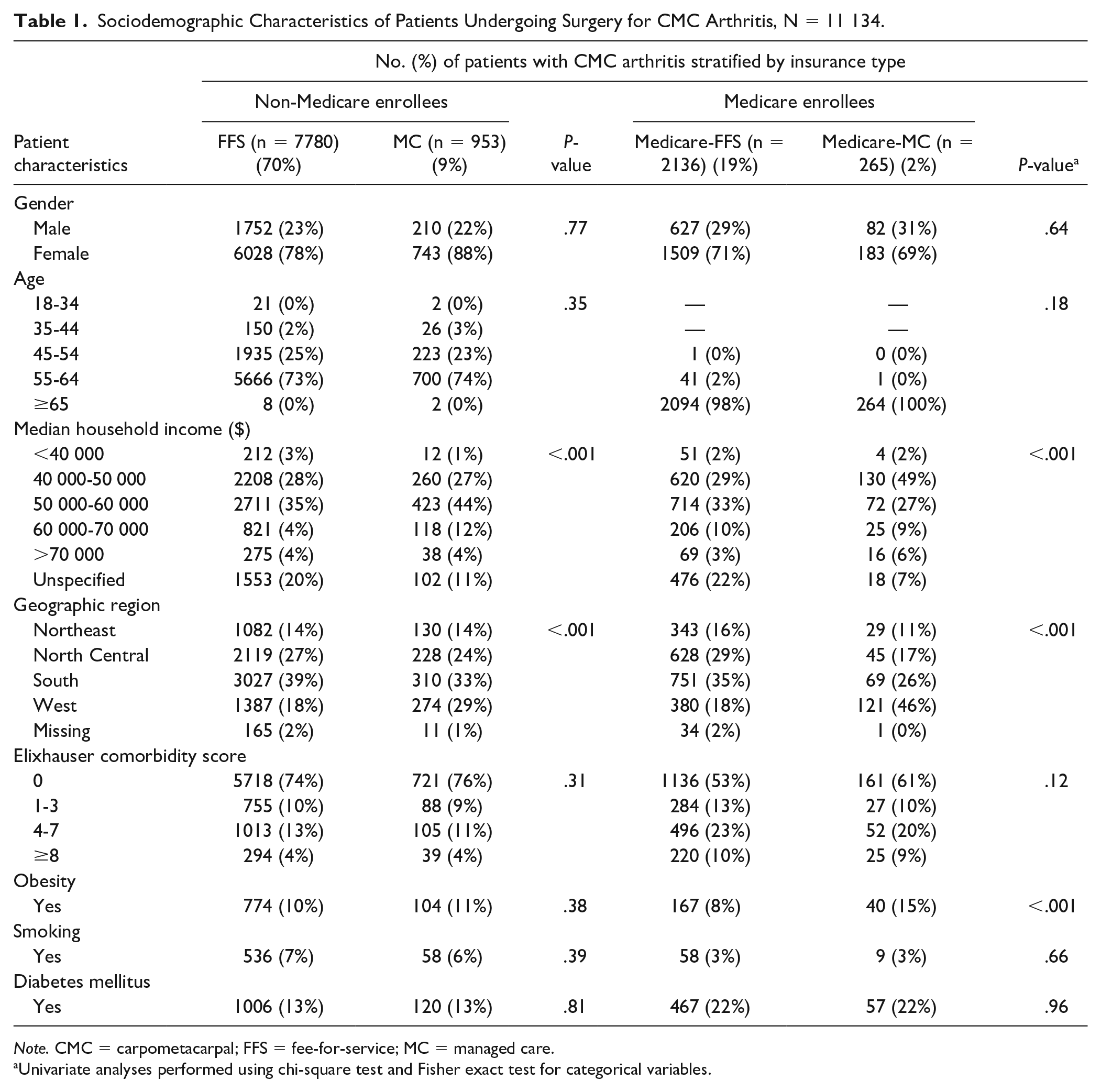
Note. CMC = carpometacarpal; FFS = fee-for-service; MC = managed care.
Univariate analyses performed using chi-square test and Fisher exact test for categorical variables.
Preoperative resource utilization for the 2 years prior to surgery for thumb CMC arthritis stratified by insurance type is presented in Table 2. On average, FFS patients had more cumulative encounters compared to MC patients (5.6 vs. 5.3, P = .02). However, there were no differences when comparing Medicare-FFS to Medicare-MC (5.5 vs. 5.4, P = .76). Furthermore, there were no differences in total imaging, number of clinic visits, or number of emergency department visits between the groups. However, patients with Medicare-FFS underwent more therapy encounters than patients with Medicare-MC (3.5 vs. 2.3, P = .03).
Two-Year Preoperative Resource Utilization for CMC Arthritis.
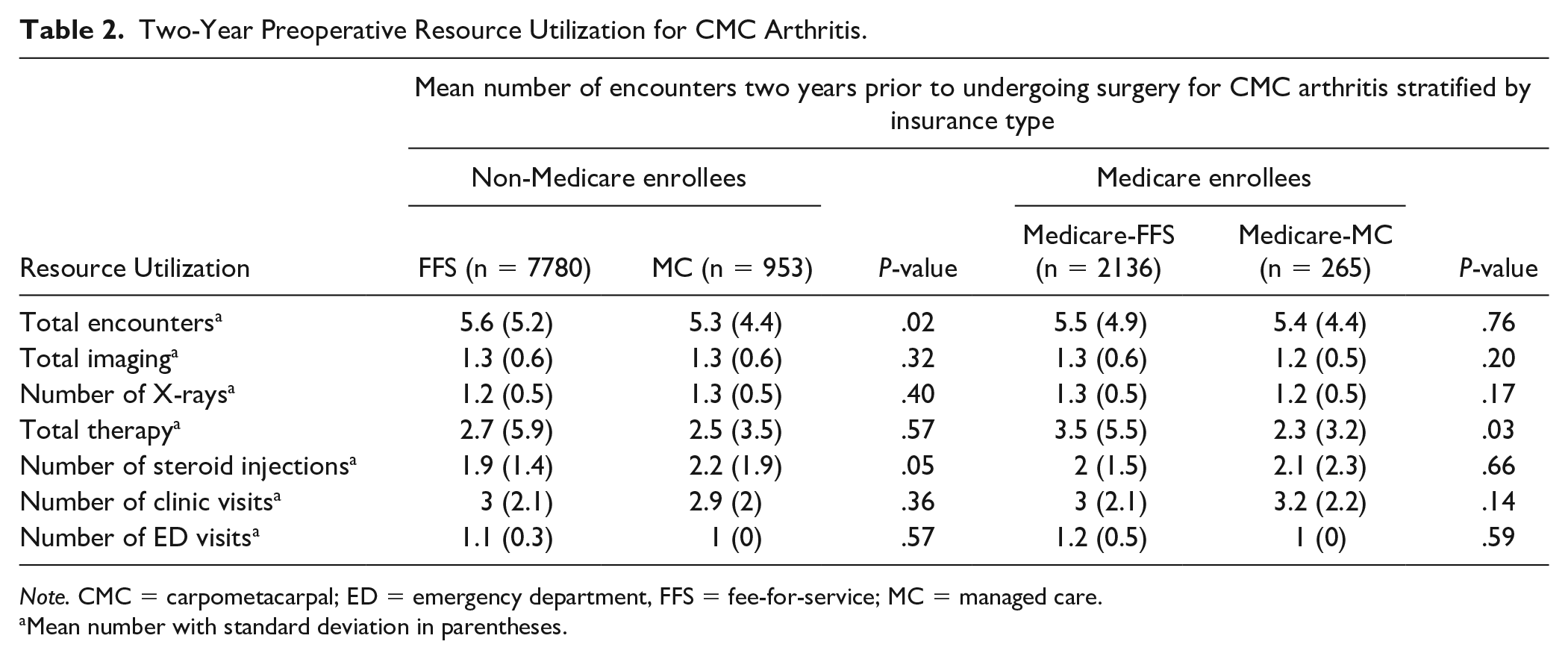
Note. CMC = carpometacarpal; ED = emergency department, FFS = fee-for-service; MC = managed care.
Mean number with standard deviation in parentheses.
Table 3 outlines the cost and OOP expenses for the 2 years prior to undergoing surgery for thumb CMC arthritis including both presurgical care and the surgery encounter. The total cost of the surgical encounter paid to the insurer was similar between the groups. Additionally, the cumulative cost for the surgical plus the presurgical encounters was not significantly different between the groups (Table 3). Figure 2 illustrates the cumulative presurgical costs excluding the surgical encounter from 3 to 24 months prior to surgery for thumb CMC arthritis stratified by insurance type. The average cumulative OOP expenses for the 2-year presurgical period plus surgical encounter for patients with FFS was $952 compared to $434 for patients with MC (P < .001). Similarly, Medicare-FFS incurred $343 in cumulative OOP expenses for the 2-year presurgical period plus surgical encounter, and Medicare-MC incurred $232 of cumulative OOP expenses for the same period (P = .003). Figure 3 demonstrates the cumulative presurgical OOP expenses excluding surgery from 3 to 24 months prior to surgery for thumb CMC arthritis stratified by insurance type. There was no significant difference in cost of surgery paid to the insurer for patients with FFS versus MC insurance ($6795 vs. $6831, P = .70) and for patients with Medicare-FFS versus Medicare-MC insurance ($6242 vs. $5695, P = .23). However, OOP expenses for the surgical encounter were significantly different between the groups (Table 3).
Mean Cost of Two-Year Preoperative Resource Utilization for CMC Arthritis.
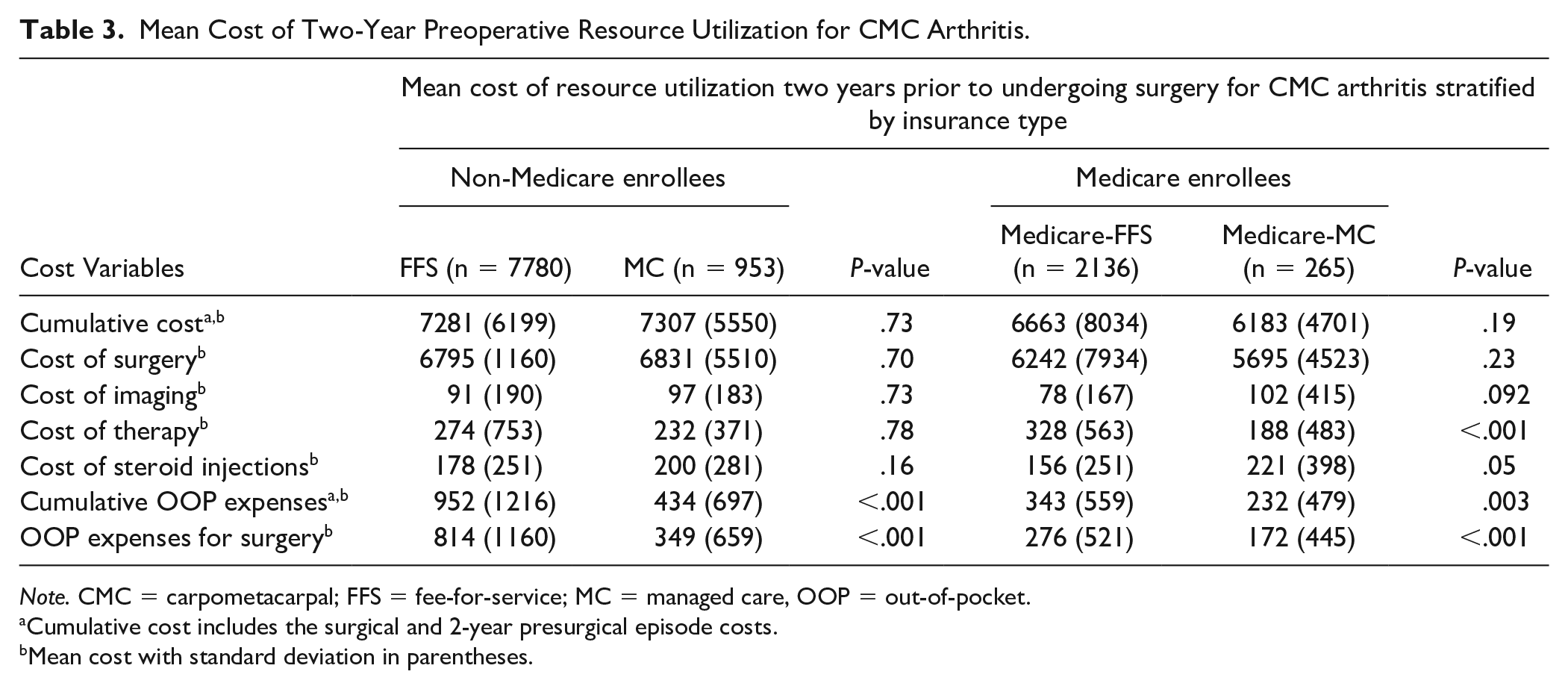
Note. CMC = carpometacarpal; FFS = fee-for-service; MC = managed care, OOP = out-of-pocket.
Cumulative cost includes the surgical and 2-year presurgical episode costs.
Mean cost with standard deviation in parentheses.
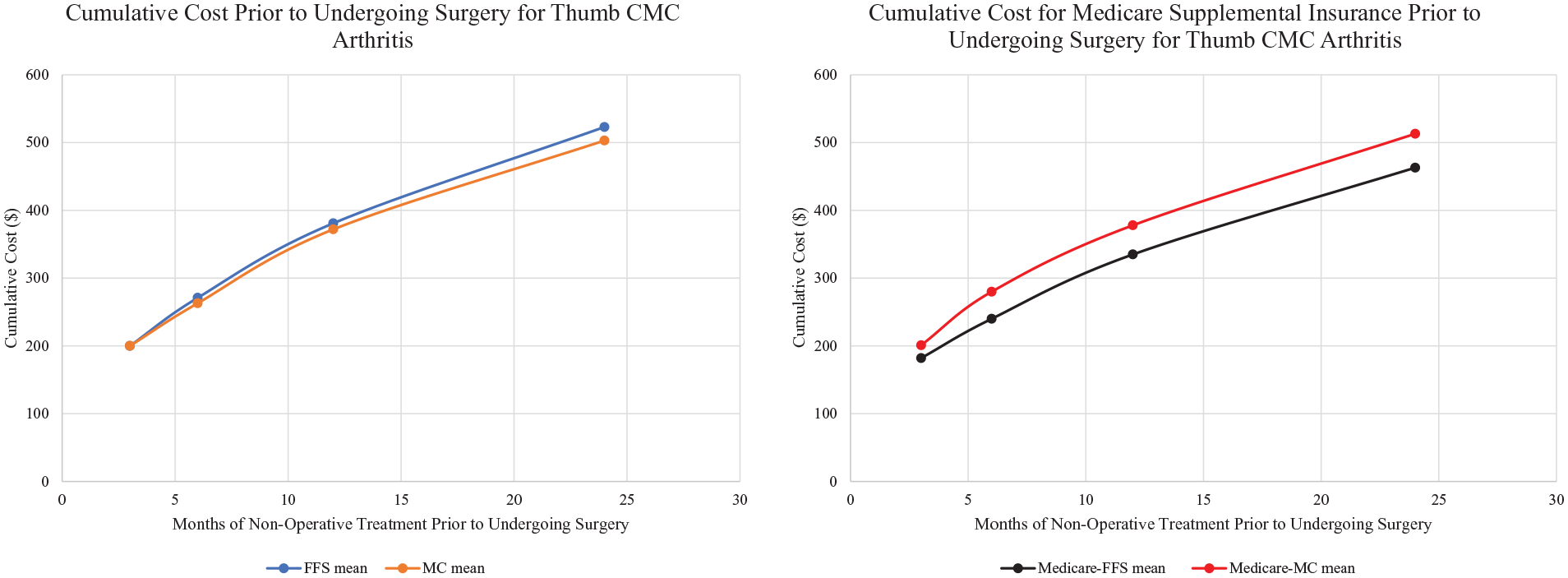
Cumulative mean cost of presurgical episode excluding surgical encounter stratified by insurance type; cumulative cost includes clinical encounters, imaging, and therapy for the entire preoperative time prior to surgery.
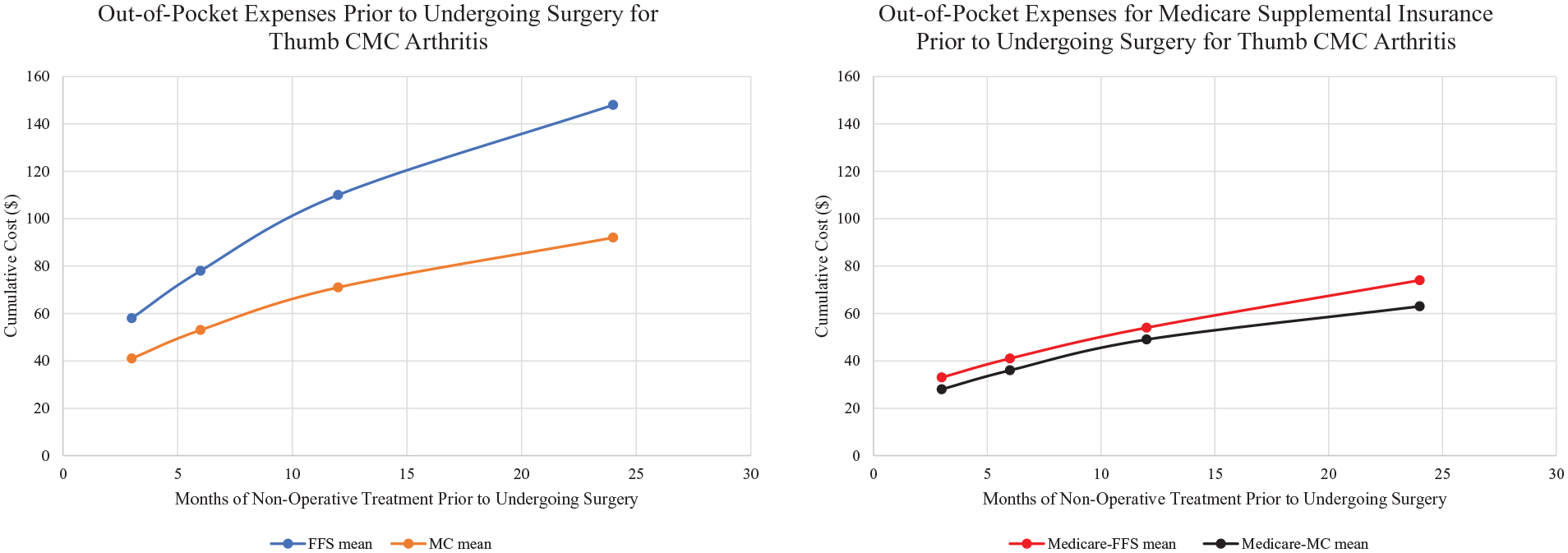
Cumulative mean out-of-pocket expenses of presurgical episode excluding surgical encounter by insurance type; cumulative out-of-pocket expenses includes clinical encounters, imaging, and therapy for the entire preoperative time prior to surgery.
Using generalized log-transformed linear regression, OOP expenses for MC patients were 46% of OOP expenses of FFS patients (cost ratio: 0.46, 95% CI, 0.43-0.50, P < .001) for care received during the 2-year presurgical period and surgery encounter. Medicare-MC patients had 21% of the predicted OOP expenses of FFS patients (cost ratio: 0.21, 95% CI, 0.14-0.31, P < .001). Table 4 depicts the results of the generalized log-transformed linear regression of predicted OOP expenses adjusted for sex, age, insurance type, median household income, and geographic region. Patients in the North Central, South, and West regions of the United States had approximately 35% to 56% more OOP expenses as compared to patients in the Northeast (P < .001).
Generalized Linear Regression of Out-of-Pocket Expenses and Patient Characteristics.
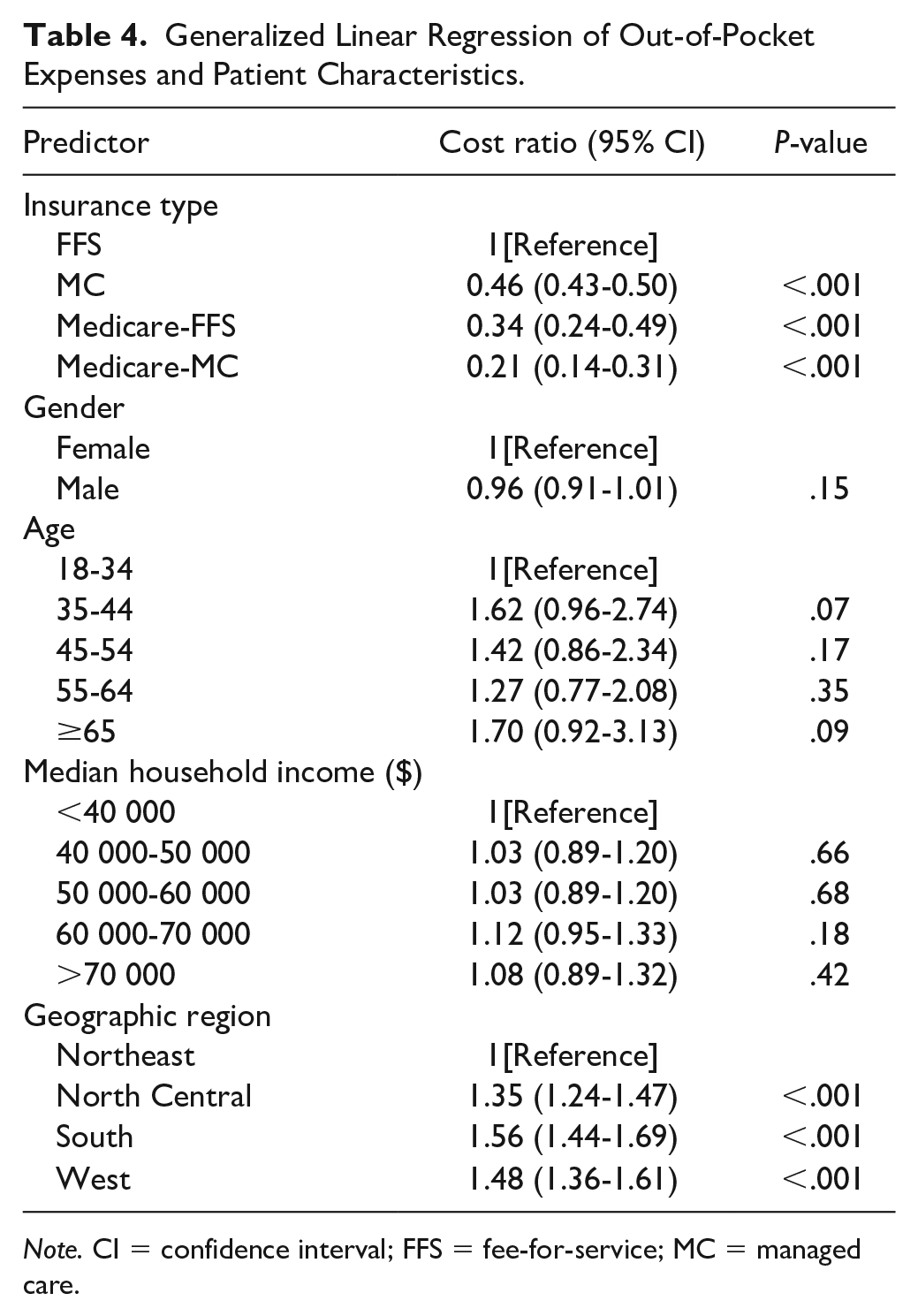
Note. CI = confidence interval; FFS = fee-for-service; MC = managed care.
Discussion
In this national analysis, patients with FFS insurance and Medicare-FFS insurance incurred significantly higher OOP expenses for their surgical and presurgical care for thumb CMC arthritis. However, we found no differences in cumulative costs and surgical costs paid to the insurer. Collectively, these findings reveal the influence of insurance type on the direct financial burden to the patient. Given the current emphasis on high-value healthcare, reforms aimed at cost reduction should incorporate evaluations of OOP expenses in addition to total cost to also consider the financial strain placed on patients and value from the patient’s perspective.
With policymakers continuing to disagree about healthcare reform, there is an ongoing debate of who will ultimately assume the burden of healthcare expenditures: patients, providers, or insurers. One approach, capitation, transfers the financial liability to providers, and has been used as a payment reform to curb healthcare expenditures. Through providing physicians with a fixed sum of money per patient, capitation aims to transfer the economic risk to providers and to minimize between provider variation, intending to promote more efficient healthcare at lower costs. Studies have illustrated that capitation leads to lower hospitalization rates15-17 and reduction in healthcare costs with equivalent patient outcomes.18,19 On the other hand, advocates against capitation warn that it leads to underutilization of appropriate care by physicians to save money.20,21 Studies have shown that patients with capitated insurance plans are less likely to receive nonessential surgery 22 such as carpal tunnel release 23 and cataract surgery, 24 highlighting the influence of reimbursement structure on care utilization. In our study of preoperative resource utilization before undergoing surgery for thumb CMC arthritis, we found patients with FFS insurance had a slightly higher number of encounters as compared to MC patients (5.6 vs. 5.3 encounters). Though this difference was statistically significant, it is unlikely to be clinically significant as we found no differences in total imaging, total therapy, number of clinic visits, or number of emergency department visits between the 2 groups. When comparing the Medicare-FFS and Medicare-MC groups, we found no differences in total number of encounters. Therefore, for the presurgical episode of care for thumb CMC arthritis, capitation does not appear to influence patients’ or providers’ use of conservative treatments in patients who ultimately received surgery, likely reflecting the influence of the physician–patient relationship in the decision-making process. However, this study focuses on a surgical cohort; therefore, the impact of insurance type on receipt of surgery cannot be investigated. Future studies of direct patient and provider encounters are needed to determine if insurance type and increasing OOP expenses affect decision-making in pursuing conservative measures or surgery for thumb CMC arthritis.
As insurers seek to reduce healthcare spending and overuse, there have been changes in health insurance policies with a transition of some costs to beneficiaries. With these changes, OOP expenses continue to increase. Our study emphasizes the importance of cost sharing when determining treatment for patients with thumb CMC arthritis. We found no difference in cumulative cost of care for the 2-year presurgical episode and for the cost of surgery stratified by insurance type. However, patients with FFS and Medicare-FFS had significantly higher OOP expenses, suggesting a trade-off between insurance coverage and cost sharing. Furthermore, patients with Medicare-MC and MC had approximately 21% to 46% of the OOP expenses of patients with FFS. MC insurance plans may place limits on patients’ selection in providers, but this limited choice may protect patients against direct financial costs through decreased cost sharing. The national increase in cost sharing has been spurred by approximately an 86% rise in deductibles and a 33% rise in co-insurance, which varies substantially across different medical and surgical diagnoses. 25 However, physicians infrequently consider patients’ OOP expenses when conferring care, yet patients prefer communicating about costs with physicians before deciding treatment.26-28 In a study of physician surveys, Pham et al found that only 40% of physicians consider OOP expenses when ordering diagnostic tests and only 51% consider OOP expenses when determining inpatient versus outpatient treatment. As compared to primary care physicians, medical subspecialists were less likely to consider cost sharing when ordering tests or prescribing treatment, highlighting the lack of emphasis placed on value from the patient’s perspective. 29 In conditions with less concrete treatment algorithms, such as thumb CMC arthritis, where patients can undergo numerous conservative measures, providers should consider OOP expenses to limit the financial burden placed directly on their patients.
With increases in cost sharing, direct patient costs have implications for access to care. OOP expenses have been shown to augment the socioeconomic disparities in healthcare. Overall, studies have shown that patients in low-income areas have less adherence to medication than patients in high-income areas. However, this finding was compounded when patients had increased co-payments with patients from low-income areas and high cost sharing having the least medication adherence. 30 The authors postulate that increased cost sharing is intensifying socioeconomic health disparities. Additionally, other studies have demonstrated that increased cost sharing in the pediatric population can lead to delays in care. In a study by Fung et al, 7 patients at or below 250% of the federal poverty line delayed taking their child to a clinic visit for an asthma exacerbation if they had higher cost sharing. Given the variation in OOP expenses based on insurance type, there is potential for patients to delay or forgo treatment and exacerbate current healthcare disparities. Therefore, providers should have candid discussions with patients about treatment decisions and OOP expenses, especially in conditions such as thumb CMC arthritis with multiple treatment options.
As with other insurance claims studies, our analyses have several limitations. The Truven MarketScan databases do not contain granular clinical information such as disease severity. However, we limited our cohort to patients who ultimately underwent surgical intervention for CMC arthritis to control for differences in disease severity. Furthermore, it is unknown whether insurance type and magnitude of OOP expenses influences receipt of surgery for thumb CMC arthritis. Additionally, insurance claims data do not contain physician-patient interactions and decision-making regarding treatment options, which may play a role in utilization of specific treatments. We also cannot verify if the preoperative treatments were provider- or patient-driven. Moreover, this study lacks data on premiums paid, which may have added financial burden for patients, but are not directly impacted by healthcare utilization. Lastly, we derived our cohort from a large employer-based insured population including Medicare supplemental insurance, thus limiting the generalizability of our findings to the Medicaid, Medicare-only, and uninsured populations. Patients with employer-sponsored health insurance may have less severe disease and disability than patients with other types of insurance, which may affect resource utilization in the preoperative period.
Despite these limitations, our population-based study reveals the influence of insurance type on direct patient OOP expenses for both the presurgical and surgical care for patients with thumb CMC arthritis. Patients with capitated insurance plans had significantly less cost sharing with similar cumulative costs paid to the insurer. With healthcare expenditure transitioning to patients through rising deductibles, co-payments, and co-insurance, providers should consider OOP expenses when conferring care. Furthermore, healthcare reform aimed at promoting high-value care should also consider reduction in OOP expenses to limit the financial burden placed on patients and consider value from the patient’s perspective.
Supplemental Material
Appendix_A_final – Supplemental material for Out-of-Pocket Spending for Thumb Carpometacarpal Arthritis: Capitation Matters
Supplemental material, Appendix_A_final for Out-of-Pocket Spending for Thumb Carpometacarpal Arthritis: Capitation Matters by Jessica I. Billig, Yu-Ting Lu, Brian P. Kelley, Kevin C. Chung and Erika D. Sears in HAND
Supplemental Material
Appendix_B_final – Supplemental material for Out-of-Pocket Spending for Thumb Carpometacarpal Arthritis: Capitation Matters
Supplemental material, Appendix_B_final for Out-of-Pocket Spending for Thumb Carpometacarpal Arthritis: Capitation Matters by Jessica I. Billig, Yu-Ting Lu, Brian P. Kelley, Kevin C. Chung and Erika D. Sears in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study qualified for exempt status from the institutional review board.
Statement of Informed Consent
Because of the exempt status, the need for informed consent was waived.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.C.C. receives book royalties from Wolters Kluwer and Elsevier. He has received financial support from Axogen to attend conferences. J.I.B., Y.T.L., B.P.K., and E.D.S. have nothing to disclose. E.D.S. is supported by a Career Development Award Number IK2 HX002592 from the United States (U.S.) Department of Veterans Affairs Health Services R&D (HSRD) Service.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Erika D. Sears is supported by a Career Development Award Number IK2 HX002592 from the United States (U.S.) Department of Veterans Affairs Health Services R&D (HSRD) Service. The funding organizations had no role in the design and conduct of the study, including collection, management, analysis, and interpretation of the data.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.