
Abstract
Keywords
Introduction
While multiple surgical techniques for the treatment of basal joint osteoarthritis have been described, there is no clear consensus on which provides superior outcomes. In an effort to better delineate any advantage between the techniques performed at this institution, a retrospective review comparing clinical outcomes and patient satisfaction with trapeziectomy and abductor pollicis longus (APL) suspensionplasty compared to trapeziectomy with ligament reconstruction and tendon interposition (LRTI) was performed. The authors’ hypothesis is that soft tissue only reconstruction (APL suspensionplasty without bone tunnels) following trapeziectomy would result in quicker recovery and greater patient satisfaction than LRTI. As subsidence does not correlate with clinical outcome, the authors seek to determine if the added potential morbidity and risk of creating bone tunnels and harvesting the flexor carpi radialis (FCR) adds any additional stability in the short term.
Methods
Study Design
A retrospective review of 139 consecutive patients treated surgically for basilar arthritis with either APL suspensionplasty or LRTI from 2008 to 2015 at the Hand Center of San Antonio was performed. Of the 139 patients, 51 patients (53 hands) were treated with trapeziectomy with APL suspensionplasty and were compared to 151 patients (166 hands) who underwent treatment with trapeziectomy with LRTI. Outcomes assessed included postoperative pain relief, grip and pinch strength, major complications (tendon adherence and impingement), minor complications (wound infection and dehiscence), and need for revision surgery. Relief or persistence of preoperative pain was determined by clinical documentation because visual analog scale pain scores were not consistently document pre- and postoperatively. Two-tailed, Fisher exact test was used for data analysis.
Surgical Technique—Trapeziectomy
For both techniques, a trapeziectomy is first performed via a dorsal approach. The first dorsal compartment is released along the dorsal margin of the subsheath to prevent volar tendon subluxation. Dorsal periosteal flaps are elevated to expose the trapezium which is removed in either a piecemeal fashion with a Rongeur or as a whole with a corkscrew joystick, depending on surgeon preference.
Surgical Technique—APL Suspensionplasty
The APL suspensionplasty is performed in a similar fashion to that described by Sigfusson and Lundborg. 1 A distally based slip of the APL tendon is created. This slip is then brought through the distal FCR tendon where it is tensioned appropriately and sutured to itself. The remaining APL is folded on itself, secured and placed in the trapeziectomy void.
Surgical Technique—LRTI
Following trapeziectomy in patients undergoing LRTI, a bone tunnel is drilled through the base of the first metacarpal. The FCR tendon is transected proximally, delivered into the trapeziectomy defect, and split. Half of the FCR tendon is then passed through the drill hole in the first metacarpal. The 2 halves of the FCR tendon are then tied to each other to suspend the first metacarpal based and sutured together. The rest of the tendon halves are tied together to create an anchovy which is placed in the trapeziectomy void.
Results
APL suspensionplasty resulted in postoperative pain relief in 92.5% (n = 49) of cases compared to 94.0% (n = 156) seen with LRTI (P = .758). Mean postoperative grip and pinch strengths with APL suspensionplasty were 41.2 and 10.4 kg, respectively. With LRTI, average grip strength was 42.1 kg, and pinch strength was 9.7 kg. Both techniques were well-tolerated with few complications. In the APL suspensionplasty group, 2 patients who underwent simultaneous thumb metacarpophalangeal joint fusion experienced adherence of the extensor pollicis longus (EPL) tendon, one of whom required tenolysis. One patient had a postoperative infection requiring drainage. Among the LRTI cases, 1 patient experienced wound dehiscence requiring re-closure, and 2 patients had minor postoperative infections treated with oral antibiotics. Mean follow-up time among APL suspensionplasty patients was 3.3 months compared to 8.4 months following LRTI (Table 1).
Technique Comparison.
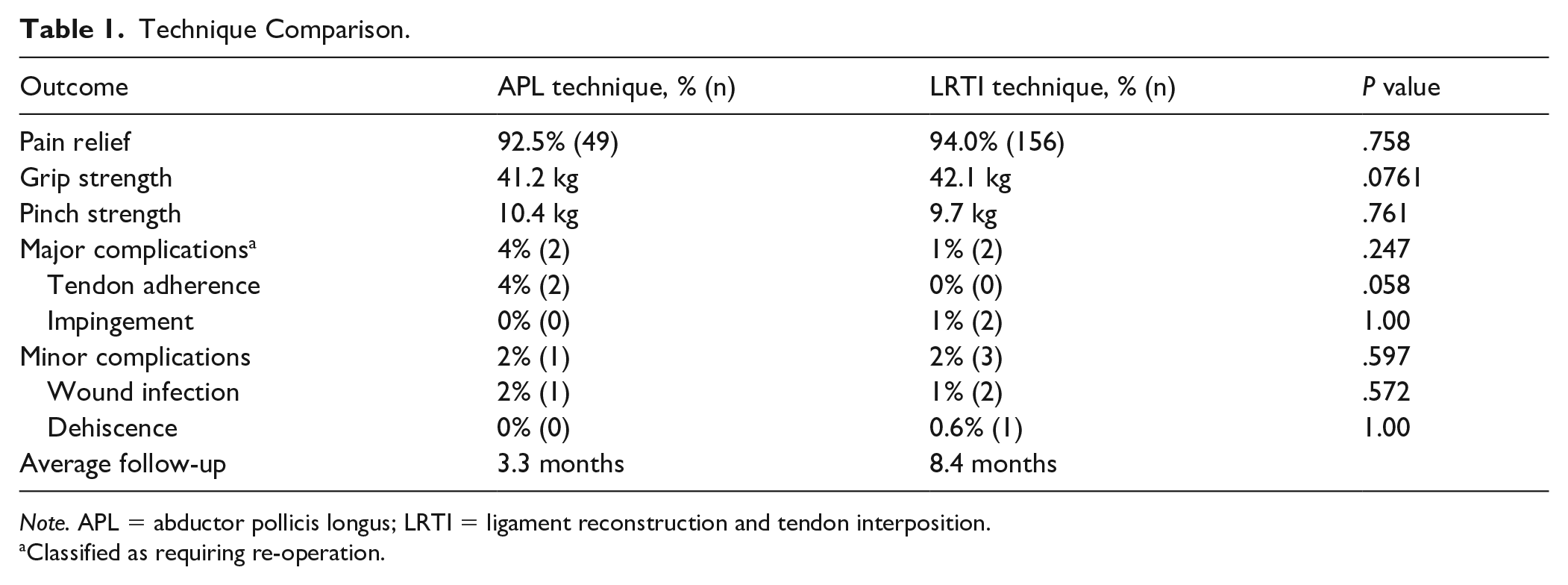
Note. APL = abductor pollicis longus; LRTI = ligament reconstruction and tendon interposition.
Classified as requiring re-operation.
Discussion
The use of the APL tendon for stabilization and suspension of the first metacarpal following trapeziectomy was first reported by Thompson in 1986 as a salvage technique following failed trapezium implant arthroplasty. In this initial description, the dorsal APL slip was divided at the musculotendinous junction, passed through bone tunnels in the first and second metacarpal bases, and interwoven with the extensor carpi radialis brevis (ECRB) tendon. Immobilization with a Kirschner wire was performed for 5 to 6 weeks. 2
Since 1986, numerous variations of Thompson’s technique have been published in the literature. Some of these techniques incorporate the use of bone tunnels,2-7 Kirschner wire fixation,2,5,6 an interweave with ECRB,2,7 extensor carpi radialis longus,6,8,9 FCR,1,10- 12 or a wrap-around FCR.4,10,13 Reported complications are uncommon but include superficial radial nerve entrapment, neuritis or neuroma, reflex sympathetic dystrophy, tendon rupture, and superficial surgical site infection.4,6,9,13,14
A review of the literature identified 14 previous studies reporting the use of trapeziectomy with APL suspensionplasty for the treatment of carpometacarpal (CMC) arthritis in a total of 444 hands (Table 2).1-9,11,13,14,15 Outcomes evaluated in these studies included pain relief, range of motion, pinch and grip strength, patient satisfaction, and results of validated questionnaires such as the Disabilities of the Arm, Shoulder and Hand score and Michigan Hand Outcomes Questionnaire score. As seen in this study which reports pain relief in 92.5% of the patients undergoing APL suspensionplasty, high rates of pain improvement was seen elsewhere in the literature. Studies documenting pain-related outcomes reported “excellent,” “very good,” or “good” relief in 76.2% to 100% of patients.3,4,5,13 Complete resolution of pain was reported in 38.1% to 70%.1,2,7,14
Literature Review of APL Suspensionplasty Techniques.
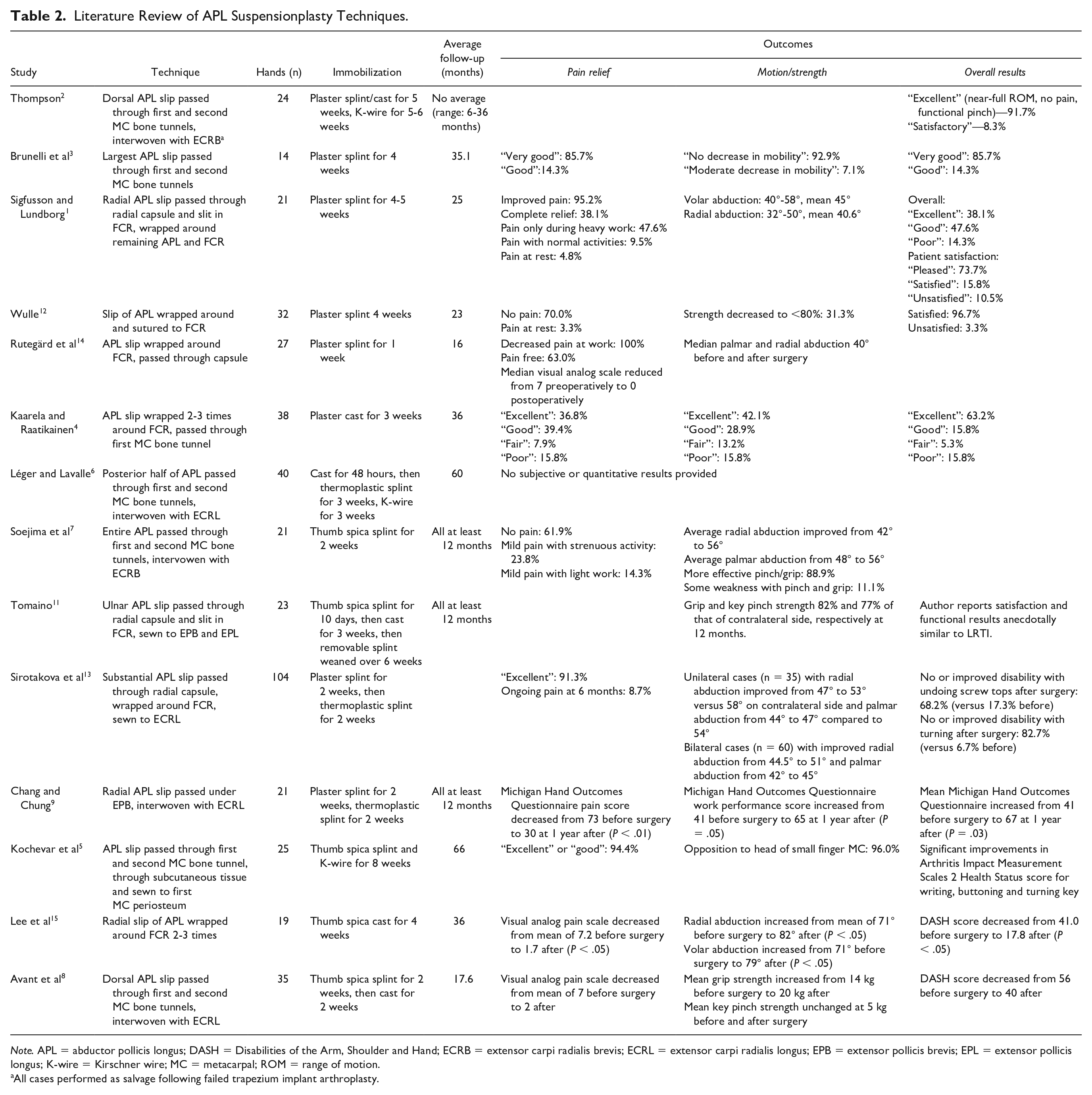
Note. APL = abductor pollicis longus; DASH = Disabilities of the Arm, Shoulder and Hand; ECRB = extensor carpi radialis brevis; ECRL = extensor carpi radialis longus; EPB = extensor pollicis brevis; EPL = extensor pollicis longus; K-wire = Kirschner wire; MC = metacarpal; ROM = range of motion.
All cases performed as salvage following failed trapezium implant arthroplasty.
The technique used here is most similar to that initially described by Sigfussen and Lundborg in 1991. A single incision is used to perform trapeziectomy and harvest of the radial-most slip of the APL tendon. The tendon slip is passed through the joint capsule and FCR tendon, and secured to the FCR with appropriate tension to suspend and stabilize the first metacarpal. By eliminating the use of metacarpal bone tunnels, Kirschner wire fixation, and a second incision for tendon harvest described in other APL suspensionplasty techniques, this method may avoid some of the pain and morbidity associated with other approaches. This is difficult to quantify, however. Chang and Chung 9 also advocate use of the radial-most APL slip as it is favorable because traction of this slip ulnarly toward the FCR tendon will adduct the thumb metacarpal base and correct its lateral subluxation.
Additionally, limited immobilization was used in this study with 6 weeks of splinting compared to up to 8 weeks reported in previous publications. Our high rate of pain relief and low rate of complications support that earlier mobility and return to normal activities is likely safe. Further studies evaluating whether this might correlate to earlier return to work and baseline function would be beneficial.
While this study and others support the safe and efficacious use of APL suspensionplasty as a treatment for advanced CMC arthritis, there is very little data comparing it to other well-established surgical options such as trapeziectomy alone and LRTI. In our review, only 1 German language study comparing APL suspensionplasty (n = 21) to LRTI (n = 20) was identified. This comparison reported statistically significantly shorter operative time, shorter scars, stronger pinch, key grip, and grip strengths with APL suspensionplasty. No significant differences in pain, range of motion, Disabilities of the Arm, Shoulder and Hand Score, or radiographic subsidence were seen however. 16 While this study did not demonstrate the same statistically significant advantages of APL suspensionplasty over LRTI, it does support its use as a safe and effective alternative.
Compared to other techniques described for APL suspensionplasty in the literature, the technique used here eliminates the need for a second incision utilized by Chang, Kochevar, and Lèger. Others have reported an incidence of FCR tendonitis with use of the APL up to 25%. 16 No cases of tendonitis were seen in our 53 suspensionplasties with this technique.
In addition to APL suspensionplasty and LRTI, a variety of other techniques for the surgical management of basal joint arthritis have been demonstrated to effectively relieve pain—all centered around removal of the trapezium.17-29 This includes trapeziectomy alone,17-19 hematoma distraction arthroplasty (trapeziectomy with temporary K-wire fixation),20,21 suture suspensionplasty between the APL and FCR tendons,22,23 suture button suspensionplasty between the first and second metacarpals,24,25 and allograft and xenograft interpositions.26,27 The use of multiple types of implant arthroplasties has also been reported; however, long-term complication rates have limited their popularity thus far.28,29
While trapeziectomy alone has been shown to be effective in relieving pain, the various suspensionplasty and interposition techniques seek to prevent subsidence of the first metacarpal into the void of the removed trapezium which theoretically could be associated with a loss of thumb height/mechanical advantage or arthrosis of the new metacarpal-scaphoid interface. This subsidence, however, has not been reproducibly demonstrated to have negative clinical implications. While some previous studies have suggested that subsidence may be associated with decreased pinch strength,30,31 more recent studies suggest that the degree of radiographic subsidence does not correlate with clinical function.32,33 Some subsidence is still seen even with techniques utilizing an autogenous tendon interposition, including LRTI and APL suspensionplasty, as the final bulk of the interposition “anchovy” is inadequate to replace the height of the trapezium. This has not been shown to impact clinical or functional outcomes.7,33
Although most of the literature reports outcomes of a single surgical technique, there are multiple comparison studies, including a few randomized trials, which have shown equivalent rates of pain relief, patient-reported outcome measures, and/or functional outcomes with trapeziectomy alone, with or without temporary K-wire fixation, and LRTI.17-19,21
While no one technique has been reproducibly demonstrated as a superior method for surgically improving pain and dysfunction associated with basal joint arthritis, we posit that the APL suspensionplasty offers shorter postoperative immobilization, potentially shorter operative times, and the avoidance of additional incisions, bone tunnels, and K-wires which may provide advantages over other techniques such as LRTI.
Conclusion
Although this study does not demonstrate clear superiority of the APL suspensionplasty in terms of speed of recovery and greater patient satisfaction compared to LRTI as initially hypothesized by the authors, it does provide additional evidence that APL suspensionplasty is a safe, effective procedure which provides similar pain relief and functional outcomes compared to LRTI. This technique potentially minimizes postoperative pain by avoiding morbidity associated with an additional incision for tendon harvest, bone tunneling, and percutaneous skeletal fixation in the immediate postoperative period. Mean follow-up in the APL group was shorter compared to LRTI; this may be because patients in the APL group returned to function sooner. Long-term follow-up studies are ongoing to determine if pain relief and overall satisfaction are maintained.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was not performed for this study as the patient present is not identifiable and no risk or harm was incurred by the patient as a result of the study.
Statement of Informed Consent
Informed consent was not performed for this study as the patient present is not identifiable and no risk or harm was incurred by the patient as a result of the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author D.P. is a shareholder for S.E.G.-WayTM Orthopedics, which is not related to this study. All other authors have no conflicts of interest to report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.