
Abstract
Introduction
To date, most epidemiologic studies have focused on ballistic firearm injuries, and data on nonballistic firearms (ie, those that do not use gunpowder) remain largely unknown. Nonballistic firearms such as BB and pellet guns are frequently purchased in the United States, with more than 3.2 million of these being sold annually. 1 They vary in design, from standard handguns to bolt action rifles, and some tactical models that mimic military sniper rifles are available. Although widely considered to be toy guns, they are often used as a nonballistic option for harvesting small game during hunting seasons in the United States. As such, they can cause serious morbidity and mortality, as evidenced by the 39 nonballistic firearm–associated deaths between 1990 and 2000. 2 The fact that nonballistic firearm muzzle velocities can surpass that of a 0.22-caliber handgun and approach those of low-powered traditional powder-based firearms is a concern to public safety due to their widespread use.1,3 Currently, there are only 24 states that carry any restriction on the sale of nonballistic firearms. 4
In this cross-sectional study, the epidemiology of pediatric upper extremity injuries secondary to nonballistic firearm (BB or pellet guns) trauma was explored using the US Consumer Product Safety Commission’s (CPSC) National Electronic Injury Surveillance System (NEISS). This study aimed to describe anatomical injury patterns to the upper extremity and commonly associated diagnoses in this population with further delineation of how these injuries were stratified by demographic factors such as age, sex, and race.
Materials and Methods
The NEISS database serves as a nationally representative, statistically validated probability sample of American hospital emergency departments—stratified by both hospital size and geographic location—from which reliable national estimates for injuries associated with a consumer product or activity may be derived. Data collection methodologies, as well as general information with respect to the survey coding and organization, can be found publicly on the CPSC webpage.5-7
In this study, each yearly sample in the NEISS database was first queried between 2000 and 2017 for all injuries of the upper extremity (defined in this study as those involving the finger, hand, wrist, lower arm, elbow, upper arm, or shoulder) associated with nonballistic firearms (Product Codes: 1237; 1936) in patients ≤18 years of age. Nonballistic firearms included gas, air, or spring-operated guns, but excluded those using gunpowder or other ballistics ammunition, toy guns, tools (ie, nail guns, glue guns, etc), or personal protective devices (bean bag guns, tear gas guns, etc). Then, case narratives were individually analyzed to exclude any injuries not explicitly associated with BB or pellet guns, such as injuries associated with paintball guns or potato guns. Following exclusion criteria from the narrative sections, 1502 unique cases of pediatric upper extremity injuries associated with BB or pellet gun use were identified in the NEISS database, yielding a total weighted estimate of 52 118 national cases presenting to US emergency departments during this time.
All weighted national estimates, standard errors, and 95% confidence intervals were calculated using parameters that are intrinsically provided by the NEISS database. The NEISS parameters “PSU,” “Weight,” and “Stratum” are inputs that the sysvet function in Stata/IC 15.1 statistical software (StataCorp, College Station, Texas) uses to give usable outputs such as primary sampling unit (PSU), data entry weight, and hospital stratum. These output data allow for the derivation of national weighted estimates for the given queries, which can be summed across years for annualized results. Significance of trends in the total national survey estimates was determined using adjusted Wald tests. Values of P < .05 (2-sided) were considered significant.
Results
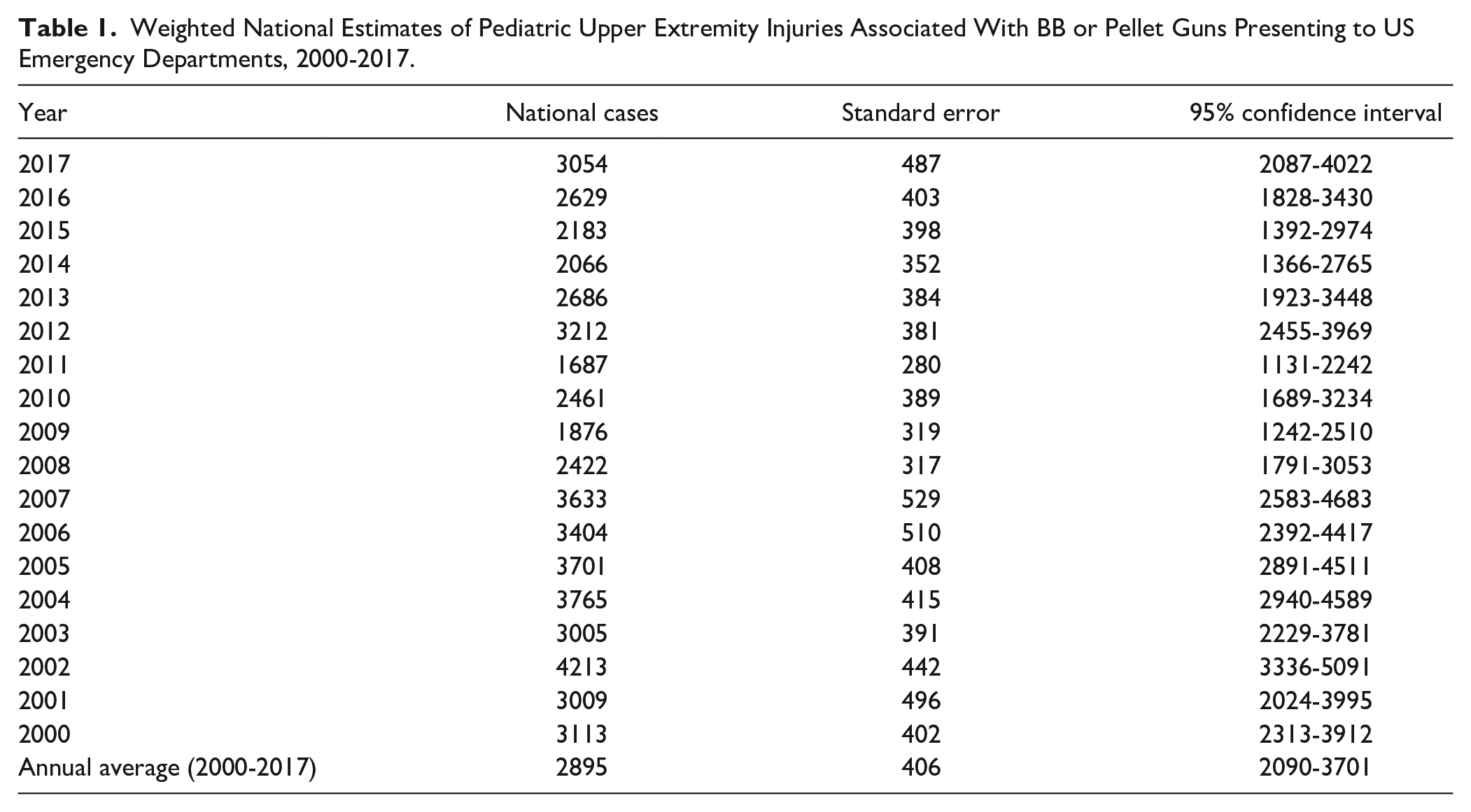
Yearly case totals from 2000 to 2017 are presented in Table 1. Over the study period, there were an estimated 2895 cases of pediatric nonballistic firearm trauma to the upper extremity annually in the United States.
Weighted National Estimates of Pediatric Upper Extremity Injuries Associated With BB or Pellet Guns Presenting to US Emergency Departments, 2000-2017.
Nonballistic weapon type and anatomical injury patterns are summarized in Table 2. BB guns comprised 79.4% of injuries, whereas pellet guns comprised 20.6%. The most commonly injured body part was the hand (41.1%), followed by fingers (35.9%). The most commonly associated diagnosis with these injuries was retained foreign body (58.0%), followed by puncture wound (20.2%). A single nerve injury was documented and was included and reported in the “other” group in Table 2. No vascular injuries were documented as part of the study.
Overall Diagnosis Characteristics of Pediatric Patients Presenting to US Emergency Departments With Injuries Associated With BB or Pellet Guns, 2000-2017.
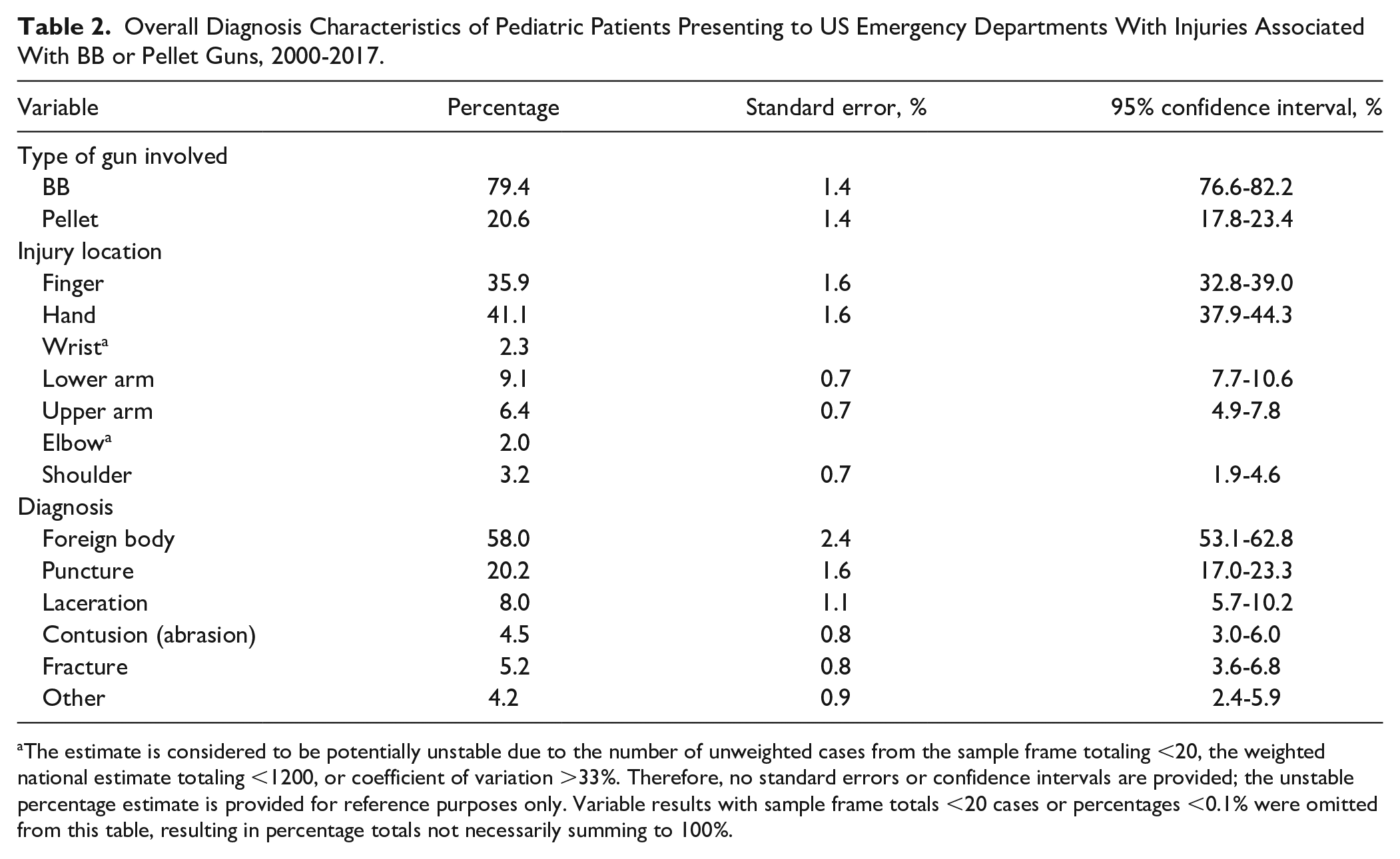
The estimate is considered to be potentially unstable due to the number of unweighted cases from the sample frame totaling <20, the weighted national estimate totaling <1200, or coefficient of variation >33%. Therefore, no standard errors or confidence intervals are provided; the unstable percentage estimate is provided for reference purposes only. Variable results with sample frame totals <20 cases or percentages <0.1% were omitted from this table, resulting in percentage totals not necessarily summing to 100%.
Demographic characteristics of the patient population involved in this study are included in Table 3. The vast majority of these injuries occurred at home and were sustained by men (91%), and adolescents between the age of 12 and 18 years were the most commonly injured (69.8%). Only 3.5% of these injuries led to inpatient admission.
Overall Demographics of Pediatric Patients Presenting to US Emergency Departments With Injuries Associated with BB or Pellet Guns, 2000-2017.
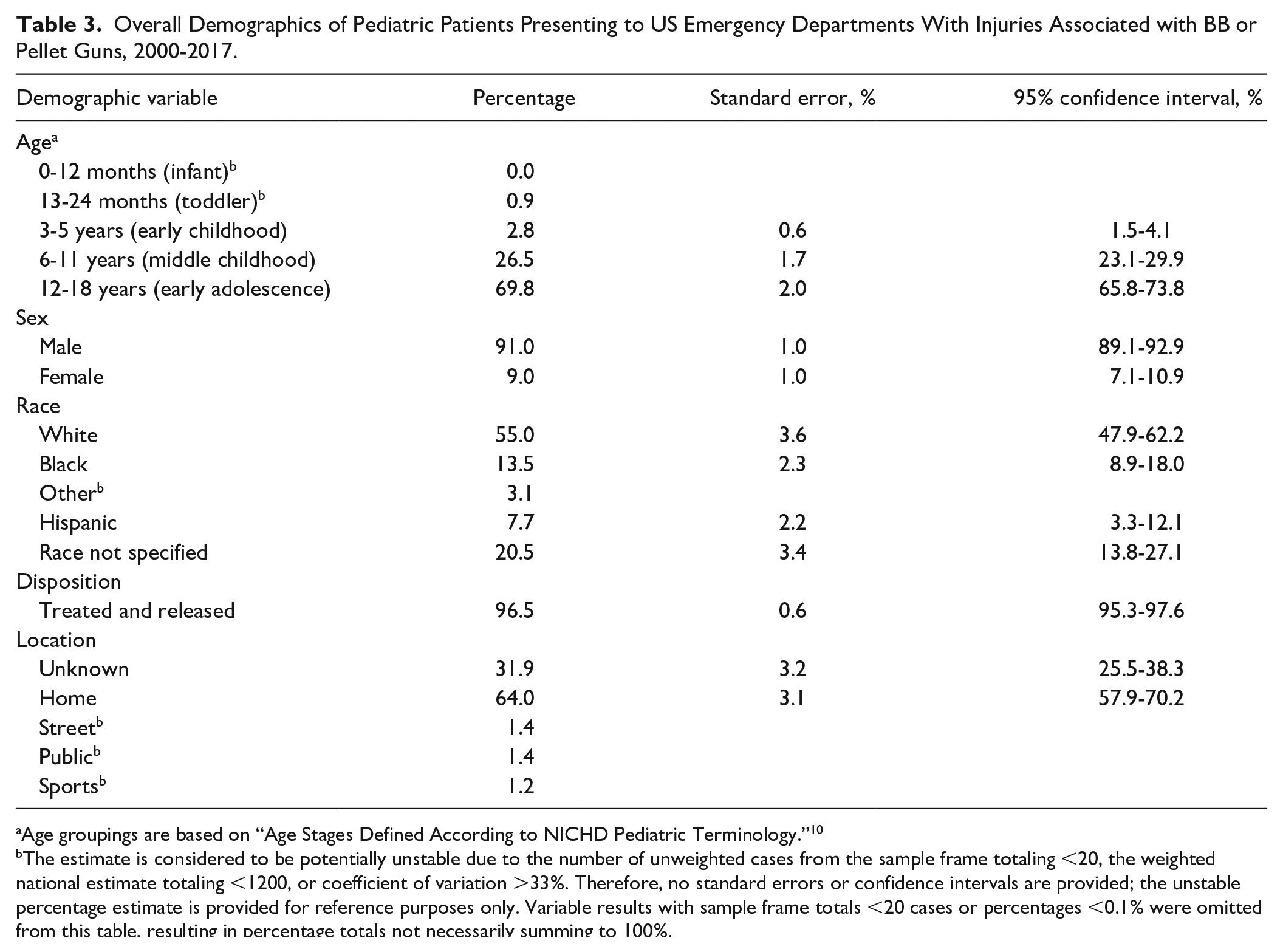
Age groupings are based on “Age Stages Defined According to NICHD Pediatric Terminology.” 10
The estimate is considered to be potentially unstable due to the number of unweighted cases from the sample frame totaling <20, the weighted national estimate totaling <1200, or coefficient of variation >33%. Therefore, no standard errors or confidence intervals are provided; the unstable percentage estimate is provided for reference purposes only. Variable results with sample frame totals <20 cases or percentages <0.1% were omitted from this table, resulting in percentage totals not necessarily summing to 100%.
Discussion
To date, there is a paucity of literature describing the epidemiology and impact of nonballistic firearm trauma to the upper extremity in the pediatric population. Both BB and pellet guns have the ability to cause significant morbidity in this population as evidenced by ballistic studies showing muzzle velocities surpassing low-caliber handguns and forensic studies showing that once penetration of the skin is achieved, a metal BB can penetrate the viscera 2 to 5 cm deep to the entry site. 8
This study attempts to elucidate the number of pediatric upper extremity nonballistic firearm trauma cases seen in the United States annually, describe the most common anatomical injury patterns, and highlight the demographics of the patients most commonly presenting with these injuries.
Although this study is specific to the upper extremity, the findings are consistent with similar studies looking at other sites of injury with nonballistic firearms. A study by Dandu et al 9 reports similar results when looking at head and neck trauma secondary to nonpowder firearms. In their study, the patients were overwhelmingly men (81%) with the same leading associated diagnoses of foreign body and laceration in the emergency department. It is interesting to note that their study reported a higher proportion of younger aged individuals, with 55% of head and neck injuries occurring between those aged 0 and 12 years compared with 69.8% of the hand injuries occurring between those aged 12 and 18 years. Therefore, it is reasonable to infer that the anatomical site of injury is likely associated with age and the ability of an individual to physically manipulate the firearm.
It is clear from the available literature that nonballistic firearm trauma causes a significant burden on the emergency department system in the United States and that the true prevalence of this type of trauma is underreported. Studies on the subject matter have called for increased education on the topic of nonballistic firearm safety. Despite attempts at education, our data demonstrate a consistent number of cases reported from year to year, as seen in Table 1.
There are several limitations to this study. As a retrospective study, it is inherently limited by the accuracy of the information available by the database queried. The NEISS database, while designed to be representative of the US health care system and generalizable on a population level, has its own limitations. First, it does not allow individual chart review for accuracy of included cases. Second, it allows for only 1 diagnosis code to be associated with each case. And finally, it is limited to emergency department visits only. These limitations are not surprising as, to our knowledge, injuries sustained from BB and pellet guns are voluntarily reported, unlike the mandatory reporting that occurs for ballistic injuries. As such, the number of cases reported in this article should be interpreted with the knowledge that the true burden of injury from nonballistic firearms is likely much greater.
With this in mind, future studies should compile all injuries secondary to nonballistic firearm trauma from BB and pellet guns with the aim to fully describe the burden of these traumas on our health care system, as well as have more concrete data from which to advocate a movement away from these weapons being classified as “toys.” In addition, future studies on the subject could investigate the financial burden associated with nonballistic firearm trauma by studying the associated rate of surgical subspecialist consults called to the emergency department and the resulting surgical interventions most commonly associated with these traumas.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This retrospective database study was institutional review board approved for a Health Insurance Portability and Accountability Act waiver.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.