
Abstract
Introduction
The incidence of flexor tendon injuries in pediatric patients has remained largely undocumented, with a frequency of 3.6 per 100 000 persons per year. 1 The pediatric literature demonstrates a higher prevalence of flexor tendon injuries in men, caused by sharp objects (glass or knife), mainly to the small finger in zone II.2-4 Several studies have shown that children have better outcomes than adults due to their increased vascularity, smaller vincula, and increased healing potential.4-7
Furthermore, in the last decades, WALANT (wide awake local anesthesia no tourniquet) surgery has increased in popularity.8,9 In adults, the repair of flexor tendon injuries performed under local anesthetic has been shown to be safe and cost-effective and is often followed by active motion rehabilitation protocols.8-11 Procedures performed under local anesthetic have several advantages, such as faster turnover times with significant cost benefit, decreased complication rates, and increased patient satisfaction.12-26 Yet no studies have examined whether anesthetic choice affects outcomes or complication rates for repair of flexor tendon injuries in children. In addition, the rehabilitation protocol varies in the pediatric population.27-31
Current methods for assessing the success of surgical repairs are based on objective measures or using patient-reported questionnaires. The American Society for Surgery of the Hand (ASSH) Total Active Motion (TAM) scores, Strickland TAM scores, and questionnaire-based Disabilities of the Arm, Shoulder, and Hand scores are the most prevalent methods of assessment. 32
The purpose of this study was to assess and determine factors associated with functional outcomes and complication rates after repair of pediatric flexor tendon injuries, including anesthetic choice.
Materials and Methods
After Research Ethics Board approval, a 10-year (2005-2015) retrospective study of all patients who presented to a tertiary pediatric hospital with a diagnosis of flexor tendon injury was conducted. All patients with tendon injuries are referred to our plastic surgery clinic as it is the main provider of primary, secondary, and tertiary specialized services in our catchment area of 2.5 million people. Patients were identified using the International Classification of Diseases, Tenth Revision, Canada (ICD-10-CA) codes (see the appendix). Patients were included if they were under the age of 18 and had 1 or more flexor tendon repairs. Patients were excluded if they did not receive surgical repair of their flexor tendon injury or had an associated avulsion fracture. Demographic variables included age, sex, and hand dominance. Clinical data collected included location and mechanism of injury, concomitant injuries, type and time of repair, type of anesthetic used (general anesthesia or local anesthesia), postoperative rehabilitation protocol, ASSH TAM scores, and complications.
The primary outcome was the documented TAM score. The TAM score is a validated tool, and an excellent score correlates to normal function, good to >75% function, fair to 50% to 75% function, poor to <50% function, and worse to less than their preoperative function. Total Active Motion scores were recorded during the follow-up appointments by our hand therapists. For patients who were lost to follow-up before 6 months, the last TAM score was recorded. If they did not have at least 1 follow-up documented with a TAM score, no TAM score was recorded. In cases where patients received a second procedure, such as a tenolysis, the best TAM score was recorded. Other outcomes of interest included development of complications and anesthetic choice.
Statistical Analysis
Demographic and clinical characteristics were summarized using descriptive statistics. As there were patients with more than 1 tendon injured and/or repaired, data from select variables were summed, and a proportion was determined accordingly (frequencies and percentage).
The primary analysis consisted of examining the predictors of the TAM score (excellent/good, fair, or poor), which was achieved by conducting a univariate analysis followed by a multivariate analysis using ordinal (proportional) regression analysis. Secondary analyses consisted of: (1) examining predictors of complication (yes/no) by conducting univariate and multivariate analyses using logistic regression; and (2) testing the association between anesthesia (local vs general) and age, sex, hand dominance, and complications; this was conducted using the Wilcoxon signed rank test for continuous variables and χ2 or Fisher test for categorical variables. Age, sex, hand dominance, concomitant injuries, anesthetic technique, total number of tendons repaired, repair time, and immobilization technique were the variables included in the models. These were predetermined and were all included in the multivariate models based on their clinical relevance.
Two-sided values of P < .05 were considered statistically significant. All statistical analyses were performed by a statistician using R statistical software version 3.4.2 1 (R Core Team, Vienna, Austria). 33
Results
Patient Demographics and Injury Characteristics
A total of 928 patients were identified with the ICD-10 diagnostic codes, and after reviewing the charts, only 109 patients had flexor tendon injuries treated at our institution. The remaining patients were excluded from the study. Patients ranged in age from 1 to 17 years (mean 12.2 ± 4.6 years) and were mainly right hand dominant (72 of 109 patients; 66%) and men (84 of 109 patients; 77%). There were a total of 162 digits injured, with the small finger being the most common (48 digits injured; 30%). There were 235 tendons injured at different levels: 92 flexor digitorum superficialis, 126 flexor digitorum profundus, and 17 flexor pollicis longus. The most common mechanism of injury was from a knife (46 of 109 patients; 42%); others included: glass (25 of 109 patients; 23%), sharp metal object (12 of 109 patients; 11%), or jersey finger (9 of 109 patients; 8%). Zone II was the most frequent zone where the flexor tendons were injured (82 of 159 zone injuries; 52%). There were 60 patients who had in total 119 concomitant injuries, and the most common concurrently injured structure was the digital nerve (57 of 119 concomitant injuries; 48%). In total, 47 patients reported no concomitant injuries. The mean time from injury to repair was 5 ± 7.6 days for the patients who presented within 30 days of the flexor tendon injury (100 patients). Nine of the 109 patients had a delayed presentation (after 30 days) and repair (mean time 187 ± 229 days) (Figure 1). Despite delayed presentation and repair, the patients had good (n = 8) or excellent (n = 1) outcomes.
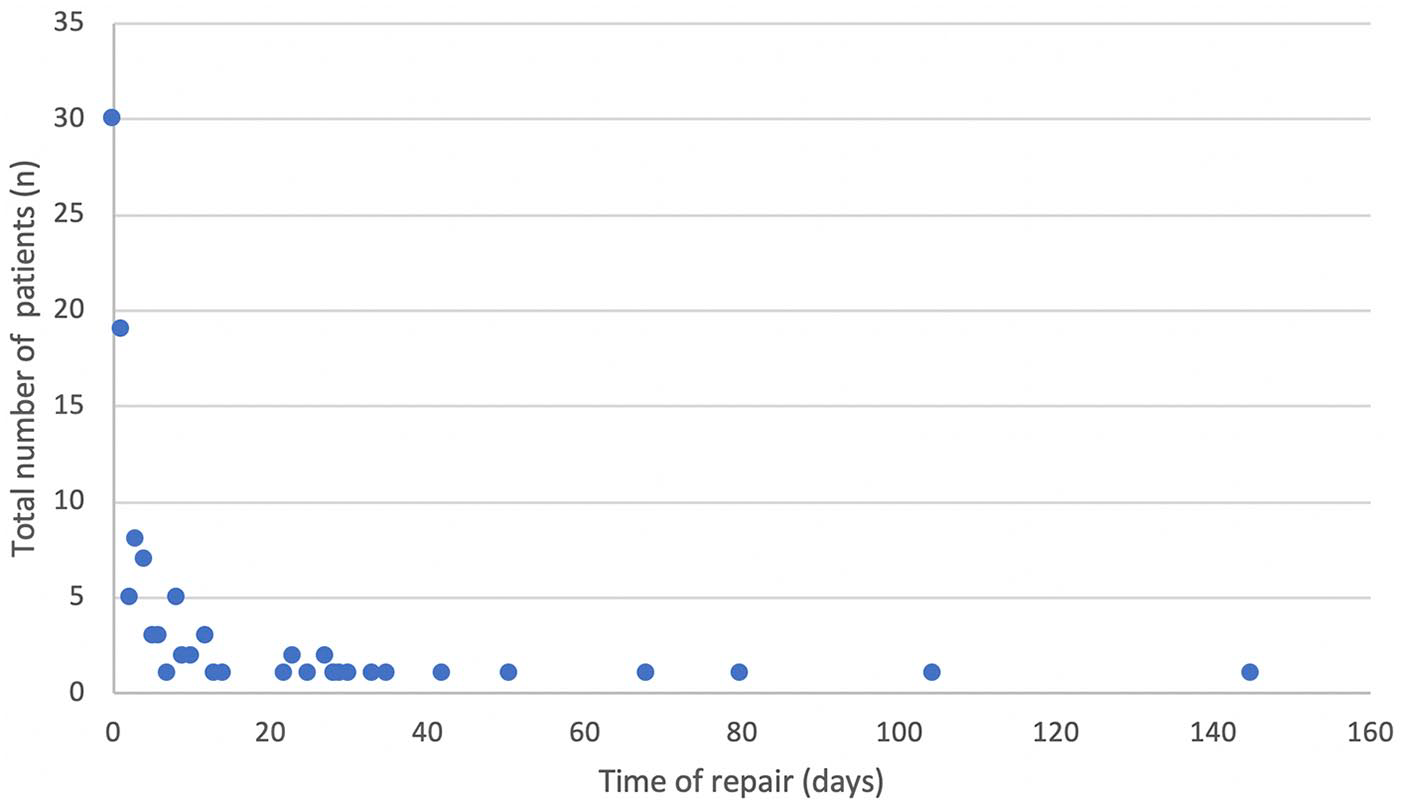
Time of repair from initial date of injury.
Anesthetic Choice
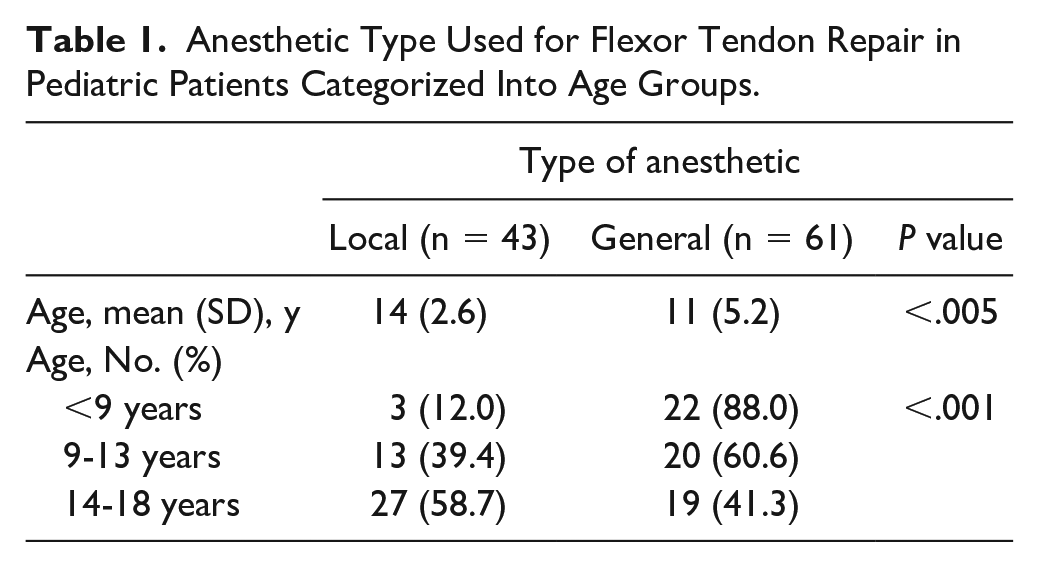
Local anesthetic was used in 43 (41%) and a combination of general and local in 61 (56%) of 104 patients; anesthetic choice was not identified in 5 patients. There was a significant association between age group and type of anesthesia used, general anesthesia being favored for children under the age of 13 years (P < .001) (Table 1).
Anesthetic Type Used for Flexor Tendon Repair in Pediatric Patients Categorized Into Age Groups.
Outcomes and Complications
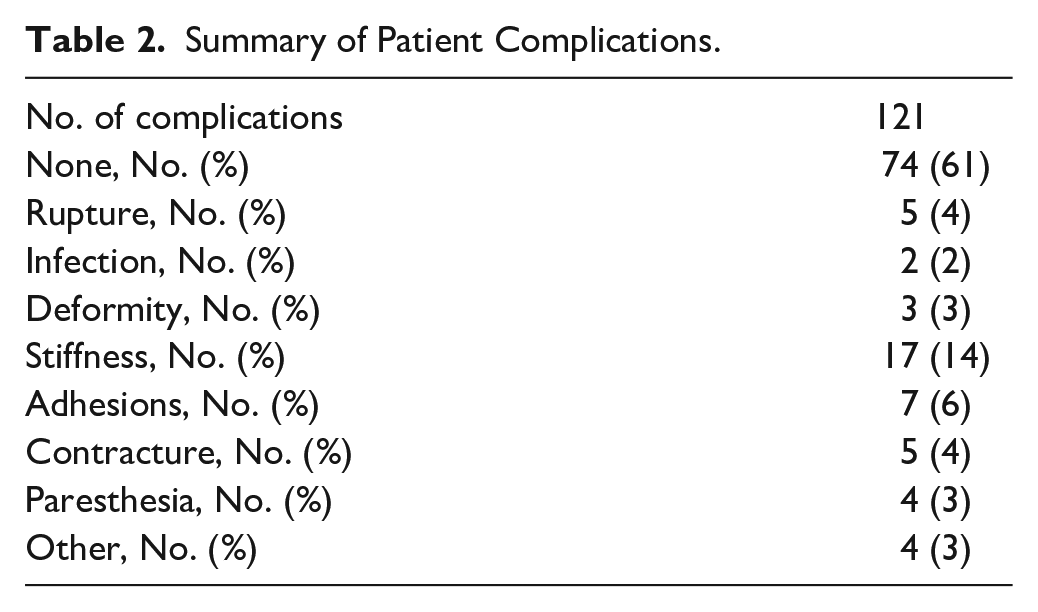
Methods of repair included: the Kessler technique (111 of 235 tendons), figure-of-eight knot (6 of 235), Strickland (4 of 235), and other (4 of 235); 10 of the 235 injuries were not repaired. Epitendinous repair was performed in 67 of the 225 total repairs. Overall, TAM outcomes were excellent or good in 95% of patients (excellent = 17, good = 86, fair = 4, poor = 1, lost to follow-up = 1). The most commonly reported postoperative complication was stiffness (n = 17 of 121 complications; 14%), with most patients having no complications (74 of 109 patients; 68%), demonstrating a documented rupture rate of 4% (Table 2). Tenolysis was documented in 13 patients (mean time after initial repair = 78 ± 59 weeks), with most of them showing good or excellent outcomes (n = 9). Of the 5 patients with fair and poor TAM scores, 4 required tenolysis, and 2 patients had postoperative rupture.
Summary of Patient Complications.
Postoperative Protocol
There were 85 patients who followed a postoperative protocol for 12 ± 18 weeks, the most frequent one being the Kleinert protocol (42 of 109 patients; 39%). A thermoplastic splint (93 of 109 patients; 85%) or cast (14 of 109 patients; 13%) was required for select patients, for a mean time of 8.4 ± 10 weeks.
There were no association between TAM score and age, sex, hand dominance, anesthetic choice, number of tendons repaired per patient, time of repair, or immobilization technique (Table 3). When controlling for other factors, concomitant injuries were a significant predictor of TAM score; patients who presented with concomitant injuries were 88% more likely to have a fair/poor TAM compared with the patients with no concomitant injuries (odds ratio [OR], 0.12; 95% confidence interval [CI], 0.02-0.49; P = .01). There was no association between complication rates and the following variables: sex, hand dominance, concomitant injuries, anesthetic choice, time of repair, and immobilization technique. When controlling for other factors, complication rates increased 1.59 times when more than 1 tendon was injured and repaired (OR, 1.59; 95% CI, 1.11-2.27; P = .01), whereas increasing age was found to be protective (OR, 0.86; 95% CI, 0.75-0.98; P = .03) (Table 4).
Univariate and Multivariate Analyses Between Select Characteristics and Total Active Motion Scores Using an Ordinal (Proportional) Regression Analysis.
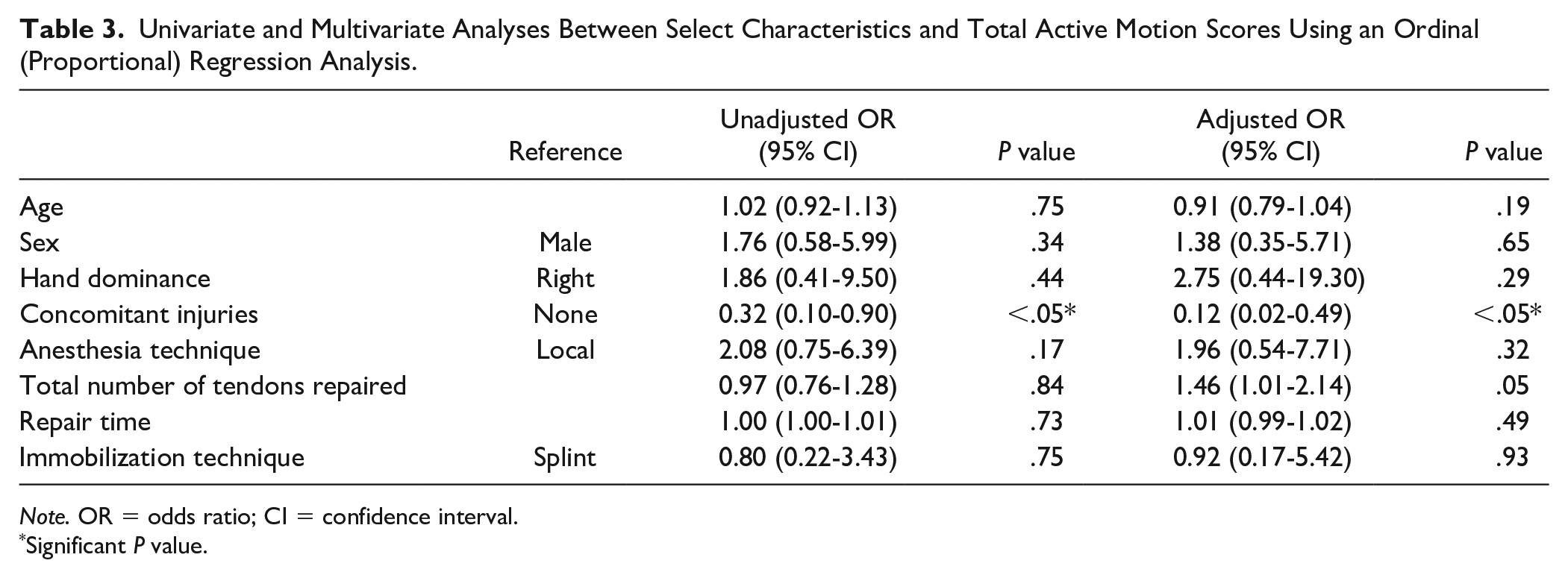
Note. OR = odds ratio; CI = confidence interval.
Significant P value.
Univariate and Multivariate Analyses Between Select Characteristics and Complications Using a Logistical Regression Analysis.
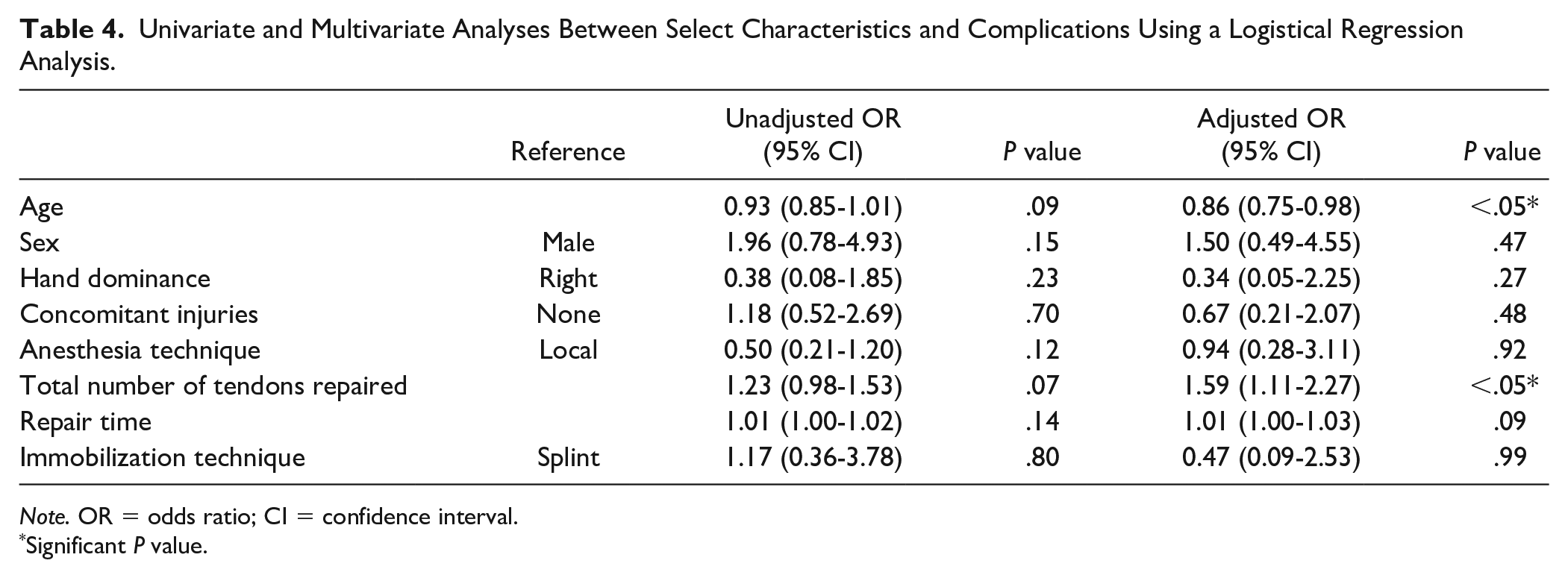
Note. OR = odds ratio; CI = confidence interval.
Significant P value.
Discussion
There is a paucity of evidence regarding outcomes after pediatric flexor tendon injuries; however, the current literature suggests that the results are favorable and may even be superior compared with adults.4-7
Patient Demographics and Mechanism of Injury
Our study cohort demographics were similar to the reported literature.1-4,34,35 Most patients were right-hand-dominant men, and the flexor tendon injuries were caused with a knife, to their small finger in zone II. Moreover, there was no association between the characteristics of our cohort or injury and the TAM scores or complication rates. Previously, the flexor tendon injuries in zone II were associated with poorer outcomes in adult and pediatric population.28,29,36,37 Recent studies support our findings that patient and injury characteristics may not necessarily correlate to poorer outcomes or higher rates of complications.2,28,38,39
Time of Repair
The mean time of repair was 5 days for patients who had a presentation within 30 days from injury. The causes of the 9 delayed repairs were initial misdiagnoses, delay in seeking treatment, or administrative referral errors. Of this delayed presentation group, all patients had good (n = 8) or excellent (n = 1) outcomes with delayed primary repair (n = 5) or tendon grafting (n = 4). Studies by Sikora et al 4 and Berndtsson and Ejeskär 29 also did not find an association between the time of tendon repair and poor outcomes in children.
Anesthetic Choice
This is the first study which reported outcomes after repair of flexor tendon injuries under the local anesthetic in children. Traditionally, patients above the age of 8 may receive local anesthetic, but patients younger would routinely be given general anesthesia due to concerns of compliance. General anesthetic with or without local anesthetic (59%) was more commonly used than local anesthetic alone (41%). The mean age of patients who received local anesthetic was significantly older (mean age = 14.1 ± 2.6, range = 7-17 years) than the general anesthetic group (mean age = 10.7 ± 5.2, range = 1-17 years). Most importantly, there were no decreased TAM scores or increased incidence of complications.
Local anesthetic has been reported to be a cost-effective12-14,19,22 and safe15,17,18,20,26 option with similar outcomes 25 to general anesthetic in the adult population. Several studies have examined the cost-effectiveness of local anesthetic. The studies12,14,22 have demonstrated significant cost and time reductions using the local anesthetic compared with the general anesthetic. 13
Conversely, there is a substantial body of literature that supports the safety of performing hand procedures under local anesthetic with and without epinephrine.16,24 Lalonde et al 18 and Chowdhry et al 15 performed large retrospective reviews which demonstrated no instances of digital infarction or serious complications from administration of local anesthetic in the digits. Therefore, the literature indicates that local anesthetic with epinephrine is safe to use in the digits.16,17,21,24,25
In our study, there were a total of 39 patients older than 8 years who received general anesthesia. These may be due to concurrent multiple digit injury, anxiety, and potential lack of cooperation.
Outcomes and Complications
The Kessler technique was the most performed method of repair in our study as previously reported, and 67 had an epitendinous repair as well.1,3,4,28 The benefit of epitendinous repair in pediatric flexor tendons is equivocal. Sikora et al 4 reported only 22 of their 100 flexor tendon repairs received epitendinous repairs in contrast to Cooper et al 3 who performed 75 epitendinous repairs in their sample of 99 flexor tendon injuries; both cohorts did not find an association between epitendinous repairs and outcomes. Therefore, the benefits of epitendinous repairs for pediatric flexor tendons or their impact on complications and functional outcomes is still unclear. Further studies with larger cohorts are needed.
Most patients (95%) had either excellent or good TAM scores, with the most common postoperative complication being stiffness. Patients who had concomitant injuries or multiple tendon repairs were more likely to have poorer TAM scores or increased likelihood of complications, respectively. This is in contrast to the study performed by Cooper et al 3 who did not find an association with concomitant injuries and outcomes. No other study, however, has examined the relationship between concomitant injuries or number of tendons repaired and outcomes or complications. Our study is the only one that indicated that age is a protective factor, whereas Sikora et al 4 and Cooper et al 3 did not find an association with age.
Furthermore, the sample size of patients who had fair or poor outcomes was too small (n = 5) to identify any predictive factors. Moreover, our data most likely underestimated patient outcomes due to variability in documentation and loss to follow-up. Many patients were discharged earlier than 6 months after repair. May and Silfverskiold indicated that the improvement in the range of motion typically continues after the first 6 months and reaches a plateau at 12 months. 40 Due to the lack of stringent documentation in patient charts (lack of explicitly stating “return to normal function”), we frequently downgraded the TAM score from excellent to good outcome. Therefore, there most likely exist a large number of patients whose TAM scores would be higher if they were reassessed at 6 months with more stringent documentation.
Postoperative Protocol
Rehabilitation protocols varied considerably, with the Kleinert protocol being the most popular postoperative protocol. The subset of patients who were completely immobilized (cast = 16) had good or excellent outcomes.
Limitations
The outcomes were measured retrospectively using only documented TAM scores. Although TAM scores provide a quantitative method of measuring outcomes, qualitative factors such as grip strength or sensation were not included. Therefore, other factors that may be important for meaningful hand function may not have been encompassed. Until a comprehensive tool that includes quantitative and qualitative measures is developed, there will remain a clinical equipoise on the best method of outcome assessment. Patients were also assumed to have a normal contralateral finger when assessing TAM scores. Due to the retrospective nature of the study, lack of stringent documentation may have influenced our results, and a prospective design would be the ideal method to assess patient outcomes. However, due to the low incidence of flexor tendon injuries in pediatric population (109 patients identified over a 10-year period), it may be difficult to conduct a prospective study unless a multicenter study across Canada is performed.
Footnotes
Appendix
Acknowledgements
The authors thank Sonam Maghera for her assistance in data acquisition and cleaning, as well as Lamia Al-Tekreeti for her assistance with data analysis.
Authors’ Note
This work was presented at the British Society for Surgery of the Hand (BSSH) 2016 in Cardiff, UK (partial results); the Canadian Society of Plastic Surgery (CSPS) 2018 in Jasper, Alberta (partial results); and the American Society for Surgery of the Hand (ASSH) 2018 in Boston, Massachusetts (partial results).
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
No informed consent was required for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.