
Abstract
Background:
The Rhode Island State Legislature passed the Uniform Controlled Substances Act in 2016 to limit opioid prescriptions. We aimed to objectively evaluate its effect on opioid prescribing for hand surgery patients and also identify risk factors for prolonged opioid use.
Methods:
A 6-month period (January-June 2016) prior to passage of the law was compared with a period following its implementation (July-December 2017). Thumb carpometacarpal arthroplasty and distal radius fracture fixation were classified as “major surgery” and carpal tunnel and trigger finger release as “minor surgery.” Prescription Drug Monitoring Database was used to review controlled substances filled during the study periods.
Results:
A total of 1380 patients met our inclusion criteria, with 644 prelaw and 736 postlaw patients. Patients undergoing “major surgery” saw a significant decrease in the number of pills issued in the first postoperative prescription (41.1 vs 21.0) and a corresponding decrease in morphine milligram equivalents (MMEs) (318.6 vs 159.2 MMEs) after implementation. A 30% decrease in MMEs was also seen in those undergoing “major surgery” in the first 30 days postoperatively (544.7 vs 381.7 MMEs). Risk factors for prolonged opioid use included male sex and preoperative opioid use.
Conclusions:
In Rhode Island, opioid-limiting legislation resulted in a significant decrease in the number of pills and MMEs of the initial prescription and a 30% decrease in total MMEs in the 30-day postoperative period after “major hand surgery.” Additional research is needed to explore the association between legislation and clinical outcomes.
Introduction
Individuals of every class, race, and social status are affected by the current opioid crisis in the United States. Opioid overdoses accounted for over 350 000 American deaths from 1999 to 2016. Furthermore, overdoses related to opioids increased by a factor of 5 between 2009 and 2016. 1
Opioid abuse is now recognized by both the medical community and society at large as a formidable issue. In a recent poll, opioids ranked sixth among all domestic priorities,2,3,4 with 81% of Americans believing that the opioid epidemic is either a major problem or a national emergency. In addition, President Donald Trump has declared the opioid epidemic a “public health emergency” and has directed the executive government to use “every appropriate emergency authority” to fight the crisis.5,6 When asked who was primarily responsible for the problem of prescription-painkiller or opiate abuse, the plurality of survey respondents (33%) blamed physicians. 4 Hence, health care providers must take an active role in fighting this epidemic.
Orthopedic surgeons play a large role in opioid prescription, especially in the postoperative patient. Roughly 7.7% of all narcotic prescriptions are written by orthopedists, a group that only accounts for 2.5% of all physicians in the United States. 7 In an attempt to address this crisis, multiple states have instituted statewide opioid prescription limits.8,9 However, given the relatively recent implementation, there is limited evidence evaluating the efficacy of such legislative measures. The need for such research is eminently clear.9,10
In the state of Rhode Island, legislation was passed in June 2016 designed to address the opioid epidemic in a number of ways, including the implementation of strict opioid prescription limits on providers. The limits permitted no more than 30 morphine milligram equivalents (MMEs) per day and no more than 20 doses total for the first narcotic prescription in an opioid-naïve patient. 11 This is equivalent to a maximum of 6 doses of 5 mg hydrocodone per day, or 4 doses of 5 mg oxycodone daily for 20 doses total. Exceptions were made for chronic pain, palliative care, nursing home care, and cancer pain. For the purposes of this study, patients were defined as “chronic opioid users” if they had an opioid prescription in the 30 days prior to their surgery. In addition, the legislation mandated review of the State’s Prescription Drug Monitoring Program (PDMP) prior to beginning an opioid regimen and every 3 months thereafter by all prescribers. Through the study of the Rhode Island model, this investigation aims to objectively evaluate the effect of narcotic-limiting legislation on opioid prescription patterns for patients undergoing 4 common hand surgeries.
Methods
Institutional review board approval both from our institution and from the Rhode Island State Department of Health was obtained prior to beginning this investigation. A bill that imposed mandatory opioid prescribing limits in Rhode Island, as described above, was passed in June 2016. We selected a 6-month period (January 1, 2016-June 30, 2016) prior to passage of the bill to compare the opioid prescribing patterns of that period with a 6-month period following implementation of these mandates (July 1, 2017-December 31, 2017). Retrospective review of our institution’s billing database using Current Procedural Terminology (CPT) codes for 4 common surgeries typically performed by hand surgeons was completed. The surgeries and their associated CPT codes that were included for analysis are listed here: thumb carpometacarpal (CMC) arthroplasty (25210, 25447), carpal tunnel release (CTR; 64721), trigger finger release (TFR; 26055), and distal radius (DR) fracture fixation (25607, 25608, 25609). We grouped CTR and TFR for analysis as “minor” surgeries given they typically require less postoperative narcotic pain medication when compared with thumb CMC arthroplasty or DR fracture.12,13 The latter group was labeled “major” surgery. We excluded any patients under the age of 18, those who had multiple surgeries under the same anesthesia, and those who could not be found in the Rhode Island PDMP database.
For all patients included in the study, demographic and surgical data were collected from their medical charts. The Rhode Island PDMP database was used to review prescriptions of all controlled substances filled during the 2 study periods. In addition, the database was reviewed for any opioid or benzodiazepine prescriptions in the 30-day preoperative period. Data on all oral formulations of morphine, hydrocodone, oxycodone, codeine, hydromorphone, and tramadol were collected and converted to MMEs 14 for the 90 days after the patient’s surgery date. Specific benzodiazepines evaluated included alprazolam, chlordiazepoxide, clonazepam, clorazepate, diazepam, flurazepam, lorazepam, quazepam, temazepam, and triazolam. Patients were considered opioid-naïve if they did not receive any narcotic prescriptions in the 30-day preoperative period, with the exception of DR fracture patients, where the window from day 30 to day 14 prior to the surgery date was used to evaluate for opioid naivety. This time period was selected to account for narcotic prescriptions filled after injury but preoperatively, for someone who would otherwise be considered opioid-naïve. For the purposes of this study, patients were considered opioid-tolerant if they had opioids prescribed and filled in the 30 days prior to the surgery date, except for the DR fracture patients, as described above.
For all patients, we collected the number of pills and total MMEs of the first postoperative script, the number of individual prescriptions and total MMEs filled within 30 days of surgery, and the total MMEs filled 30 to 90 days after surgery. Prolonged opioid use was defined as any opioids prescribed in the 30- to 90-day postoperative window. We used the 90-day cutoff in the postoperative period to exclude confounding variables such as unrelated injuries or surgeries that may affect our analysis.
For continuous variables, t test or Mann-Whitney U test was used as appropriate. χ2 analysis was used for comparison of categorical variables. Logistic regression was performed to determine independent risk factors for prolonged postoperative opioid use. All statistical analyses were performed using Stata (College Station, Texas).
Results
Patient Population
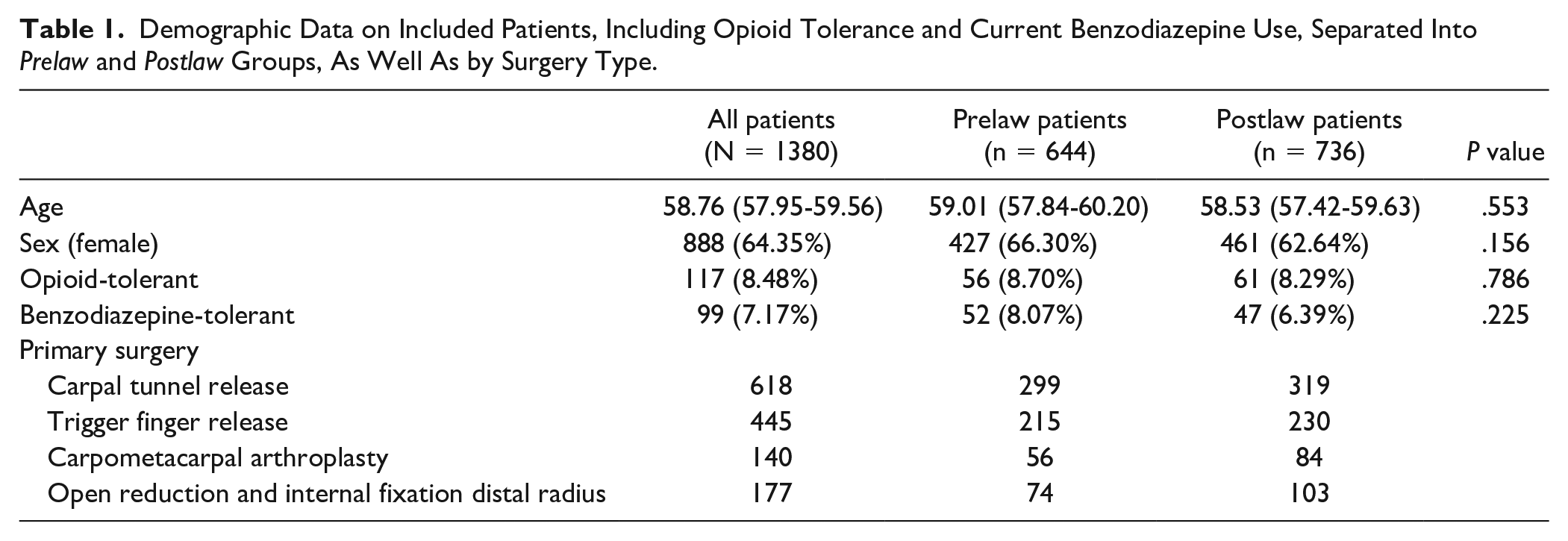
A total of 1380 patients met inclusion criteria, including 644 patients from the prelaw period and 736 patients from the postlaw period. There were no significant differences found between the prelaw and postlaw patient groups in terms of age, sex, opioid tolerance, or recent benzodiazepine use (P > .05; Table 1). The mean age of all participants was 58.76 (95% confidence interval [CI], 57.9-59.6). Approximately 8.5% of all patients were classified as opioid-tolerant, and 7.2% had recently been prescribed benzodiazepines (Table 1). The number of patients stratified by type of surgery performed is also displayed in Table 1.
Demographic Data on Included Patients, Including Opioid Tolerance and Current Benzodiazepine Use, Separated Into Prelaw and Postlaw Groups, As Well As by Surgery Type.
Initial Prescription
In comparison with the prelaw group, a significant decline in the mean number of pills issued in the first postoperative prescription for all patients was observed in the postlaw period (21.6 vs 16.6 pills, P < .05). This difference was also observed across surgeries categorized as “major surgery” (40.7 vs 21.0 pills, P < .05). However, this statistically significant decrease was not seen after procedures categorized as “minor surgery” (16.9 vs 15.1 pills, P = .14; Table 2). A corresponding decrease in the first prescription total MMEs was also observed only in the “major surgery” group (318.6 vs 159.2 MMEs, P < .05; Figure 1 and Table 2). No statistical difference was seen in the MMEs prescribed in the first opioid script for those in the “minor surgery” group (98.7 vs 105.4 MMEs, P = .48).
Detailed Comparisons of Opioid Prescriptions for All Included Patients and Stratified by Procedure Performed, Including “Minor” and “Major” Surgery Groups. Comparisons Made Between Prelaw and Postlaw Cohorts.
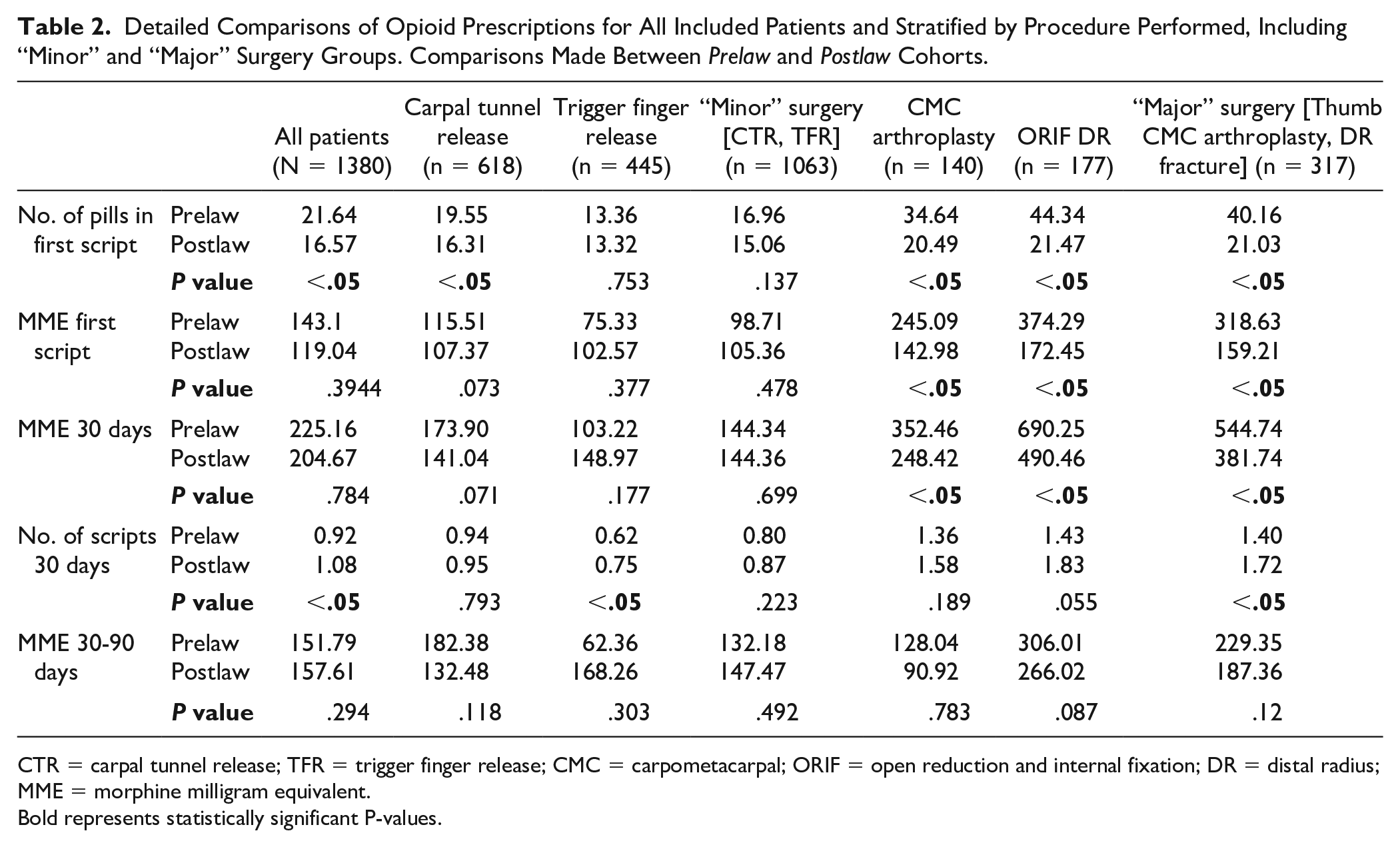
CTR = carpal tunnel release; TFR = trigger finger release; CMC = carpometacarpal; ORIF = open reduction and internal fixation; DR = distal radius; MME = morphine milligram equivalent.
Bold represents statistically significant P-values.
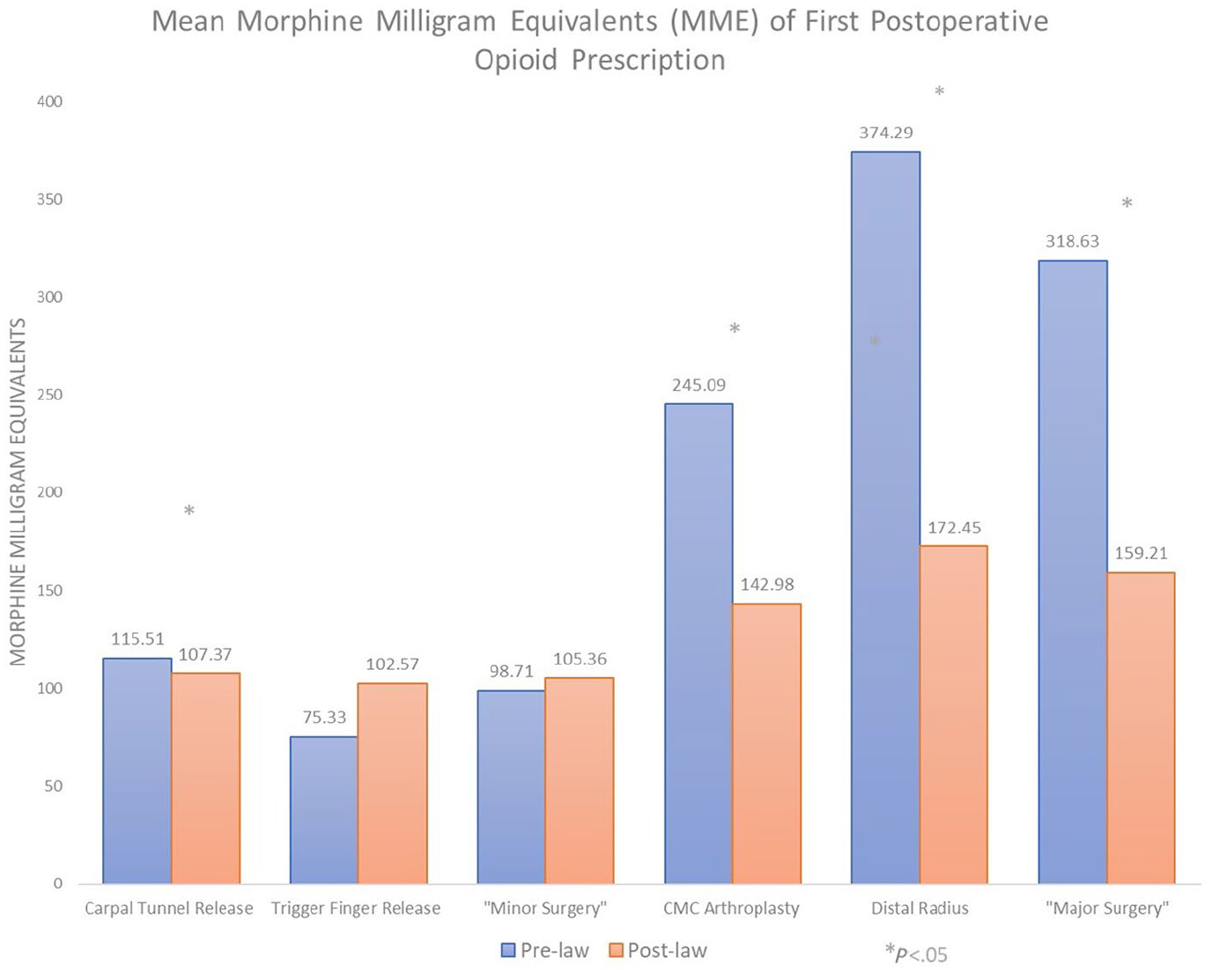
Effect of narcotic-limiting legislation on the MMEs prescribed in the first opioid prescription following hand surgery.
Opioid-tolerant patients were prescribed a greater mean number of pills in their first postoperative prescription prior to the passage of the narcotic-limiting law when compared with opioid-naïve patients (37.2 vs 20.2 pills, P < .05). Both groups showed a significant decrease in the number of pills in the first prescription postlaw (26.7 and 15.7 pills, respectively; P < .05 and P < .05; Supplemental Table 1).
First 30 Days After Surgery
Significant reductions of roughly 30% in the MMEs prescribed within the first 30 days were observed for patients in the “major surgery” group when comparing the prelaw with the postlaw group (544.7 vs 381.7 MMEs, P < .05; Table 2, Figure 2). The MMEs and the number of prescriptions were similar in the “minor surgery” group between the 2 time periods (Table 2).
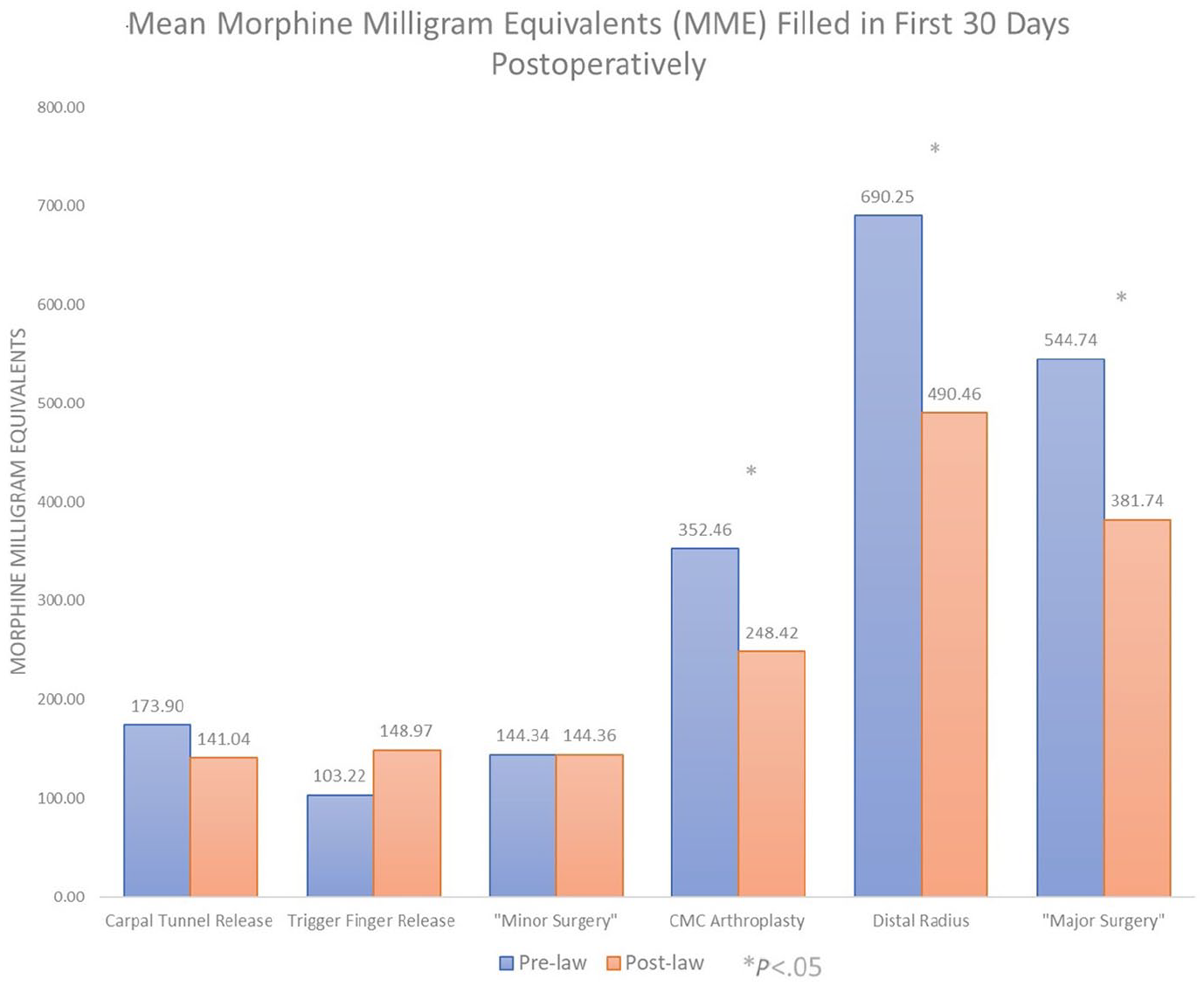
Effect of narcotic-limiting legislation on the MMEs prescribed in the 30 days following hand surgery.
No statistically significant change in the total MMEs filled in the first 30 postoperative days was observed within either the opioid-tolerant or opioid-naïve group after the law was passed (P > .05). Opioid-tolerant patients were prescribed 3.4 to 4.1 times as many MMEs as opioid-naïve patients within 30 days of surgery (Supplemental Table 1, Figure 3).
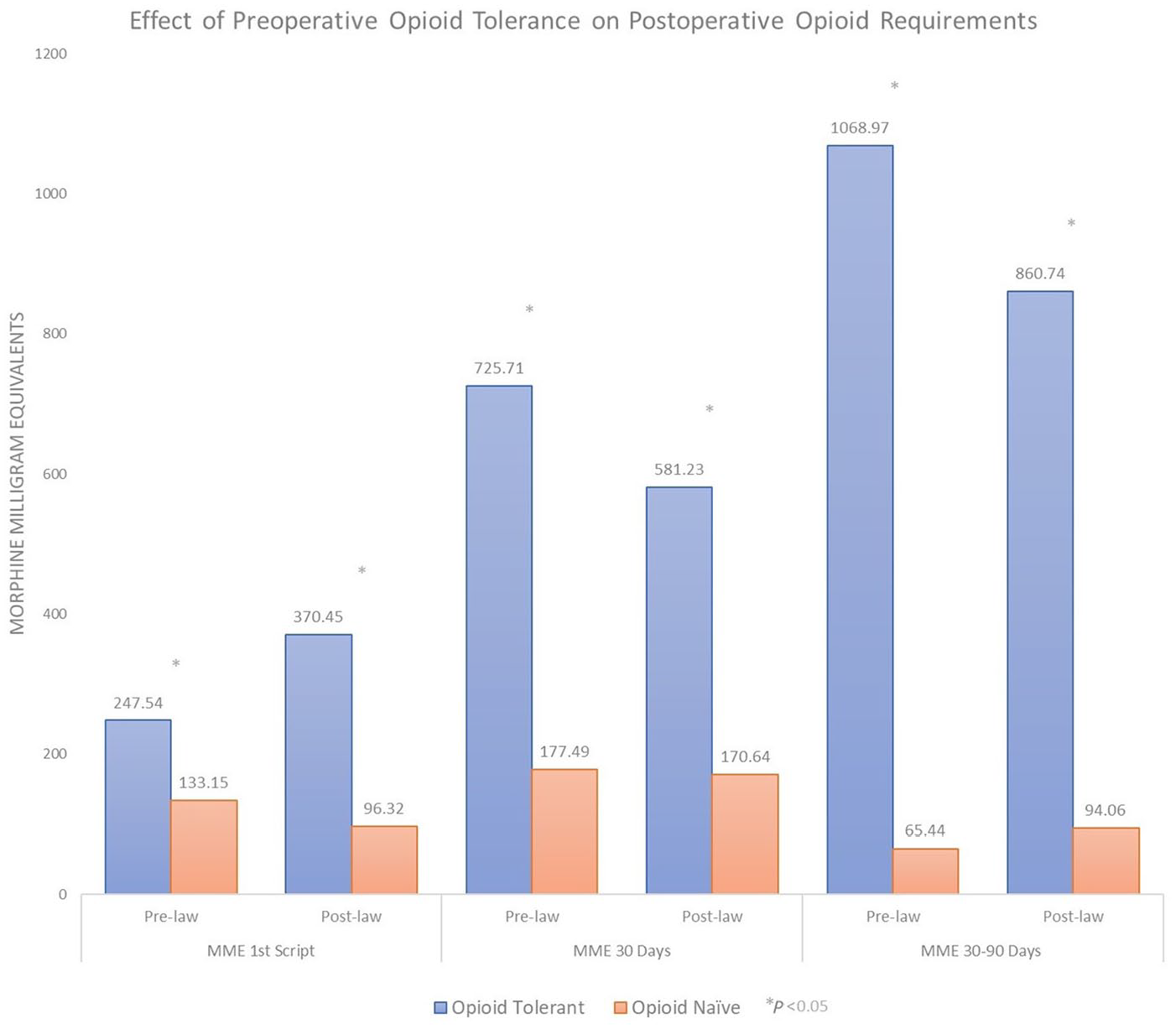
Effect of preoperative opioid tolerance or naivety on postoperative opioid requirements following hand surgery.
30 to 90 Days After Surgery and Prolonged Use
There was no significant difference between prelaw and postlaw cohorts in terms of MMEs issued during the 30- to 90-day postoperative period, across all procedures and groups (all Ps > .05; Supplemental Table 1). In both prelaw and postlaw periods, the opioid-tolerant group showed greater mean number of prescriptions and issued MMEs in the 30- to 90-day postoperative period compared with the opioid-naïve group (all Ps < .05; Supplemental Table 1, Figure 3).
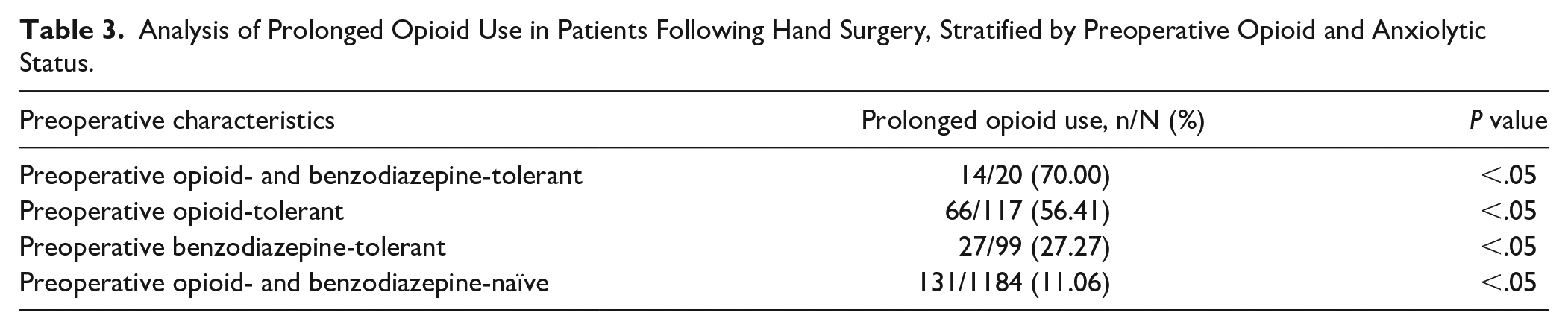
Of the patients who were preoperatively opioid-tolerant, 56.4% (66 of 117; P < .05) demonstrated prolonged opioid use following surgery. Roughly 27.3% (27 of 99; P < .05) of patients who were preoperatively benzodiazepine-tolerant demonstrated prolonged opioid use postoperatively. These effects were additive: Patients who were preoperatively both opioid- and benzodiazepine-tolerant showed prolonged opioid use following surgery 70.0% of the time (14 of 20; P < .05). Comparatively, those who were preoperatively opioid- and benzodiazepine-naïve demonstrated prolonged opioid use only 11.1% of the time (131 of 1184; P < .05; Table 3).
Analysis of Prolonged Opioid Use in Patients Following Hand Surgery, Stratified by Preoperative Opioid and Anxiolytic Status.
After controlling for potential confounders, including age, sex, preoperative opioid use, preoperative benzodiazepine use, and surgical procedure, the factor most strongly predictive of the need for prolonged postoperative opioid requirement was preoperative opioid use (odds ratio [OR] = 11.5, 95% CI, 7.5-17.6, P < .05). Male sex was also predictive of prolonged postoperative opioid use (OR = 1.4, 95% CI, 1.0-1.9, P < .05). Patients who had surgery for fixation of their DR fracture were also noted to have a higher propensity for needing prolonged postoperative opioids (OR = 3.6, 95% CI, 2.3-5.5, P < .05). Age (P = .67) and preoperative benzodiazepine use (P = .08) were not significantly associated with prolonged opioid use following surgery (Table 4).
Logistic Regression Evaluating Independent Risk Factors for Prolonged Opioid Use.
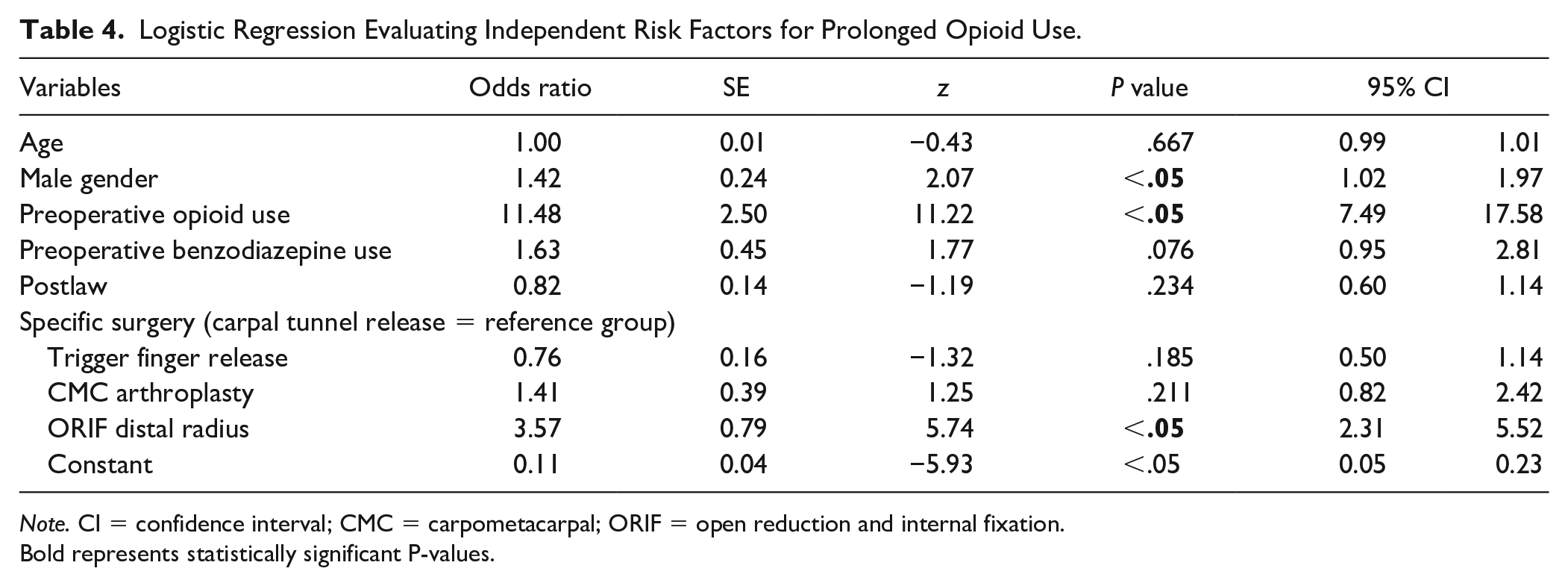
Note. CI = confidence interval; CMC = carpometacarpal; ORIF = open reduction and internal fixation.
Bold represents statistically significant P-values.
Discussion
Between 2009 and 2016, overdoses related to opioid use rose by approximately 500%, and 66% of all US overdose deaths in 2016 involved an opioid. 1 Prescription opioids are strongly associated with later heroin use. According to the National Survey on Drug Use and Health (NSDUH), 80% of active heroin users in 2013 reported that their opioid use began with prescription opioids. 15 Orthopedic surgeons are responsible for a disproportionate contribution to overall opioid prescription. 7 Specific to hand and upper extremity surgeries, some researchers suggest that patients may be receiving roughly 3 times as many opioids as needed based on the number of pills actually used. 16 Some have shown that up to 4 to 5 times as many pills are being prescribed following CTR than needed by patients for pain control.17,18
This investigation offers preliminary evidence that Rhode Island’s statewide implementation of opioid prescription limits has been successful in reducing opioid prescription in the early postoperative period following hand surgery. Following the implementation of the law, we observed a significant reduction in the MMEs of the initial prescription (51% reduction) as well as the MMEs prescribed within 30 days (30% reduction) for patients undergoing “major” hand surgery (CMC arthroplasty or DR open reduction and internal fixation [ORIF]). The 163.0 MME postlaw reduction in the 30 days following surgery in this group equates to roughly 22 fewer oxycodone 5 mg pills issued per patient compared with the prelaw period. For the 317 patients in this group, this translates to roughly 6889 fewer oxycodone 5 mg tablets dispensed in the 30-day postoperative period following the implementation of the law. This could be extrapolated to roughly 2.2 million fewer oxycodone 5 mg tablets prescribed per 100 000 patients. This reduction in the opioid medication may help limit the risk of opioid diversion. Opioid diversion refers to the use of prescription opioids by persons other than the patient to whom it was prescribed or its sale in illicit markets for illegal use.19,20 Studies have shown that over half of those who abuse prescription opioid tablets for recreational use report obtaining them from a friend or relative, whereas less than 5% obtained them from a drug dealer or other stranger. 21
Interestingly, the statistically significant changes seen for patients undergoing “major hand surgery” did not hold for the “minor” surgeries included in this study. The differences seen in the number of pills prescribed in the first postoperative script and MMEs of the initial prescription and in the first 30 days between prelaw and postlaw groups for patients undergoing CTR and TFR were clinically insignificant, despite some comparisons reaching statistical significance, likely due to the large number of patients. Patients undergoing the TFR, arguably a minor procedure without significant expectations of postoperative pain, had a low number of prescribed pills even in the prelaw time frame. The state law did not lead prescribers to change their prescription patterns as their current habits fell within the purview of the legislation. Peters et al 18 prospectively evaluated patients undergoing carpal tunnel surgery on an outpatient basis and noted that, on average, patients only used 10 pills out of the 40 pills of the opioid prescribed. Similarly, Dwyer et al 12 investigated the use of patient education material in the use of opioid medication postoperatively and noted that after the intervention, patients consumed 3 opioid pills after CTR and 25 opioid pills after DR ORIF. Earp et al 13 demonstrated that the implementation of more conservative institutional guidelines for postoperative opioid prescription resulted in mean 90-day postintervention totals of 39.2 MMEs prescribed for minor surgeries, including CTR and TFR, and 208.1 MMEs for more major surgeries, including DR ORIF and CMC arthroplasty. These numbers are lower or similar to the doses patients in this study were prescribed after the law was implemented, suggesting that the initial script of no more than 150 MMEs may be sufficient for postoperative pain control.
While it is unclear how many pills the patients used for pain control in the postoperative period, the implementation of the law decreased the opioids that are dispensed from the pharmacy, and it can be inferred that the patients potentially used less medications for pain control after the operation as less pills were available to them. More importantly, however, the reduction seen in the opioid medications dispensed in the postlaw period may help to reduce the risk of opioid diversion in the community. A 2015 study showed that among those using opioids for recreational or nonmedical reasons, 67.6% had obtained them from a friend or relative. 22 Furthermore, among those friends and relatives, 83.8% reported obtaining the opioids in question from a single doctor. 23
For both opioid-tolerant and opioid-naïve patients, the number of pills issued in the first prescription decreased significantly following the passage of the law. This is notable because while the legislation explicitly designated opioid-tolerant patients exempt from the mandatory prescription limits, the results show that this patient group has nevertheless seen a reduction in initial pill number. Such findings may indicate a shift in physician and pharmacy opioid prescribing habits for all patients regardless of the prior opioid status, perhaps consistent with increased utilization of PDMP databases in the assessment of patients’ history of opioid prescription.24-26 In addition, both pill number and MMEs were greater for opioid-tolerant patients than for opioid-naïve patients both before and after the passage of the law. This pattern may further suggest that prior opioid status may indeed factor into clinical decision making, at least in the context of postoperative care following hand surgery. Overall, there was a slight decrease in MMEs issued in the first 30 days for both groups, but these changes did not reach statistical significance, indicating that stratification across procedure type rather than opioid status better illustrated postlaw changes in opioid prescription patterns in the first 30 days. Notably, however, there was a significant reduction in the mean MMEs issued to opioid-tolerant patients in the 30- to 90-day postoperative period following the passage of the law. This 19.5% decrease provides preliminary evidence that Rhode Island’s opioid-limiting legislation may have helped to reduce chronic opioid use in patients with a recent history of opioid consumption.
This study used information available from the Rhode Island PDMP database, which provided accurate and comprehensive data regarding all controlled substance prescriptions issued in Rhode Island and the surrounding states. Access to these data from 2 distinct time periods—before and after the implementation of opioid-limiting legislation—allowed for the semiexperimental nature of this study and strengthened the validity of its findings. The study benefited from access to detailed demographic data collected from patient charts, combined with longitudinal prescription records for all patients.
There are several potential limitations of this study that are worth discussing. We did not collect pain scores or other clinometric outcomes for the enrolled patients, which would allow investigation into the association between these outcomes and opioid prescription patterns. Also uncaptured by the study were complications, unplanned emergency department visits, or opioids obtained from illicit sources. This study was performed at a time when there is growing recognition among patients and providers alike of the potential for opioid misuse and abuse. Although it is possible that broader medical trends toward more conservative opioid prescription may have contributed to our findings, it is unlikely that epidemiologic trends alone could account for the significant decline in opioid prescriptions in such a short interval following the implementation of new legislation. Finally, through investigation of the number of opioid pills and MMEs filled by patients at pharmacies, this study deduced these patients’ actual use of opioids for postoperative pain management. In reality, we cannot make any determinations about how many of these pills were actually consumed by the patients during the period of study. Further research investigating patterns of opioid utilization and patient outcomes is needed. Regardless, the findings of this study suggest that Rhode Island’s narcotic-limiting legislation significantly reduced the number of opioid pills prescribed and filled across the state for those undergoing surgeries we classified as “major,” an effect with significant implications for public health.
Supplemental Material
sj-pdf-1-han-10.1177_1558944720988132 – Supplemental material for Is Opioid-Limiting Legislation Effective for Hand Surgery Patients?
Supplemental material, sj-pdf-1-han-10.1177_1558944720988132 for Is Opioid-Limiting Legislation Effective for Hand Surgery Patients? by Kalpit N. Shah, Daniel B. C. Reid, Jack H. Ruddell, Benjamin H. Shapiro, Peter James, Joseph A. Gil, Alan H. Daniels and Edward Akelman in HAND
Footnotes
Ethical Approval
Institutional review board approval was obtained at all participating institutions for collection and analysis of patient data.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
A waiver of informed consent was obtained from the institutional review board to approve this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.A. receives royalties from Integra Medical. A.H.D. receives royalties from Springer; consulting fees from Stryker, Globus, Orthofix, Spineart, DePuy; and research and fellowship support from Orthofix. The remaining authors have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.