
Abstract
Background
Scaphoid nonunion can occur in up to 55% of displaced scaphoid fractures. Long-term functional outcomes of this injury are lacking. In addition, no study has published rate of return to active military service after this injury. Our goal was to educate providers and patients on expected functional outcomes and return to duty after treatment of scaphoid nonunion.
Methods
We conducted a retrospective review of patients who underwent scaphoid nonunion repair at our institution from 2008 to 2017. The primary outcome measures were union rates, return to duty rates, and functional outcome scores obtained by telephone call. A total of 144 patients were included and 40 responded to our call for long-term follow-up.
Results
A total of 72% of patients achieved union after surgery, 18% required revision surgery, and 74% of patients were able to return to full duty after surgery. However, this number progressively decreased at 1, 2, and 5 years after surgery. At an average of 5.9 years after surgery, the mean Quick Disabilities of the Arm, Shoulder, and Hand (qDASH) score was 23.9. The mean qDASH for patients who achieved union (21.9) was significantly lower than those with persistent nonunion (29.2) (P = .0115).
Conclusion
Scaphoid nonunion is a difficult problem in the military. We found a high rate of persistent nonunion often requiring revision to partial or full wrist arthrodesis. In addition, our long-term functional outcome scores demonstrate significant disability after this injury, even when union is achieved. This information can help us better counsel our patients and set expectations after treatment of this injury.
Introduction
Displaced fractures of the scaphoid have a reported nonunion rate of up to 55%.1-3 These injuries can lead to a degenerative wrist condition termed scaphoid nonunion advanced collapse (SNAC). Left untreated, scaphoid nonunions have been shown to result in SNAC wrist in as little as 6.7 years.4,5 In an effort to prevent this late deformity, operative treatment of scaphoid nonunion is advocated. Most outcome measures after this surgery focus on achieving bony union of the nonunion, grip strength, and range of motion. Rates of bony union are extremely variable, ranging from 27% to 100%. 6 Reports on long-term functional outcomes of this injury are lacking. Few recent studies of modern fixation techniques report functional outcomes with a minimum of 5 or more years and a recent systematic review in the Journal of Hand Surgery specifically called for functional outcomes with follow-up of greater than 5 years.6-8 In addition, no study has published rate of return to active military service after this pathology and its surgical treatment. As the military requires physical activities involving weight-bearing in full extension at the wrist, this is a unique population in which to assess functional outcomes after this injury. The goal of our study was to define long-term functional outcomes of scaphoid nonunion repair in a military population to better counsel our patients and set expectations after treatment of this injury.
Materials and Methods
After obtaining approval from our institutional review board, we conducted a retrospective review of patients who underwent surgical repair for scaphoid nonunion at our institution from 2008 to 2017. Patients were identified by the Current Procedural Terminology code 25440 for scaphoid nonunion repair. All active duty, reservist, or recruit patients aged 18 years or older treated surgically for scaphoid nonunion repair were included. Exclusion criteria involved insufficient follow-up data and surgery performed within 3 months of injury as most sources agree that at least 6 months are needed to definitively identify a nonunion. 9 All operations were performed by fellowship-trained hand surgeons at a single institution. Surgical technique involved open reduction, internal fixation (ORIF) through either a dorsal or volar approach with single headless compression fixation. Surgeons used several different bone graft techniques including nonvascularized distal radius and iliac crest autograft, allograft, and 3 patients who received dorsal vascularized bone graft. All demographic data including age, sex, hand dominance, tobacco use, prior treatment, adjunctive treatment and surgical complications including need for revision surgery were collected via medical record review.
Our primary outcome measures were union rates, return to duty rates, and the Quick Disabilities of the Arm, Shoulder, and Hand (qDASH) functional outcome score. The qDASH is an 11-question outcome measure that has been validated as an effective alternative to the longer 30-question Disabilities of the Arm, Shoulder, and Hand (DASH) score in terms of cross-sectional and longitudinal reliability.10,11 When comparing scores in different studies, it is important to note that qDASH scores are approximately 4 points higher that DASH scores in the same patient.10,11 These scores were collected by telephone call. An unpaired t test was used to compare the mean final qDASH scores between patients who went on to union versus those who did not as well as the union rate between smokers and nonsmokers. Other questions asked during the telephone call included what percentage, in any, their wrist injury contributed to their deciding to leave military, if they have had another surgery on the wrist since leaving, and if they receive disability payments from the Department of Veterans Affairs (VA) due to their wrist injury. Other secondary outcomes included revision rate and limited duty (LIMDU) rate. A LIMDU period in the Navy and Marine Corps is a 6-month period of time in which a patient is temporarily removed from their regular occupation. This temporary removal from duty allows for recovery from their injury while avoiding physically demanding activities, deployments, or shipboard duty.
Results
A total of 144 patients met inclusion criteria. Only 2 patients were women and 142 were men. Average age at the time of initial presentation was 24.7 years. Average clinical follow-up was 9.4 months. Of 54 (37.5%) patients used tobacco, 89 (61.8%) used a bone stimulator after surgery, and 38 (26.4%) were given calcium and vitamin D supplementation (Table 1). Of the total 144 patients included, 40 had persistent nonunion after surgery for a rate of 27.8%. There were 3 superficial infections (2.1%) treated with oral antibiotics and no deep infections requiring revision surgery. Twenty-seven patients (18.8%) had revision surgery, the large majority of which were required for persistent nonunion. Other indications for revision included hardware prominence, stiffness, and post-traumatic osteoarthritis. These revision surgeries consisted of 10 scaphoidectomies with 4-corner fusion, 8 revision ORIFs, 3 proximal row carpectomies, 2 hardware removals, 1 wrist arthrodesis, 1 wrist arthroscopy and debridement, 1 radial styloidectomy with manipulation under anesthesia, and 1 distal scaphoid pole excision. While 74 patients (51%) needed at least 1 LIMDU period to recover after surgery, 74% of patients were able to return to full active duty. However, the number remaining on active duty continued to decrease at 1, 2, and 5 years after surgery as seen in Table 2. The nonunion rate in tobacco users trended higher than that in nontobacco users (35.2% vs 23%), but this was not statistically significant (P = .126). Use of bone stimulator and calcium and vitamin D supplementation also did not have a significant effect on the nonunion rate.
Demographics.

Note. Values are given as the number of patients with the percentage of patients in the cohort in parentheses, except for age, which is given as the mean with the total range in parentheses.
Outcomes After Operative Treatment of 144 Scaphoid Nonunions.

Note. LIMDU = limited duty.
Still on active duty 1, 2, or 5 years after the date of index nonunion surgery.
A total of 40 patients (28%) responded to the phone questionnaire at an average of 5.9 years after surgery (range: 1.3-11.5 years). Of all responders, the average qDASH score was 23.9 (range: 11-43). In those who went on to union after surgery, the average qDASH score of 21.9 was significantly lower compared with the score of those who had persistent nonunion, 29.2 (P = .0115) (Table 3). A total of 25% of patients indicated that their wrist symptoms were the primary reason they left the military; 75% of patients are receiving VA disability payments for their wrist. None of these patients had any additional surgeries since leaving the military.
qDASH Scores Among 40 Survey Responders.
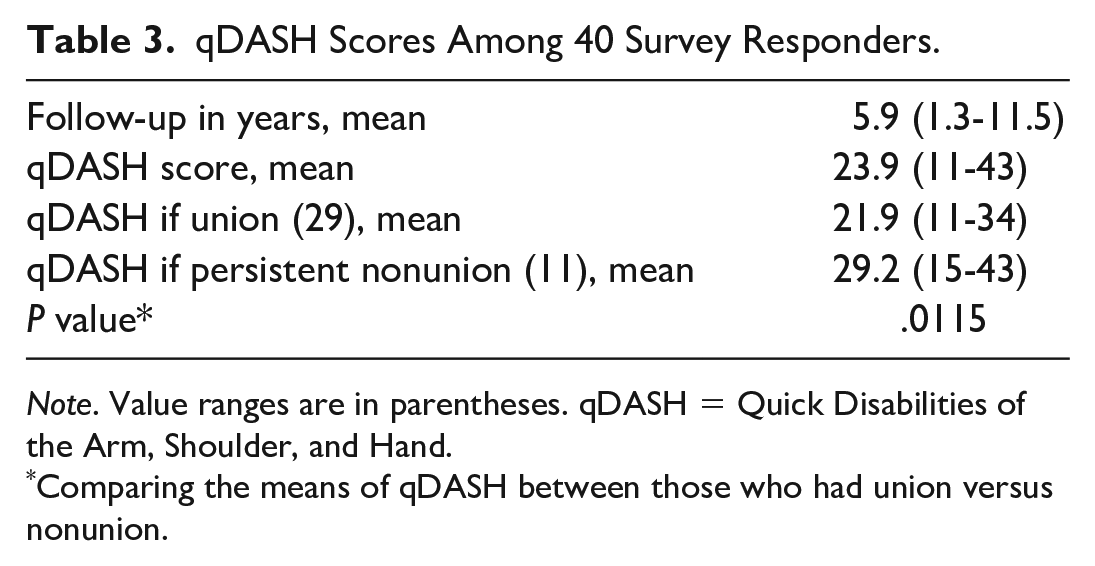
Note. Value ranges are in parentheses. qDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
Comparing the means of qDASH between those who had union versus nonunion.
Discussion
This is the first study to our knowledge to report return to duty rates and long-term functional outcomes after scaphoid nonunion repair in a military population. Historical literature has suggested that scaphoid nonunion is not compatible with active duty service and that surgical treatment results are unsatisfactory in this population. 12 Our study demonstrated that treatment is compatible with return to duty at a rate of 74%. Even so, our optimism is tempered by the reduced rate of patients remaining on active duty after 1, 2, and 5 subsequent years. Current literature using a variety of techniques for nonunion repair has found persistent nonunion rates from 6% to 34%.13-19 Our rates of nonunion (28%) and revision (19%) are at the upper end of the range seen in recently published studies. It is possible that different surgical techniques based on their findings at presentation would have led to better results. For example, only 3 of the 144 index surgeries involved vascularized bone graft, which the literature has found to increase union rates in the case of proximal pole avascular necrosis (AVN).13,17,18
Even if union is achieved, these injuries can lead to significant disability. The average qDASH score in this study was 23.9 at 6 years after surgery. There were 6 (15%) good, 31 (77.5%) satisfactory, and 3 (7.5%) poor outcomes in our cohort of responders 20 (Table 4). Other recent studies on surgical treatment of scaphoid nonunion have found DASH and qDASH scores ranging from 6 to 49.3 at final follow-up.14-16,19,21 As expected, qDASH scores were significantly higher in patients who went on to persistent nonunion. Disabilities of the Arm, Shoulder, and Hand scores in patients who fail to achieve union have been reported as high as 61.8, emphasizing the importance of selecting the surgical technique with the highest chance of achieving union. 14 To put things in perspective, our average qDASH score is comparable to those found in long-term follow-up for perilunate fracture dislocation injuries of 20 to 23.22,23 These values are significantly higher than those found in operative or nonoperative treatment of acute scaphoid fractures where the average DASH score is 4 at 10-year follow-up. 24 Baseline qDASH scores in the general population increase with age and average range of 7 to 10 in people aged 30 to 49 years. 25 Given that the minimal clinically important difference for qDASH scores is 14 to 15, the patients in our study had significant disability at long-term follow-up.11,26
Functional Outcomes Based on qDASH Scores in 40 Survey Responders.

Note. Excellent = qDASH 1 to 5; good = 6 to 15; satisfactory = 16 to 35; poor = >35. qDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
This study has several limitations. As this was a retrospective study with multiple surgeons, there was no standardization of surgical technique. Second, because radiographic review was outside the scope of this study, we were unable to quantify the severity of disease at the time of surgery. An early scaphoid nonunion without arthritic changes behaves differently from a chronic nonunion with AVN of the proximal pole and warrants a different treatment technique. This information was not always available in our chart review, and the selection of surgical technique may have affected the final outcomes. In addition, given the young age and high functional demands of this cohort, there was likely a bias toward fixation and motion preserving surgery even in the face of established risk factors for failure. Third, only 40 of the 144 patients responded to our phone calls to provide long-term functional outcome data. While this could be expected given that many of our patients have been out of the military for 5 to 10 years, this subjects our findings to selection bias.
The treatment of scaphoid nonunion remains a challenge to hand surgeons. Our study found that long-term functional outcomes were only satisfactory and associated with significant disability, even in the patients who achieved union. There remains a high rate of persistent nonunion, often requiring revision with a salvage procedure. While a high rate of patients were able to return to duty initially, far fewer were able to remain on active duty 5 years after their surgery. Based on our findings, military patients can be advised that they have good chance of returning to duty after this injury, but that they will have significant limitations compared with their uninjured side. This study highlights for military and civilian populations alike that expectation management is critical when treating this complex problem.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.