
Abstract
Background
Although pediatric hand fractures are common and generally have good outcomes, they remain a considerable source of anxiety for non–hand surgeons, who are less familiar with these injuries. We hypothesized that this anxiety may manifest as inefficiency in referral patterns.
Methods
The records of pediatric patients with isolated, closed hand fractures without concurrent trauma seen at our institution by a hand surgeon between January 2017 and December 2018 were retrospectively reviewed.
Results
There were 454 patients included; 62.1% were men, and the mean age was 9.6 years at initial encounter. Most patients (89.6%) were treated nonoperatively and incurred few complications (0.5%). Roughly half of all cases (n = 262) initially presented to an outside provider. Of these, 24.0% (n = 64 of 262) were evaluated by 2+ providers before a hand surgeon. Most commonly, these patients were referred from an outside emergency department (ED) to our ED before hand surgeon evaluation (n = 45 of 64). Forty-seven patients required surgery; however, none were performed urgently. Although a greater proportion of 7- to 11-year-old patients saw 2+ providers prior to a hand surgeon (P = .007), fewer required surgery (P < .001).
Conclusions
Pediatric closed hand fractures are mainly treated nonoperatively and nonemergently with generally excellent outcomes. Our data suggest that many patients continue to be referred through the ED or multiple EDs/providers for treatment. These inefficient referral patterns demonstrate the need for better education for ED and primary care providers, as well as better communication between these providers and local pediatric hand surgeons. Advancements in these areas are likely to improve efficiency of care and decrease costs.
Keywords
Introduction
Hand fractures are common injuries in the pediatric population, frequently managed both in primary care and in acute settings. It has been reported that hand fractures comprise about 2.3% of all pediatric emergency department (ED) visits, and almost one-third of pediatric hand fractures are referred by primary care physicians (PCPs) to tertiary care facilities.1-5 As such, both ED physicians and PCPs play a pivotal role in the referral and management of these injuries. 6
Guidelines for the management of emergent pediatric hand trauma (ie, open fractures, fingertip injuries/amputations) exist7-9; however, these injuries constitute a small minority of all hand fractures. It has been reported that open fractures only represent 4% of all hand fractures evaluated by physicians, whereas closed phalangeal fractures are one of the most common types of fractures seen by PCPs.10,11
In an age of cost containment and patient-centric care, the management and referral pattern of these nonemergent pediatric hand fractures have become a topic of interest for hand surgeons, PCPs, and ED physicians alike. Although previous studies have shown that surgical intervention is rarely required and outcomes are generally good for closed hand fractures,10,12 emerging studies have drawn attention to the current inefficiency that exists in the referral and treatment of all types of hand injuries.11,13,14 This inefficiency is likely due in part to a paucity of data that address presentation patterns for closed hand fractures in children. To address these knowledge gaps, this study characterizes the presentation patterns, treatment, and outcomes of pediatric closed hand fractures at a single, urban, tertiary pediatric care center.
Materials and Methods
Approval was obtained from our institution’s committee on clinical investigation with a waiver of informed consent. Hospital records were queried using International Statistical Classification of Diseases and Related Health Problems, 10th revision codes associated with closed hand fractures. The medical records of patients with closed phalangeal or metacarpal fractures treated at our institution from 2017 through 2018 were identified and reviewed. Inclusion criteria for analysis required patients to be evaluated by a hand surgeon at our institution. Patients with open fractures, concurrent major trauma, incomplete medical records, or those above the age of 18 years were excluded. Medical records were reviewed for demographic information, referral history, injury type, intervention, and outcomes. For analyses, an operation was defined as a closed reduction with percutaneous pinning or an open reduction with internal fixation and did not include closed reductions with local anesthesia. In addition, an “urgent operation” was defined as one where surgery was performed within 24 hours after the initial hand injury.
For the purpose of this study, referral patterns were defined as either direct or indirect. A direct referral pattern was defined as the referral of a patient who had been seen by only 1 provider before subsequent evaluation by a hand surgeon at our institution. An indirect referral pattern was defined as the referral of a patient who was seen by at least 2 providers before evaluation by a hand surgeon at our institution. Indirect referral patterns manifested as patients either being evaluated by an outside ED, transferred to our ED, and subsequently referred to a hand surgeon or being evaluated by their PCP who sent them to our ED, after which they were referred to a hand surgeon (Figure 1a and 1b).
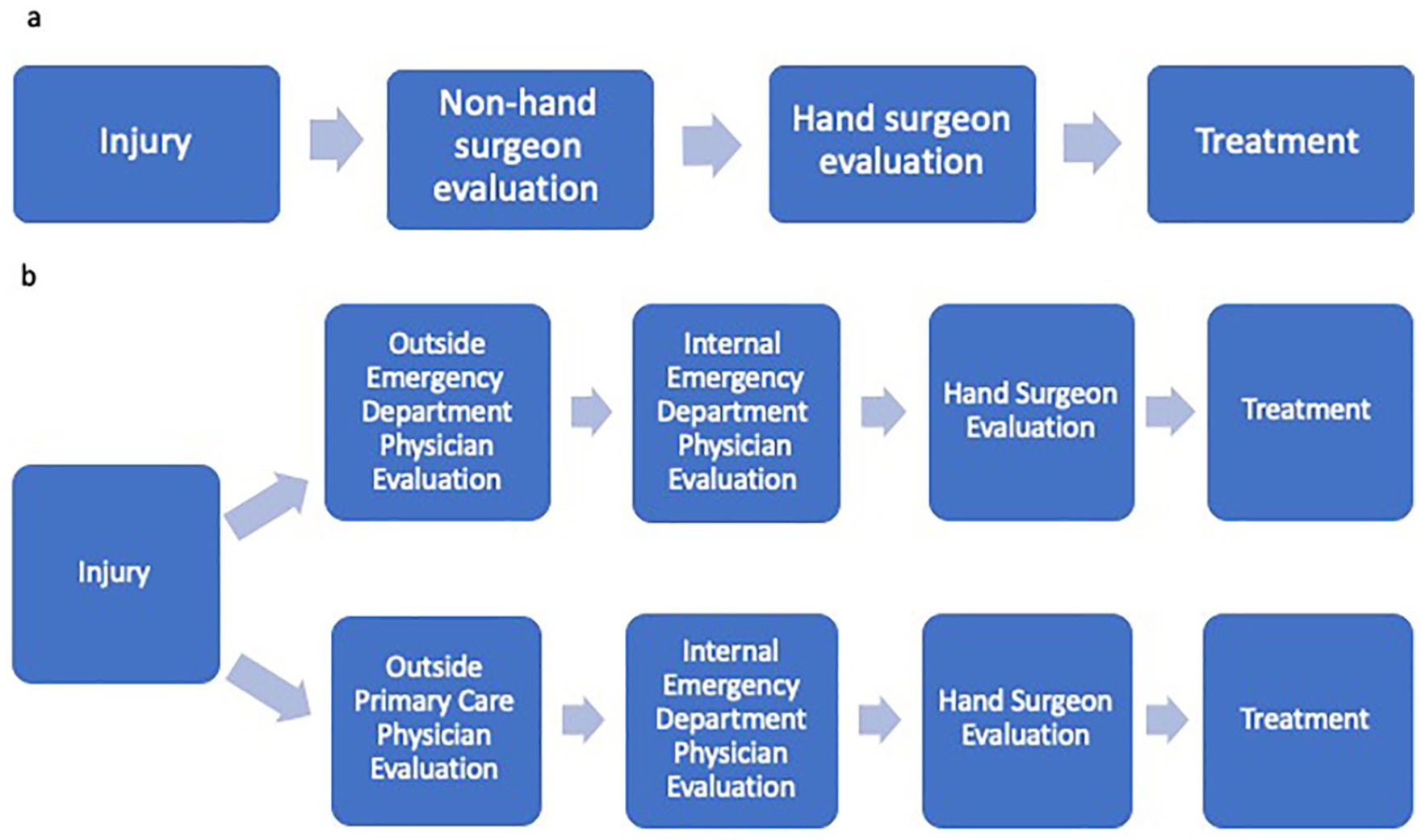
Referral patterns for pediatric closed hand fractures: (a) flow chart depicting direct referral pattern and (b) flow chart depicting indirect referral pattern.
Statistical analyses were conducted using SPSS (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, New York: IBM Corp.). Frequency distributions for demographic and clinical variables were tabulated, and mean and median values were calculated as appropriate. Patients were divided into 3 age groups: preschool (0-6 years old), elementary school (7-11 years old), and adolescence (12-18 years old). Referral pathways and interventions were compared by age group via Pearson χ2. The normality of the median time from injury to surgery of the indirect and direct referral groups was assessed by Shapiro-Wilk test and was found to be a non-normal distribution. Comparison between these 2 groups was thus conducted by Mann-Whitney U test. A value of P < .05 was considered significant for analyses.
Results
Demographics
A total of 499 patients were identified. However, 45 patients were excluded because they did not meet the inclusion criteria (ie, patient having other concurrent trauma or not being evaluated by a hand surgeon). Most of these patients were male (62.1%, n = 282) with a mean age of 9.6 ± 3.9 years.
Referral Patterns
A little more than half of the patients (57.7%, n = 262) initially presented to an outside provider or institution. All other patients (42.3%, n = 192) initially presented to our institution through the ED or the urgent care hand clinic. Among those who were referred to our institution by outside providers, there were 2 general referral patterns: a direct pattern (76.0%, n = 199), where patients saw 1 provider before being evaluated by a hand surgeon, and an indirect pattern (24.0%, n = 63), where patients saw 2+ providers before being evaluated by a hand surgeon. When patients were indirectly referred, either they were evaluated by an outside ED, transferred to our ED, and subsequently referred to a hand surgeon (71.4%, n = 45 of 63) or they were sent by their PCP to our ED and then to a hand surgeon (28.6%, n = 18 of 63).
Treatment and Outcomes
Most patients (89.6%, n = 407 of 454) were managed nonoperatively (Table 1). Two (0.5%) patients healed with malunions requiring surgical correction 43 and 166 days following the initial hand injury, respectively. A common nonoperative intervention performed on patients who were treated at our ED or urgent clinic was a reduction prior to hand fracture casting or splinting (21.7%, n = 49 of 226). Hand surgeons, fellows, or residents were consulted by the ED to perform 96% (n = 47 of 49) of these reductions. A significantly greater proportion of patients who were referred from outside providers to our ED required a reduction compared with those who presented directly to our ED or urgent clinic (48.0% vs 12.9%; P < .001). The remaining 10.4% (n = 47) of our series were treated surgically for either an unstable or nonreducible fracture (n = 33, 70.2%) or intra-articular involvement (n = 14, 29.8%). There was no significant difference between the rate of surgery performed within the indirect and direct referral groups (17.5% vs 13.6%; P = .42). The most frequently injured digit requiring surgery was the small finger (n = 23, 42.5%). The median length of time from hand injury to surgery was 8 days (interquartile range [IQR], 6 days). The median time from hand injury to surgery was significantly longer in the indirect referral group compared with the direct referral group (11.0 vs 7.0 days, P = .047). No case in our series required urgent surgery.
Types of Intervention by Hand Specialists.
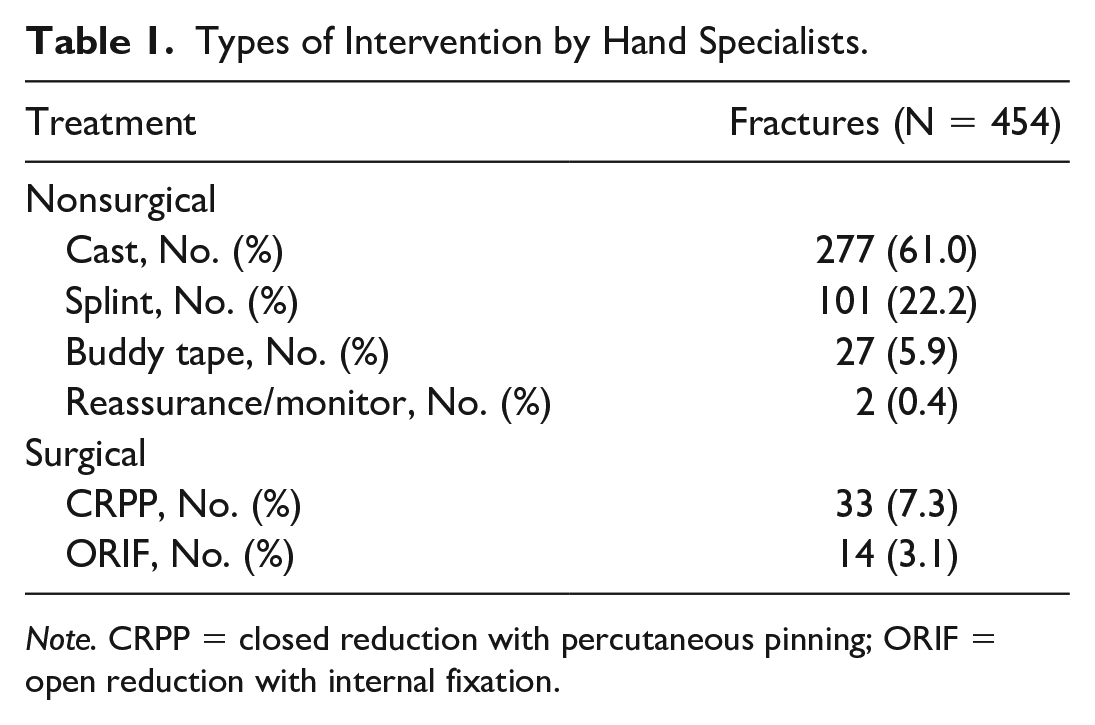
Note. CRPP = closed reduction with percutaneous pinning; ORIF = open reduction with internal fixation.
Two (4.3%) surgical cases experienced a postoperative complication, including a delayed union treated with prolonged immobilization (n = 1) and pin site irritation requiring pin adjustment (n = 1). Surgical patients were followed postoperatively for a median (IQR) of 57 (34) days.
Age Group Subanalysis
The proportion of patients referred to our institution did not vary by age group (P = .66; Table 2). Elementary school–aged children (33.3%) were referred via an indirect referral pattern significantly more often than their preschool-aged and adolescent counterparts (17.5% and 15.8%, respectively; P = .007). However, a greater proportion of the adolescent cohort required surgical intervention than younger patients (19.7% adolescent vs 5.7% elementary school vs 9.4% preschool; P < .001).
Age Group Analysis of Referral Patterns.

*A value of P < .05 was considered significant for analyses.
Discussion
Closed phalangeal and metacarpal fractures in children are common, comprising 2.3% of all ED visits. 3 In addition, these injuries may also be seen and treated by PCPs in the office setting. Although the mechanisms of injury vary throughout childhood, operative intervention is the exception, and outcomes are generally good. Despite their prevalence and benign clinical course, anxiety over misdiagnosis and mistreatment still persists. Gornitzky et al 14 suggested that ED physicians may be uncomfortable treating pediatric hand fractures due to concerns for misdiagnosis, especially for children under the age of 9 years. We hypothesized that this anxiety would manifest as excessive or circuitous referral patterns from outside providers to our institution. Therefore, we aimed to characterize the presentation patterns, treatment, and outcomes of pediatric closed hand fractures at a tertiary pediatric care center.
This case series examined the presentation and management of 454 patients who received care from pediatric hand surgeons at a tertiary care hospital. Both the sex and age distribution of this cohort approximated what has been previously reported for hand fractures.10,12,15 Our study found that nearly all injuries (89.6%) were treated with nonsurgical interventions, such as casting and splinting, which is consistent with previously reported rates of nonsurgical management for hand fractures.12,14 This nonoperative strategy resulted in excellent outcomes as only 2 (0.4%) patients in our series incurred a complication. This is similar to reports in the pediatric population.16,17
A minority (10.4%) of our cohort required surgical management for their fracture, a frequency similar to other studies. 10 As expected, there were 2 main indications for surgical intervention: fractures with loss of articular congruity or fractures that were unreducible/unstable. 18 Surgical intervention also resulted in excellent outcomes, with only 2 (4.3%) of all surgically treated patients incurring a complication, a rate which is lower than previously reported. 10 In addition, none of these surgical cases required urgent intervention, with most procedures occurring 5 to 11 days following initial injury. This observation is important for referring providers to be aware of as it suggests that emergent referral for closed hand fractures with no concurrent trauma is rarely, if ever, necessary.
Over half of all hand fractures treated at our institution were referred by an outside provider, which is a considerably greater rate than that reported in similar studies. 5 Of these referred patients, about one-quarter were indirectly referred and evaluated by 2+ non–hand providers. This finding suggests that inefficiencies in the form of extra office or ED visits still exist for these common injuries. Although it is unclear how many patients were completely managed by their outside institution and did not require referral, hundreds are referred to our institution annually. In addition, in many of these indirectly referred cases, surrounding community EDs were evaluated, and then the patient was referred to our ED where a secondary evaluation was performed before referral to hand surgeons. When a community ED admits and evaluates a child with a closed hand fracture, ideally these injuries would undergo stabilization with a direct, nonemergent referral to a hand surgeon who treats children. Although individual pediatricians’ offices may not be equipped to manage these injuries initially and may require further management in an ED, these providers should be familiar with surrounding institutions or providers who will manage these injuries efficiently.
Furthermore, it was observed that the elementary school–aged patients in our series were more likely to see multiple non–hand surgeons before definitive treatment. However, this subgroup was significantly less likely to require surgery compared with the adolescent group, who were more often directly referred to a hand surgeon for care. This finding may speak to the uncertainty that non–hand surgeon providers face when evaluating and treating younger patients with closed hand fractures. Previous studies have hypothesized reasons for excessive referrals for these relatively minor injuries, citing causes such as physicians’ caseload volume, anxiety regarding litigation for misdiagnosis, and the lack of access to pediatric specialists.3,14,19 In addition, a recent systematic review examining all types of pediatric hand injuries posited that inefficiency may result from a more basic disconnect between the referring criteria used by PCPs and hand surgeons. 18 The explanation is likely multifactorial and will vary based on the referring providers’ resources, experience, and geographic location. In addition, we found that when children were referred to our institution’s ED, they required reduction at a much higher rate than patients who initially presented to our institution. This difference in the overall need for reductions is unlikely to be attributable to differences in overall frequency of fractures requiring reduction between community hospitals and our institution. Rather, it suggests that community hospital providers frequently refer to our ED for reduction of these fractures. Greater education and training is needed concerning how to safely and effectively reduce closed hand fractures in children.
We conclude that opportunities exist to improve patient care for children with closed hand fractures. Ideally, these changes would involve both the community non–hand surgeon providers who often see these patients first and the hand surgeons who often treat them definitively. One area for improvement is increased recognition by the former group that the overwhelming majority of closed, pediatric hand fractures are treated nonoperatively and have good outcomes. Moreover, these injuries rarely require emergent or even urgent surgical care, obviating the need for ED-to-ED transfers. However, education and communication should be facilitated by the pediatric hand surgeons and centers who definitively treat these patients. Specifically, educational tools to address common fracture patterns and likelihood of surgery, techniques in splint application, and, in some cases, fracture reduction should be made available. Furthermore, hand surgeons or pediatric centers should implement user-friendly, fast-track pathways of care to enable referring providers to easily bypass the tertiary care ED when establishing definitive care for patients. Previous studies from Lee et al and Colen et al have shown that hand injuries contribute significantly to ED volume and cost burden, citing ED charges of $21 billion over a 4-year period.20,21 Thus, new referral pathways, which circumvent multiple ED visits, potentially could yield considerable savings.
Study limitations must be acknowledged. This data set only represents the referral pattern of patients presenting to a single tertiary care facility that specializes in pediatric care and thus may limit its generalizability. In addition, this medical center fields referrals from a large surrounding metropolitan and suburban population with varying capabilities, which may also impact the results of this study. Furthermore, due to the retrospective nature and limited access for referral criteria from outside providers, the reported results may fail to capture the nuances involved in the multifaceted decision to refer a patient. For example, our findings may actually underestimate the current state of referrals if patients were seen at multiple local practices or urgent care centers before being referred to our institution. Conversely, our findings cannot fully appreciate all current practice patterns as we recognize many patients are managed by an outside PCP or ED provider and did not require evaluation at our institution. Future studies should explore the initial management by outside providers, such as attempted reductions or other interventions, and reasons for referrals.
Conclusion
Pediatric closed hand fractures are mainly treated nonoperatively and nonemergently with generally excellent outcomes. Our data suggest that many patients continue to be referred through the ED or multiple EDs/providers for treatment. These inefficient referral patterns demonstrate the need for better education for ED and PCPs, as well as better communication between these providers and local pediatric hand surgeons. Advancements in these areas are likely to improve efficiency of care and decrease costs.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article contains studies with human subjects.
Statement of Informed Consent
Our institutional review board approved this study with a waiver of informed consent (protocol number: P00032379).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.