
Abstract
Background
A paucity of literature exists specifically examining self-inflicted (SI) gunshot wounds (GSWs) to the hand and wrist, which impart greater energy and have a higher risk of adverse events than non–self-inflicted (NSI) GSWs.
Methods
We retrospectively reviewed records of patients who presented to our plastic surgery service after sustaining acute GSWs involving the hand and wrist between 2016 and 2018.
Results
We identified 60 patients who sustained GSWs involving the hand and wrist; 17 (28%) were SI, and 43 (72%) were NSI. Within the SI group, 100% of patients were Caucasian, with an average age of 54 years. Within the NSI cohort, 77% of patients were Black, 19% were Caucasian, and 4% identified as other. While not statistically significant, we noted a substantial increase in patients requiring operative intervention in the SI cohort (65% SI vs 37% NSI, P = .08). There was a statistically significant increase in patients requiring more than 1 operation in SI patients (24% SI vs 5% NSI, P = .04). Patients who sustained SI injuries were also more likely to present with acute carpal tunnel syndrome requiring urgent surgical release and to develop wound infections (12% vs 0%, P = .08).
Conclusions
Self-inflicted GSWs involving the hand and wrist are associated with greater morbidity than their low-energy NSI counterparts. Individuals presenting with SI GSWs are more likely to be older, to require multiple operations, to develop infections, and to present with acute carpal tunnel syndrome requiring urgent surgical decompression.
Keywords
Introduction
In the United States, firearms account for more than 67 000 nonfatal injuries and 31 000 deaths annually.1,2 The 2018 Small Arms Survey report showed that more than 85% of the 1 billion small arms distributed globally belonged to civilians. The United States, which accounts for less than 5% of the world’s population, owns 46% of the global total of civilian-own guns.3,4 Upper extremity trauma resulting from firearm injury is common. Roughly 17% of all nonfatal injuries and more than 70% of unintentional gunshot wounds (GSWs) involve the upper extremity. 2 These injuries have increased in incidence with a rise in domestic violence combined with growing availability of handguns to the civilian population. 5 The fallout associated with firearm injuries presents a major public health challenge with permanent and widespread consequences.1,2,6 Beyond the devastating impact of premature death and disability, firearm injuries also have profound economic implications for our health care system and society as a whole, amounting to a staggering $48 billion annually in combined medical bills and lost work. 1
There is ample literature on the impact of GSWs to the upper extremity. However, there is a paucity of information specifically examining the injury patterns and overall morbidity associated with self-inflicted (SI) GSWs to the hand and wrist. Ballistic injuries to the hand and wrist are often associated with elevated morbidity due to the high density of vital structures and overall complexity of hand and wrist mechanics. These injuries, when SI, are invariably accidental in nature and associated with low-velocity (<600 feet/second) handguns. The classic presentation involves a middle-aged Caucasian man with a single GSW to the hand or wrist following accidental discharge while cleaning a firearm (Figure 1). Due to the point-blank nature of SI GSWs, greater energy is imparted on the soft tissue and bone compared with non–self-inflicted (NSI) GSWs. Existing literature on GSWs to the upper extremity has failed to consistently differentiate between SI and NSI injuries. Given the financial burden and morbidity associated with these SI GSWs, it is imperative that we work to better understand this patient population and their often devastating injuries. The purpose of this study is to examine the injury patterns, management, and sequelae of SI GSWs to the hand and wrist and to highlight differences relative to traditionally studied NSI GSWs. The evidence presented here may serve as a guide for management and counseling of patients affected by these devastating injuries.

Clinical photos of a patient who sustained a self-inflicted gunshot wound while cleaning a loaded, 9-mm handgun.
Materials and Methods
An institutional review board–approved retrospective review was performed, examining records of patients who presented to our plastic surgery service after sustaining acute GSWs involving the upper extremity between 2016 and 2018. Patients were identified using International Statistical Classification of Disease, 10th Revision codes. Charts were then reviewed to identify whether the GSW was or was not SI, creating 2 groups for comparison. Patients with a mechanism of injury secondary to shotgun, pellet, or BB gun injury were excluded. In our preliminary review, we determined that shotgun injuries to the hand and forearm were almost exclusively NSI in nature. Due to the greater energy, blast radius, and degree of bone and soft tissue destruction associated with shotgun injuries, we decided to exclude this potentially confounding mechanism of injury. Patients younger than 18 years of age or having undergone a prior hand or wrist surgery were also excluded. Clinical charts including admission notes, consult notes, and operative reports were reviewed to identify patient demographics (age, sex, race, zip code) and relevant clinical information. Patient injuries were assessed, noting location of injury, presence of fracture, soft tissue loss, need for operation, and time to operation. Clinical notes from follow-up visits were analyzed to review outcomes, including persistent neuropraxia, presence of infection, general functional status, and need for reoperation. Demographic and clinical factors were compared using bivariate analyses. Continuous variables were compared using a Mann-Whitney U test. Categorical variables were compared using the Fisher exact test and Pearson χ2 test. Statistical significance was defined as P < .05.
Results
We identified 60 patients who sustained GSWs involving the hand and wrist presenting to our level 1 trauma center plastic surgery service between 2016 and 2018. Of these 60 patients, 17 patients (28%) sustained SI GSWs, and 43 (72%) sustained NSI GSWs. All SI wounds were reported to be accidental; 11 (65%) were reported to occur while cleaning the weapon. Ballistic data were available for 14 SI patients (82%), with 9 mm handguns being implicated in half of these cases. Ballistic data were not readily available for the NSI cohort. All patients in the SI cohort were Caucasian men, with an average age of 54 years. In the NSI group, 41 patients (95%) were men, with an average age of 29 years; 33 patients (77%) were Black, 8 (19%) were Caucasian, and 2 (4%) identified as other. Within the SI group, 4 patients (24%) had a medical history significant for diabetes mellitus. Ten (59%) of 17 SI patients presented with bony injuries, with 80% (8 of 10) of these injuries affecting the proximal phalanx. Within the SI group, 11 patients (65%) required operative intervention, with 4 of those 11 patients requiring more than 1 operation. Criteria for operative intervention included neurovascular compromise; extensive soft tissue or skin loss; critical injury to flexor or extensor tendons; fractures with significant angulation, rotational deformity, or functional impairment; and fractures with severe contamination, comminution, or segmental bone loss. Two patients (12%) in the SI cohort presented with acute carpal tunnel syndrome requiring urgent surgical release. Of the 11 SI patients who underwent operative intervention, 2 (18%) of these patients developed wound infections. In the NSI cohort, 16 (37%) of 43 required operative intervention, with no cases of acute carpal tunnel syndrome and no cases of postoperative infection. These results are summarized in Tables 1 and 2. In-person, outpatient follow-up was recommended for all patients in both groups. Incarceration did not preclude follow-up, as these patients are routinely transported by the justice center to our outpatient office, accompanied by a guard. We did not identify a statistically significant difference, between groups, in the number of patients lost to follow-up (LTF) after their initial emergency department (ED) visit. In the NSI group, 12 (28%) of 43 patients were LTF after the initial ED visit, compared with 1 patient (6%) in the SI group (P = .09). The mean duration of follow-up in the SI group was 119 days; excluding the patient LTF after the initial ED visit increased the duration of follow-up to 127 days. In comparison, the mean follow-up duration for the NSI group was 80 days; excluding patients who were LTF after their initial ED visit increased the duration of follow-up to 110 days. While it is possible that a patient would decide to follow-up elsewhere, we identified only 1 patient who received additional hand care at another institution. We found no statistically significant differences in insurance coverage between groups, with 76% (13 of 17) of patients insured in the SI group and 77% (33 of 43) of patients insured in the NSI group.
Demographic Information.
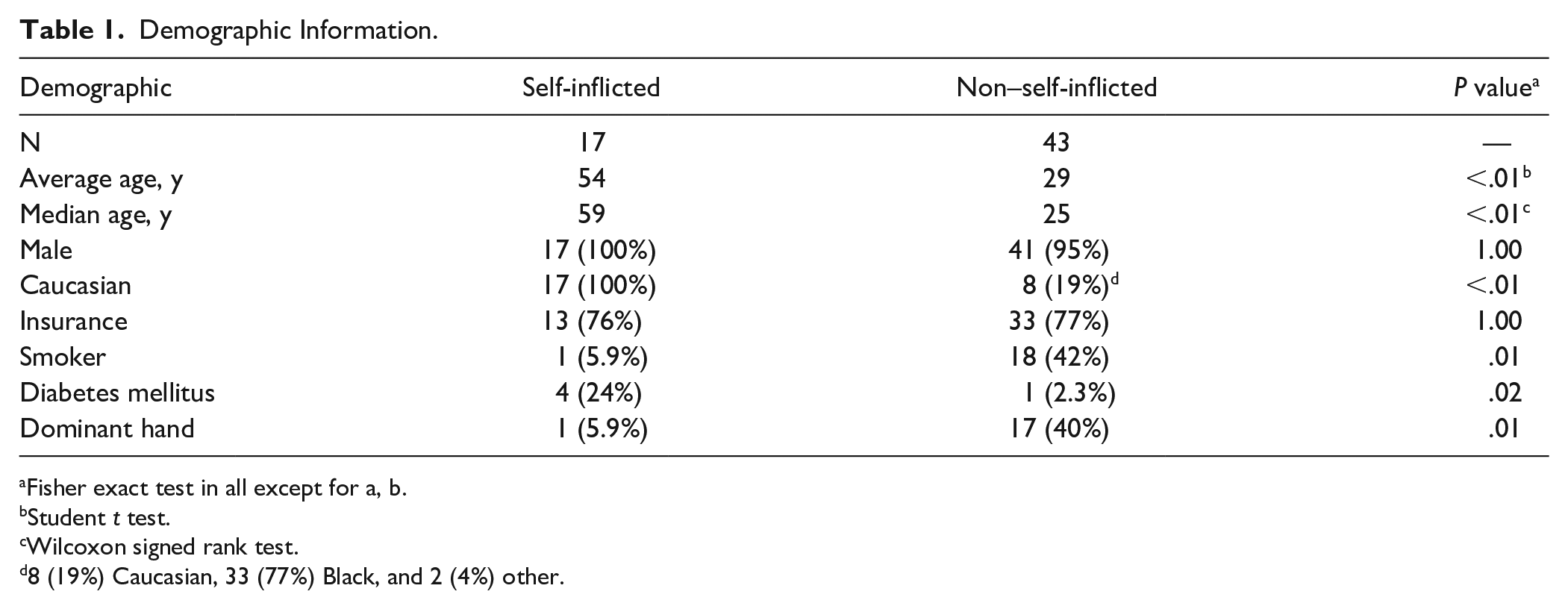
Fisher exact test in all except for a, b.
Student t test.
Wilcoxon signed rank test.
8 (19%) Caucasian, 33 (77%) Black, and 2 (4%) other.
Injury and Management Patterns and Sequelae.
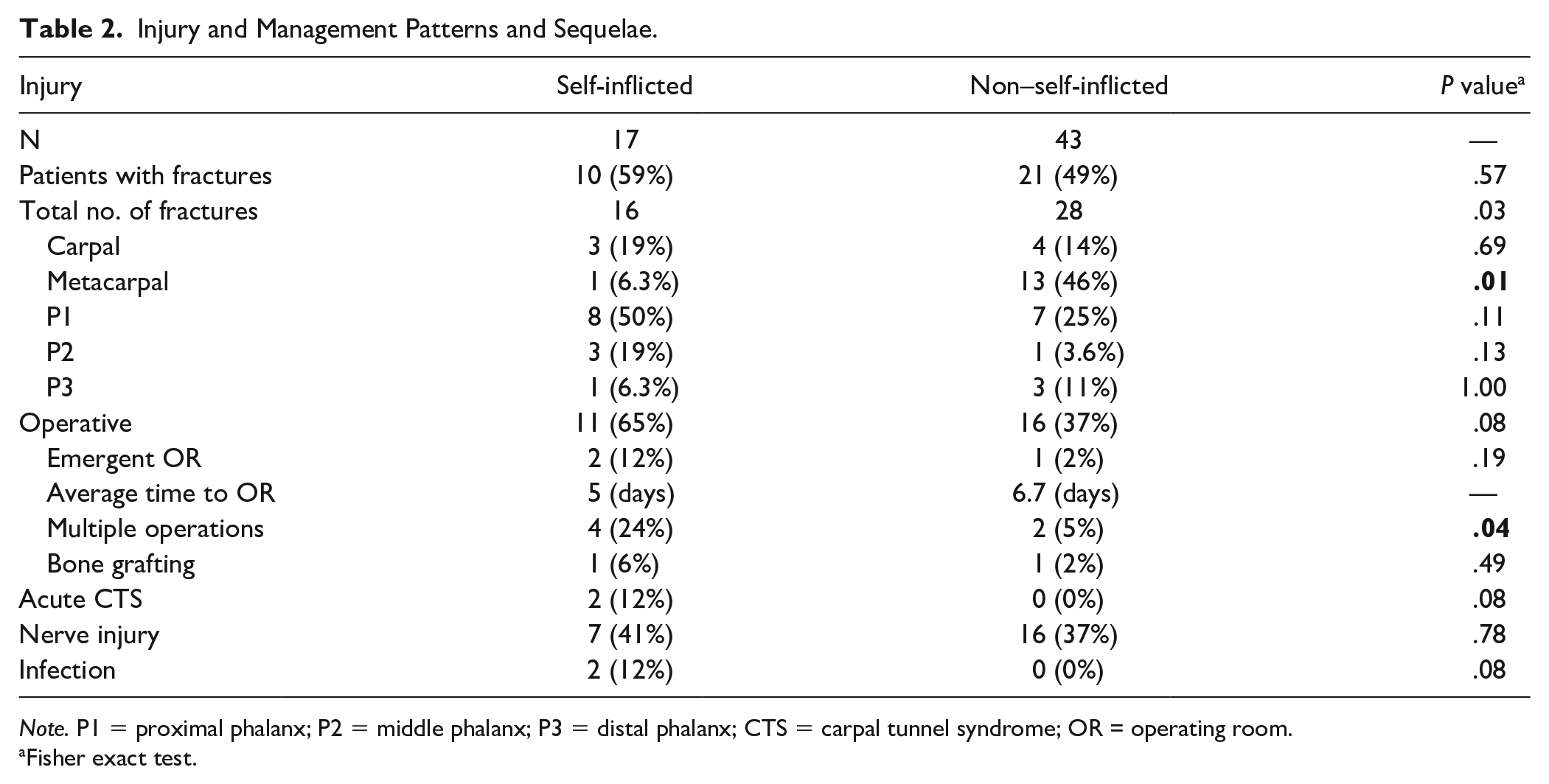
Note. P1 = proximal phalanx; P2 = middle phalanx; P3 = distal phalanx; CTS = carpal tunnel syndrome; OR = operating room.
Fisher exact test.
Discussion
The aim of this study was to better understand the injury patterns, management, and sequelae of SI GSWs affecting the hand and wrist and to outline differences relative to traditional NSI GSWs. Hand surgeons are no strangers to firearm injuries, as approximately 17% of all GSWs involve the upper extremity. 1 In cases of SI injuries, that number doubles, with 34% of unintentional GSWs affecting the upper extremity. National firearm surveillance data have indicated that young men in their second and third decades of life consistently account for over half of all nonfatal GSW injuries. 6 One of the striking findings of our review is the age and race disparity between our SI and NSI cohorts (Figure 2). Consistent with national trends, we found that of the 43 patients in our NSI group, a disproportionate percentage of patients were young Black men (77%), with an average age of 29 years. This is a stark contrast to the demographics of the 17 patients in our SI cohort, in which all were Caucasian men, with an average age of 54 years (Table 1).
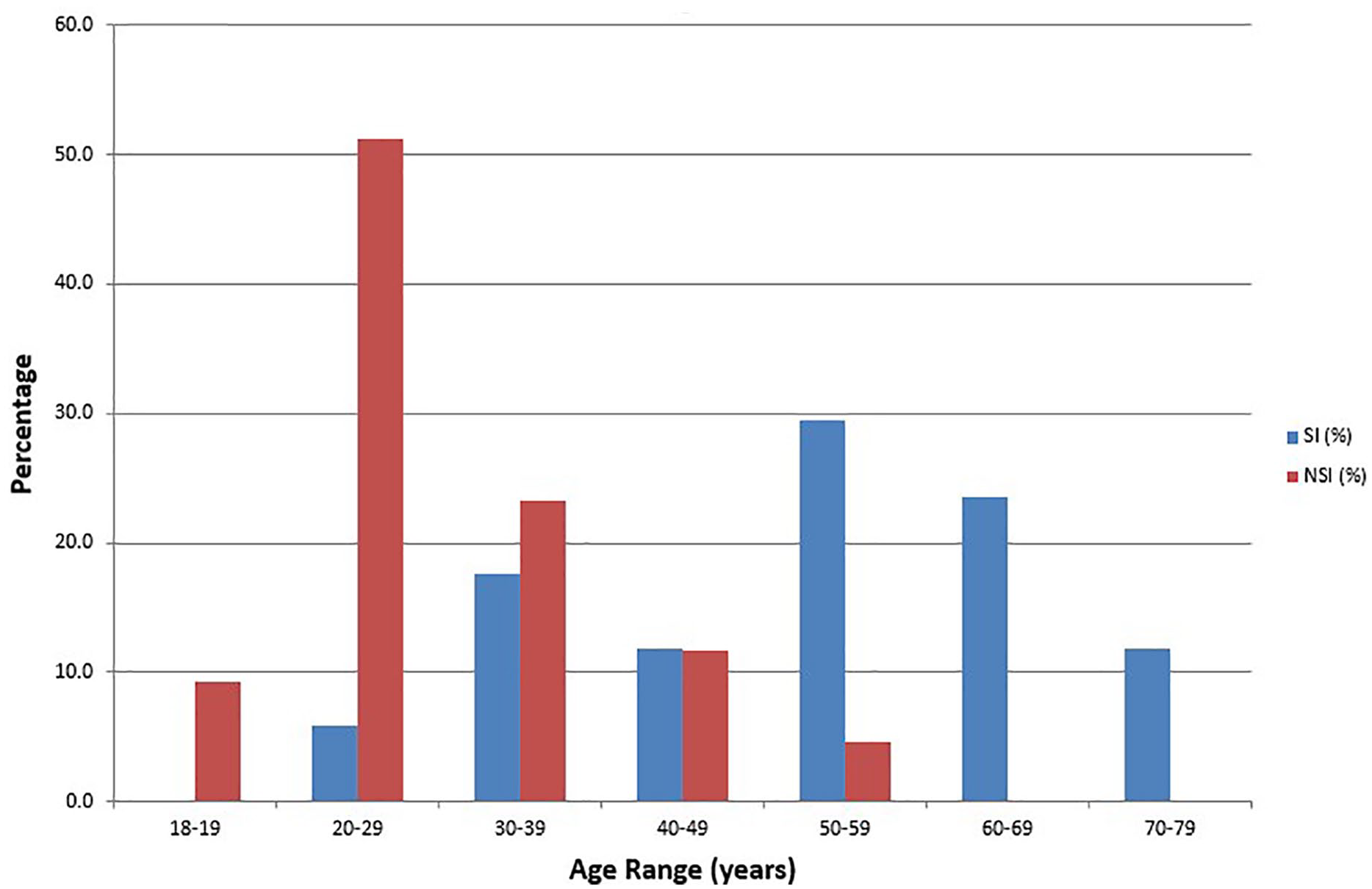
Age distribution of patients with gunshot wounds to the hand and wrist.
In our literature review, we identified just 1 other publication that explicitly identified SI GSWs. Hutchinson et al reviewed 97 firearm-related hand injuries that presented to a level 1 trauma center over a 10-year span. In contrast to our study, in which just 28.3% of injuries were SI, Hutchinson and colleagues found that most (81.4%) of the patients in their series sustained SI injuries. The reason for this discrepancy is not immediately clear, although the series by Hutchinson et al 7 did include 44 BB and pellet gun injuries, which may have a higher likelihood of occurring secondary to an SI mechanism. The frequency of bony injury in our review (59% SI vs 49% NSI) was similar in our 2 groups and consistent with the existing literature. However, we noted a substantial increase in patients requiring operative intervention in the SI cohort (65% SI vs 37% NSI). Pereira and Boyd 8 reported that comminuted fractures involving the phalanges and metacarpals are common—up to 61% of cases—whereas defects requiring bone grafting are less common. Our review echoes these findings, especially in the NSI cohort, where 48% of patients with bony injuries sustained fracture(s) to the metacarpals and 33% involving the phalanges. In contrast, most SI patients with bony injuries fractured the proximal phalanx (Figure 3a). Proximal phalanx fractures affected 80% of patients and accounted for 50% of all fractures in the SI cohort (Table 2). Existing literature has demonstrated that bone grafting in the setting of GSW injuries is well tolerated, with a low complication rate.9-11 Despite being associated with greater energy, our SI sample was too small to draw definitive conclusions regarding any increased likelihood of injuries requiring bone grafting. In our review, only 1 patient in each group required bone grafting.
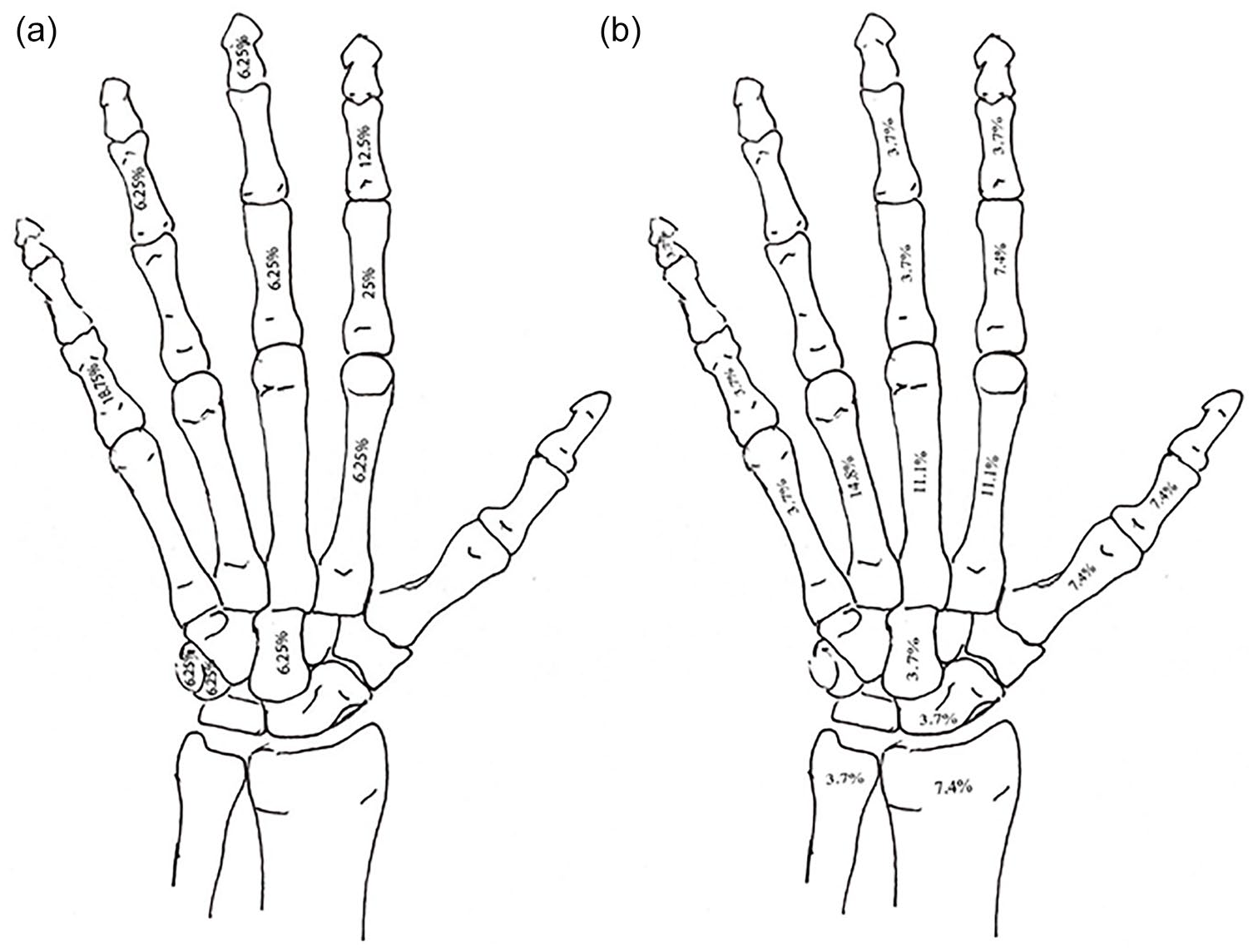
(a) Distribution of fractures in the self-inflicted gunshot wound cohort. (b) Distribution of fractures in the non–self-inflicted gunshot wound cohort.
Although existing literature describes wide variation in the incidence of postinjury neuropraxia and nerve injury, our study revealed that SI GSWs had an increased risk—albeit not statistically significant—of developing acute carpal tunnel syndrome requiring urgent surgical decompression. Kouyoumdjian reported nerve injury rates as high as 21%, Elstrom et al reported 45%, and Pannell et al recently reported an incidence of 63%.12-14 Pannell et al retrospectively reviewed 41 patients in an effort to identify predictors of nerve injury after GSWs to the upper extremity. In patients with nerve injury, Pannell et al 12 found a higher incidence of fractures, retained fragments, vascular injury, and compartment syndrome. In their series, despite a 63% rate of nerve palsy, no patients were reported to have acute carpel tunnel syndrome. In our review, 35% of SI GSW patients and 37% of NSI patients suffered from some degree of neuropraxia at a mean follow-up of 16 weeks.
Classic treatment algorithms advocate early aggressive surgical debridement, bony fixation, and repair of damaged structures as indicated.11,12,15-17 Of our 11 SI patients who required operative intervention, 6 patients underwent fracture fixation by means of closed reduction and percutaneous pin, open reduction and internal fixation, or external fixation; 3 patients underwent revision amputations; 2 patients required skin grafting; 2 patients required urgent carpal tunnel release; and 1 patient required ulnar artery repair. All patients in our SI and NSI cohorts underwent timely bedside washout with administration of antibiotics in the ED. Patients with fractures were continued on a week-long course of oral antibiotics, per standard protocol at our institution. With the exception of injuries with neurovascular compromise mandating urgent operative intervention, surgical treatment was performed at an average of 5 to 7 days following injury. While most of the operative NSI patients required only a single procedure for definitive treatment, we found that SI GSWs were associated with a statistically significant increased risk of requiring multiple operations. Four (36%) of 11 operative patients in the SI cohort required additional trips to the OR. Two of these patients underwent multiple washouts due to persistent devitalized tissue (with 1 patient requiring skin grafting); 1 patient underwent bone grafting; and 1 patient underwent secondary tenolysis and capsulotomies. While not statistically significant, we found it notable that our SI cohort had a 12% rate of infection, which tends to be a rare sequelae of traditional low-velocity GSWs to the hand.8,11,18 Although patients in our SI cohort had a statistically significant increased rate of diabetes, neither patient who developed infections had a history of smoking or diabetes. Existing literature has demonstrated that while civilian GSW infection rates are typically low, higher velocity weapons and weapons with increased blast effect (ie, shotguns) are associated with higher rates of infection.18-20 In a similar fashion, our review indicates that SI GSWs increase energy delivered substantially enough to increase the burden of devitalized tissue, as well as the complexity of definitive treatment.
Better understanding of and appreciation for the elevated morbidity associated with SI GSWs allow the practitioner to have a more informed preoperative conversation with the patient and to better guide management decisions. There are limitations associated with this study. First, we had a relatively small sample size, which is compounded by limited long-term follow-up. Despite an average follow-up of 16 weeks in our SI cohort, 35% of patients were LTF within 4 weeks. Consequently, we were unable to perform consistent review of postinjury functional outcomes. Retrospectively collected data are also inherently subject to its own limitations and may be incomplete or inaccurate. In future studies, it would be beneficial to gather consistent, long-term follow-up data to formally assess functional outcomes between the 2 groups. Despite its limitations, our review provides evidence that SI GSWs to the hand and wrist are associated with greater morbidity than their low-energy NSI counterparts. Individuals presenting with SI GSWs are more likely to be older, to require multiple operations, to develop postoperative infections, and to present with acute carpal tunnel syndrome requiring urgent surgical decompression. Further studies with larger cohorts and better analysis of functional outcomes are needed to fully determine the long-term impact of these injuries.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
Institutional review board approval was obtained prior to performing this retrospective review. All patient identifiers were removed in the data collection process and are not included in this manuscript.
Statement of Informed Consent
Informed consent was waived due to the retrospective nature of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.