
Abstract
Systemic sclerosis (scleroderma, SSc) is an autoimmune disease that causes significant dysfunction to multiple organ systems, including the musculoskeletal system. It poses significant challenges to the hand surgeon, including calcinosis, ischemic changes, Raynaud phenomenon, tendinopathies, synovitis, and joint contractures. Patients with SSc also suffer from multiorgan dysfunction, which makes them high-risk surgical patients. The hand surgeon must understand the pathophysiology, treatment strategies, and special operative considerations required in this population to avoid complications and help maintain or improve hand function.
Introduction
Systemic sclerosis (scleroderma, SSc) is an autoimmune disease of unknown etiology that can cause significant dysfunction to multiple organ systems. Systemic sclerosis is a resultant of 3 pathogenic processes: obliterative vasculopathy, immune dysregulation with production of autoantibodies, and increased extracellular matrix and collagen production from fibroblast dysfunction. Ultimately these lead to progressive vascular insufficiency and fibrosis of the integumentary, musculoskeletal, cardiovascular, pulmonary, renal, and gastrointestinal systems.1,2
Systemic sclerosis is classified as either limited cutaneous scleroderma or diffuse cutaneous scleroderma (dcSSc) depending on extent of disease process. Limited cutaneous scleroderma has a prolonged disease course with skin manifestations typically limited distal to the elbows and knees, whereas dcSSc has a rapidly progressive course, extending proximal to the elbows and knees with marked trunk and multisystem organ involvement.1,3 Both subsets of SSc have significant hand manifestations including calcinosis, ischemic changes, Raynaud phenomenon (RP), tendinopathies, synovitis, and joint contractures. These manifestations place patients at risk for superficial and deep infections and wound healing complications. An understanding of the pathophysiology, and special operative considerations required in this population will allow hand surgeons to avoid complications and optimize treatment outcomes.
Calcinosis
Calcinosis cutis is defined as the deposition of insoluble calcium in the skin and subcutaneous tissues in the setting of normal calcium metabolism. 4 The prevalence of this condition in patients with SSc is approximately 22%, typically occurring about 10 years after diagnosis. 5 The pathophysiology of calcinosis cutis is largely unknown; potential mechanisms include local trauma, inflammation, vascular hypoxia, and dysregulation of bone matrix proteins leading to the accumulation of calcium deposits. The theory of microtrauma supports the fact that patients most commonly present with lesions in the subcutaneous tissues and fascia of the hands (more commonly the dominant hand) and feet. Also affected are the extensor surfaces of forearms, elbows, and knees. 5 Radiographs reveal 1 of the 2 characteristic patterns in the hand: widespread calcium deposits along the length of the finger or well-defined deposits at the distal tuft (Figure 1). 6 While often asymptomatic, severe calcinosis in the hands can lead to pain, soft tissue and joint contractures, and skin ulcerations. In the setting of superimposed ischemia, skin ulcerations place the patient at risk of soft tissue or deep infection as well. Given the unknown pathogenesis, treatment for calcinosis remains challenging. Although many medical therapies have been suggested (including calcium channel blockers, warfarin, bisphosphonates, rituximab, and sodium thiosulfate), there is limited evidence to support their use, given variable results and small trials. 7 For painful lesions, acetaminophen and nonsteroidal anti-inflammatory drugs can be used for symptomatic relief. Ultimately, surgical excision is the treatment of choice for symptomatic calcinosis, particularly in the setting of superimposed infection. The most common surgical technique involves simple excision with a scalpel and thorough curettage to ensure that all residual calcification is removed. For diffuse disease, the goal is debulking rather than complete excision. Incisions can be left open or closed depending on the size of the wound, although it is important to note that this patient population may be at a higher risk for wound complications secondary to vascular compromise. 7 Aside from surgical excision, other minimally invasive techniques have been described. Calcinosis has been treated using a high-speed burr procedure in which small stab incisions are made through which calcium deposits are burred and extruded with saline. 8 Lapner and Goetz 8 suggest that the high-speed burr technique should be reserved for focal calcinosis limited to 1 or 2 fingers. Finally, carbon dioxide laser therapy has been used to vaporize calcium deposits with moderate resolution of pain, although results show limited success. 9 It is important to note that asymptomatic lesions should not be treated surgically, given the high rate of recurrence and potential for wound complications.

(a) Anteroposterior and (b) lateral radiographs of the hand depicting calcinosis of the index finger tuft.
Ischemia
Ischemia associated with SSc is one of the most debilitating consequences of the disease, given the chronic pain and disability that ensues. It is now recognized that microvascular and macrovascular changes are a common finding in patients with scleroderma with a predominance of ulnar artery and superficial palmar arch involvement in the hand (Figure 2). 10 The narrowing of these major hand vessels in addition to microthrombi formation, tissue damage, and vasospasm leads to digital ulceration. Three types of digital ulcers have been identified by Hachulla et al 11 : fingertip (ischemic), extensor surface (mechanical), and calcinosis-associated ulcers (related to mechanical and inflammatory phenomena). Digital ulcers can result in significant morbidity, often becoming digit-threatening secondary to osteomyelitis or gangrene (Figure 3). 7 More than half of the patients with SSc will experience digital ulceration during the disease course, with one-third going on to recurrent ulceration despite pharmacologic treatment. 12
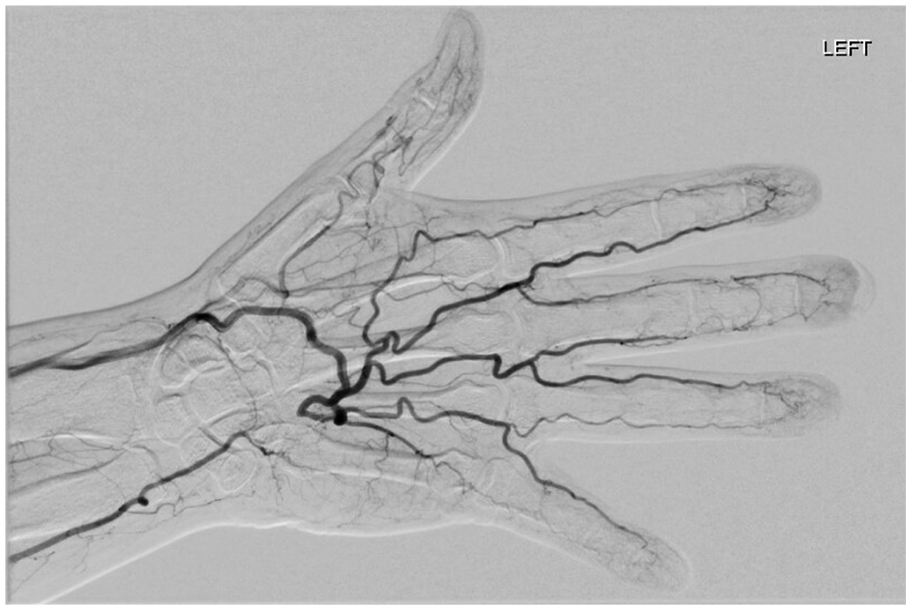
Arteriogram of a patient with systemic sclerosis and an ulnar artery thrombosis.
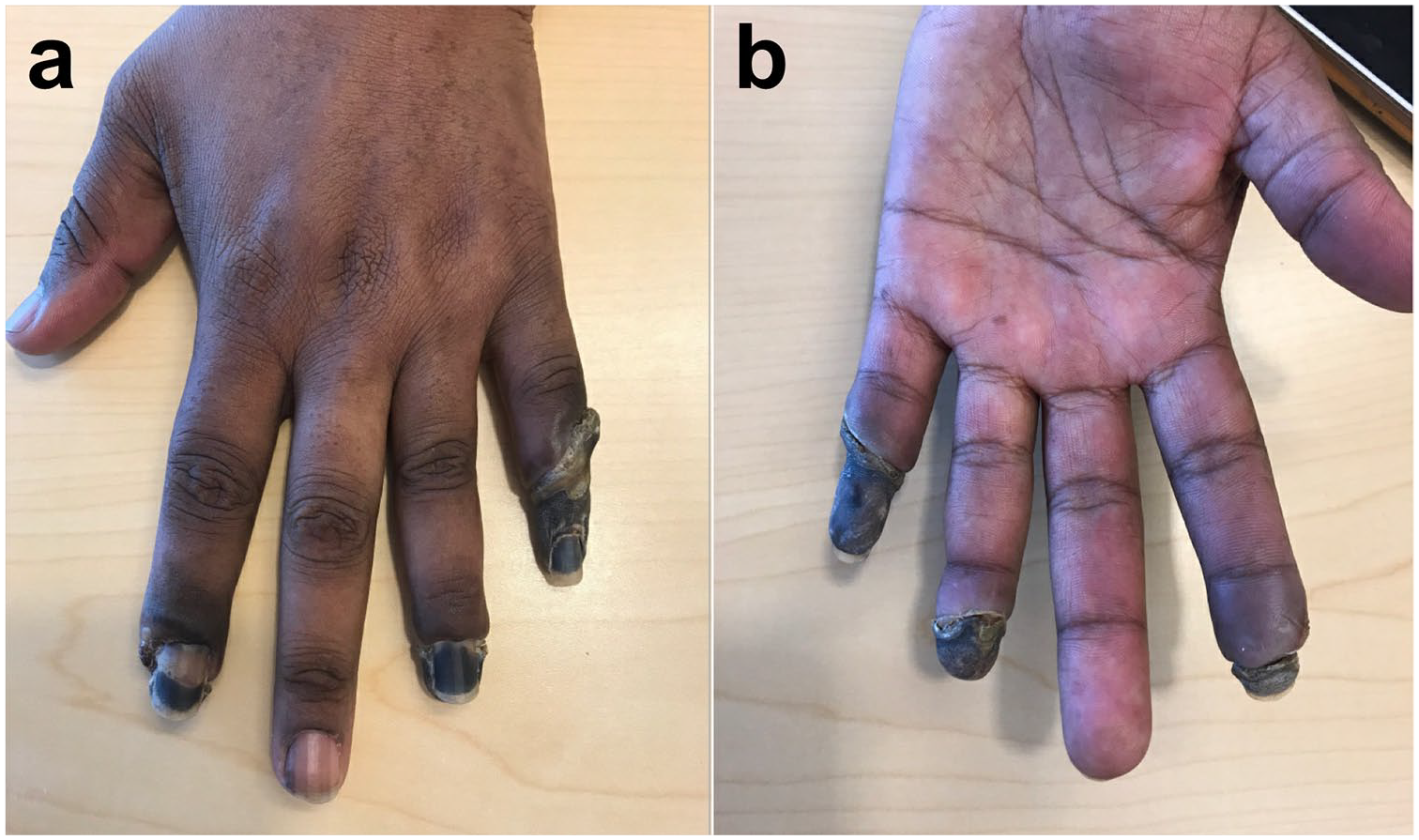
Dry gangrene as a result of ischemic changes in multiple fingertips in a patient with systemic sclerosis. (a) Posterior view. (b) Anteroposterior view.
The presence of underlying infection in the setting of digital ulcers is common, with Giuggioli et al identifying 67% of ulcers having a local infection (Figure 4). The most common organisms identified were Staphylococcus aureus followed by Escherichia coli/Enterococcus faecalis and Pseudomonas aeruginosa. 13 Osteomyelitis was identified in approximately 20% of patients in the study, with 11% of patients requiring digital amputations. Typical wound care for ulcers without overlying infection includes topical hydrogel with or without antimicrobial agents. Once an infection has developed, thorough irrigation and debridement of the wound is necessary to disrupt biofilm formation and remove nonviable tissue. If underlying osteomyelitis is present, the patient will likely need a long-term course of systemic antibiotics. Once dry gangrene has developed, the nonviable area is left to demarcate and eventually autoamputate. Autoamputation can take months to progress but is advantageous because length of the digit is preserved. Although surgical amputation is immediate, the creation of a new surgical wound in an area of compromised blood supply often results in wound complications. Therefore, formal amputation is reserved for severe cases or those with underlying infection. 7

Osteomyelitis of the index finger and second ray with overlying soft tissue infection in a patient with systemic sclerosis.
Raynaud Phenomenon
Raynaud phenomenon is seen in up to 96% of patients with SSc and is often the first manifestation of the disease. 7 It is characterized by vasospasm of the cutaneous arterioles of the hands in response to cold or increased sympathetic tone. 14 Patients typically experience episodic pallor or cyanosis of the digits induced by cold or stress. Raynaud phenomenon alone is typically benign, but when combined with the underlying vasculopathy of systemic scleroderma it can cause more severe changes. This is attributed to progressive endothelial damage, intimal hyperplasia, adventitial fibrosis, and luminal narrowing resulting in ulceration and chronic pain. 7
With regard to management of RP, patients are generally comanaged by a rheumatologist. It is advised that patients protect their hands from inciting events by keeping their hands warm in cold conditions and avoiding smoking. 7 Pharmacologic vasodilators are often prescribed as well to control the incidence of attacks. 15 Calcium channel blockers, most commonly nifedipine, are first-line therapy. 15 They have been shown to reduce both the frequency and severity of Raynaud attacks while also lowering the incidence of ulcerations. 16 Second-line treatment options include angiotensin II receptor blockers and phosphodiesterase 5 inhibitors (sildenafil and tadalafil); unfortunately, these are typically more expensive and have a higher side effect profile such as headaches, flushing, cough, dizziness, hypotension, and arrhythmias. 15 For severe symptoms and critical ischemia, prostaglandin analogs have become the standard of care but can be administered intravenously for 3 to 5 days, and are very expensive. 15
Given the propensity for these patients to go onto digital ulceration and gangrene, procedures have been developed in attempt to increase blood flow to the hand. The most common surgical intervention is periarterial sympathectomy (Figure 5). This involves microscopically stripping the arterial adventitia ultimately removing the sympathetic innervation from the distal hand vasculature. 7 The primary targets for sympathectomy include the radial and ulnar arteries, superficial palmar arch, and common digital arteries. The extent to which the dissection is carried out is variable, ranging from millimeters of the involved digit to an extensive approach extending into the forearm. 7 In general, it is recommended that 2 cm of adventitia be stripped from each vessel to ensure removal of sympathetic input. 7 Pace and Merritt 17 demonstrated favorable results with the extended periarterial sympathectomy in patients that had failed medical management, ultimately demonstrating improvements in ischemic pain, high rates of ulcer healing, and long-term patient satisfaction.

Patient with Raynaud phenomenon in the bilateral hands status after sympathectomies of the radial and ulnar arteries and palmer arch on the left upper extremity.
Chemical sympathectomy has also been described using botulinum A toxin for patients with RP.15,18 While there are several proposed mechanisms for the effect of botulinum A administered locally including inhibition of sympathetic vasoconstriction, inhibition of sensory nerves, and endothelial exocytosis of endothelin, the exact mechanism(s) remains unknown. 19 There has not been a consensus on dosing or injection protocols for botulinum A toxin, but most surgeons inject the toxin locally around the radial and ulnar arteries, the superficial palmar arch, and/or the digital vessels. While prospective studies have shown good results in patients with primary RP, the recent randomized controlled trial by Bello et al 18 demonstrated mixed results in patients with SSc-associated RP. In this study, they found a decrease in measured laser Doppler blood flow to the hands receiving botulinum A injection at 1 month compared with placebo; however, no difference in blood flow was seen at 4 months. The decrease in blood flow was more significant in patients with dcSSc and long-standing RP. Despite this finding, there was a trend toward improvement in pain scores in hands receiving botulinum A injections, although this was not clinically significant. 18 Based on the current literature, it is unclear whether the use of botulinum A toxin can provide benefit in patients with SSc-associated RP.
Tendon Involvement
Tenosynovitis is seen in up to 27% patients with scleroderma. Although some patients experience inflammatory tenosynovitis similar to rheumatoid arthritis, patients with SSc are more likely to have fibrotic tendon sheath thickening, termed “sclerosing tenosynovitis.” Extensor tendons are more likely to be affected than flexor tendons, and synovitis is present in approximately 46% of patients. There is also a correlation between the presence of tenosynovitis and active or severe disease. 20
Patients with dcSSc can present with characteristic tendon friction rubs (TFRs) described as leathery crepitus over tendons. 21 These TFRs can be present in ankles, knees, elbows, and wrist and are described in 6% to 37% patients with SSc.20,22 Specifically for the hand surgeon, these can be palpable over the flexor or extensor tendons at the wrist or fingers. 23 These TFRs were originally assumed to be from fibrinous deposits in tendon and tendon sheaths, 23 but newer imaging studies suggest the infiltrates are in the deep soft tissues and the fat septae, leading to thickening of the pulleys of the fingers and extensor/flexor retinacula. 24 Although these TFRs do not require surgical intervention, they are correlated with increased functional disability, fingertip ulcers/gangrene/amputations, and joint contractures.22,25 In addition, TFRs are associated with worsening disease severity; increased renal, cardiac, pulmonary, and gastrointestinal involvement; and decreased survival rates.22,25 Due to the association between TFRs and increased mortality, it is extremely important for the hand surgeon to ensure that patients presenting with TFRs are referred to a rheumatologist, for disease treatment and monitoring.
Synovitis and Arthritis
Joint pain is exceedingly common in patients with SSc, with some studies reporting arthralgias in up to 66% to 97% patients. Arthralgias present a notable challenge to this population, with most patients reporting significant pain and disability. 26 Arthralgias can be the presenting symptom of SSc, with up to 20% complaining of joint pain before SSc diagnosis. 26 Synovitis and arthritis on clinical examination can present in up to 46% of patients;20,27 however, subclinical synovitis can be detected in a much higher proportion on imaging studies.20,28 Radiographic studies demonstrate a wide range of joint pathology from inflammatory arthritis, including osteolysis and erosive changes, to osteoarthritis with subchondral sclerosis and osteophytes.26,27,29 The most common presentation, however, is joint space narrowing with or without bony changes. 29
Joint Contractures
Claw hand deformity with proximal interphalangeal (PIP) joint flexion contractures is present in up to 31% of patients with SSc and is often progressive.21,27 Contractures are more common in dcSSc but can occur in both subtypes.21,27,29 These contractures are a result of sclerosis of the skin, volar plate, and flexor tendon sheath with concomitant flexor tendon shortening. With time, central slip attenuation and lateral band volar subluxation ensues.7,23,30 Progressive PIP flexion contracture causes tension, ischemia, and atrophy of the dorsal skin leading to ulcerations and infections.7,30 Compensatory extension occurs at the metacarpophalangeal (MCP) joints, which can be worsened by sclerosis and contracture of the dorsal soft tissues.6,7,30
Procedures aimed to improve range of motion of the PIP joint, such as silicone arthroplasty and soft tissue releases, have been described. Outcomes of these procedures have been poor with significant residual stiffness. Therefore, most surgeons advocate for PIP arthrodesis. 7 Lipscomb et al 31 first described outcomes for hand surgery in 6 patients with SSc in 1969; he performed 17 PIP joint arthrodeses with complete fusion and healing in all patients. Many other surgeons have since reported their results with 94% to 100% fusion rates, minimal complications in wound healing, and improved hand function.6,30-34
Position of PIP joint arthrodesis has been described ranging from 30° to 60° of flexion, with increasing angle from the index finger to the small finger.6,30-33 Placing the joint in too much extension can place tension on the volar blood supply and lead to finger ischemia 6 ; therefore, it is imperative to assess distal finger blood flow intraoperatively and reposition the PIP joint accordingly. Lipscomb et al 31 advocated for more flexion for PIP fusion to ensure proper contact with the thumb for pinch grip. Given limited MCP motion and concomitant thumb deformities, the surgeon should use careful intraoperative assessment to place the joint in optimal functional position.
Melone et al described the vascular supply to the skin overlying the PIP joint and advocate for dorsal bipedicled flaps in the setting of PIP joint fusions in patients with SSc (Figure 6).6,32 These allow for excision of dorsal wounds and have shown excellent results for soft tissue healing. Tension band wires and dorsal plates have been described for PIP joint fusions in the general population. Tenuous dorsal soft tissues and progressive contractures in patients with SSc, however, increase the risk of hardware exposure and need for further surgery.6,7,33 It is therefore recommended that fusions be performed with Kirschner wires that can be easily removed in clinic postoperatively.6,7,33,34
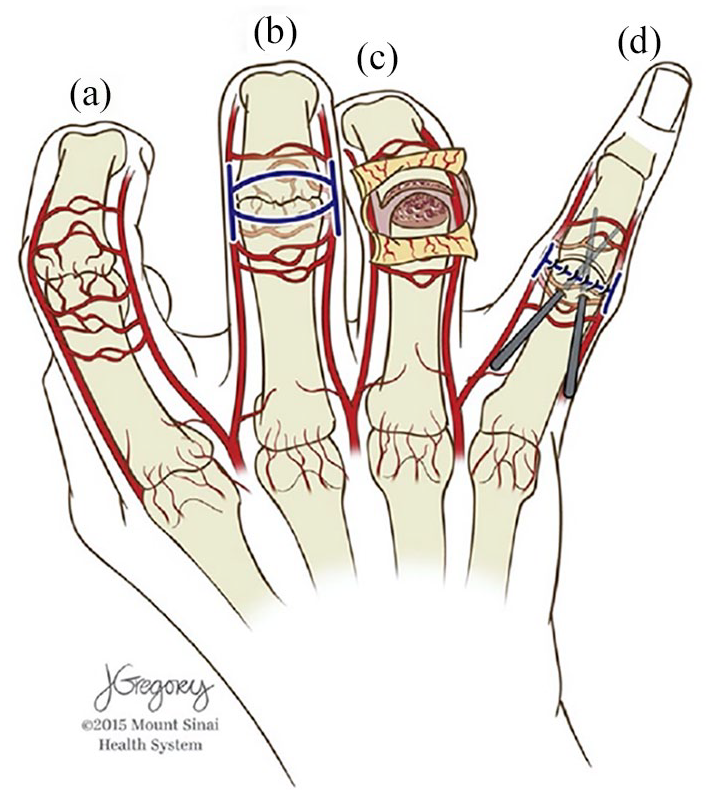
Dorsal bipedicle flap advocated by Melone et al for proximal interphalangeal (PIP) joint fusions.
To address hyperextension deformities at the MCP joint, both resection and silicone arthroplasties have been described.6,30-33 The risk of destabilizing the MCP joint is low due to the sclerosis and contracture of the surrounding soft tissues. 34 Therefore, complete metacarpal head and condyle resection is to remove tension on the soft tissues and regain motion. 6 These procedures provided only slight improvements in joint range of motion with an average of 50° arc postoperatively, but produce better position for overall hand function.6,30-33 Metacarpophalangeal joint arthroplasty can be performed through a single transverse dorsal incision allowing for complete joint exposure, preservation of periarticular vascular networks, and extensor mechanism centralization and repair. 32 It is important to note that extensive hand therapy may be required to maintain the range of motion of the MCP joints postoperatively and residual stiffness is common.6,30-33
Patients with SSc can develop adduction contractures of the thumb, along with trapeziometacarpal arthritis with compensatory hyperextension at the MCP joint.6,7,30 Surgical correction using trapeziectomy, adductor release, and/or MCP arthrodesis can be employed based on presentation.
Wrist Arthritis
Synovitis and arthritic changes of the wrist have also been reported in patients with SSc. Erosions and joint space narrowing are seen on radiographs, and synovitis is seen on advance imaging (ultrasound and magnetic resonance imaging).20,27,28 Limited studies exist comparing surgical interventions for synovitis and arthritis of the wrist in patients with SSc. Darrach distal ulna resection, wrist fusion, Sauve Kapandji procedure, and wrist total arthroplasty have all been described in this patient population.30,35 Further research is necessary to define the indications for operative intervention and to determine which operative procedure is most beneficial for patients with SSc.
Peripheral Neuropathies
Clinical symptoms of peripheral neuropathy, such as sensory disturbances, can be present in up to 40% of patients with SSc. 36 Carpal tunnel syndrome is the most common peripheral compressive neuropathy,36-38 but SSc can also present with cubital tunnel syndrome or mixed peripheral neuropathies.36,37 The etiology of these neuropathies has yet to be determined, but it is proposed that patients with SSc have fascicular loss and increased fibrotic deposits. 39 It is theorized that these changes could be from microangiopathy and nerve ischemia.36,39 These can be the earliest presenting symptoms of SSc, and a patient with compressive neuropathy combined with finger pain, swelling, and/or RP should be worked up for SSc.
Operative Considerations
Patients with SSc suffer from multiorgan dysfunction which makes them high-risk surgical patients, and a detailed preoperative medical evaluation is imperative. Due to facial skin and muscle tightness and stiffness, intubation can be difficult. 40 Proper ventilation can be inhibited by interstitial lung disease and pulmonary fibrosis, carrying a high risk of barotrauma. 40 In addition, trunk tissue fibrosis and muscle weakness carry the potential for postoperative respiratory failure. 40 For these reasons, regional anesthesia is preferred over general anesthesia to avoid complications.7,31,32,34,40
Due to distal soft tissue fibrosis, digital blocks can be extremely painful, and the local analgesic may have less potential to diffuse through the dense soft tissues. 34 Wrist blocks have been used successfully; however, some authors advocate for even more proximal blocks (such as scalene or brachial plexus) to avoid diseased soft tissues.33,34 It is important to note that patients with SSc can have prolonged sensory blockade after regional anesthesia, lasting up to 24 hours,33,40 and patients should be counseled preoperatively.
Local anesthesia with epinephrine is avoided in patients with SSc, given vasculopathy and potential for digital ischemia.7,32 If bleeding control is needed for visualization, a proximal arm tourniquet has been used successfully for 1 to 1.5 hours.6,31,34 To prevent vascular crisis, special attention should be given to patient warming and operating room temperature. 40
Conclusion
Systemic sclerosis is a complex autoimmune disease characterized by obliterative vasculopathy and multisystem fibrosis, leading to calcinosis, RP, digital ischemia, tendinopathy, joint arthropathy, and contractures. Surgeons should beware of the increased potential for vascular and wound healing complications, and pay close attention to surgical technique and soft tissue handling. In addition, patients with SSc can have increased perioperative risks necessitating proper preoperative workup and optimizing local anesthesia when possible. With increasing recognition of this complex disease and the unique surgical considerations it poses, complications can be avoided and surgeons can help improve or maintain hand function in this population.
Footnotes
Ethical Approval
This study did not require approval by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this review article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.