
Abstract
Background
We hypothesize that different positions of the wrist in the coronal plane makes the carpus susceptible to ulnar impaction.
Methods
We prospectively enrolled 10 adult volunteers and obtained fluoroscopic images of each wrist in 12 different positions using a standardized protocol. Distances from the ulna to the lunate (UL) and ulna to the triquetrum (UT) were digitally measured as was the portion of the lunate surface area that was uncovered (LUR) with wrist deviation.
Results
A wrist position of Pronation, Neutral Deviation, and Grip (P-ND-G) significantly shortened the ulnocarpal distance when compared to a position of Neutral Rotation, Neutral Deviation, and No Grip (NR-ND-NG). Radial deviation during pronation and gripping (Pronated, Radial Deviation, Gripping [P-RD-G]) resulted in the lowest mean UL distance (1.2 mm). UT distance was minimized by a position of ulnar deviation during a pronated grip (Pronated, Ulnar Deviation, Gripping [P-UD-G]) (3.1 mm). The lunate becomes more uncovered with radial deviation.
Conclusion
Radial deviation minimizes the UL distance while ulnar deviation minimizes the UT distance during a wrist position of pronation and gripping. Further, there is more proximal lunate surface area uncoverage during all positions of radial deviation compared to ulnar deviation.
Introduction
Ulnocarpal impaction (UCI), also known as ulnar impaction or ulnocarpal abutment, is a clinical term used to describe ulnar-sided wrist pain, swelling, and limitation of motion secondary to pathologic loading of the distal ulna against the triangular fibrocartilage complex (TFCC) and ulnar carpus resulting in progressive degeneration of both of these structures as well as attrition of the lunotriquetral (LT) ligament. 1 Given the myriad of pathologies that encompass the ulnar side of the wrist, a detailed history and clinical examination is needed.2,3 Patients are often focally tender over the site of impaction (lunate, triquetrum, ulnar head or styloid, etc.) and their pain is exacerbated when the wrist is in a position of pronation and ulnar deviation. 1 The ulnocarpal stress test, described by Nakamura and colleagues in 1997, involves placing the wrist in a position of maximal ulnar deviation and applying an axial load while taking the forearm through a passive arc of pronosupination. 4 While this test is sensitive for UCI, a positive test can occur due to several alternative pathologies. 2 Therefore, radiography has become a useful adjunct in diagnosing UCI. On standard, neutral PA radiographic views, UCI is characterized by degenerative changes to the ulnar-proximal side of the lunate, the radial-proximal aspect of the triquetrum, and the distal radial ulnar head.1,5-7 A pronated grip view has also been described to evaluate for positive ulnar variance, which has a strong association with UCI as it has been shown to shorten the ulnocarpal distance by 1 to 3 mm.1,8-10
The effect of wrist deviation on ulnocarpal relationships has been less well-studied. The authors of this study appreciated a change in the gross appearance of the proximal carpal row with radial deviation that would seem to make UCI more likely to occur. Furthermore, we recognized that no single radiographic view exists that demonstrates a position in which UCI is most likely to occur. Such radiographic views have been described for scapholunate instability, 11 radioulnar joint instability, 12 and skier’s thumb, 13 for example, and can aid in making a diagnosis when history, physical examination, and standard radiographic findings are equivocal. Furthermore, while many provocative tests have been described as being sensitive for detecting UCI, none of them are very specific. 2
Thus, we designed a study with the purpose of finding a position that had the greatest effect on minimizing the ulnocarpal distance with the rationale that this view may prove to be a practical and reproducible imaging technique to aid in the work-up of patients with suspected UCI. While patients affected by UCI most often describe pain when their wrist is loaded in a position of pronation and ulnar deviation, we hypothesize that the lunate will be closer in proximity to the distal ulna and most uncovered when the hand is in a pronated grip position in maximal radial deviation.
Materials and Methods
Following institutional review board (IRB) and radiation safety board approval, a prospective diagnostic study was conducted at a single academic medical center. Inclusion criteria consisted of healthy adult (≥18 years old) subjects. Volunteers expressed interest in study participation after seeing an IRB-approved flyer located in medical center common spaces. Any volunteer who had a prior wrist injury, procedure, surgery, diagnosis, or who had current wrist pain was excluded. Although the radiation exposure risks associated with digital fluoroscopic imaging of a distal extremity are minimal, females of child-bearing age were specifically asked about the possibility of pregnancy and were excluded if they answered affirmatively. All participating volunteers wore protective lead during imaging. The study cohort consisted of a sample of convenience of 10 volunteers (6 males and 4 females) with mean age 33.4 years (27-45 years). Hand dominance was evenly distributed.
Twelve fluoroscopic images of the left and 12 of the right wrist of each volunteer were obtained using a standardized protocol devised in conjunction with a certified radiographer and musculoskeletal consultant radiologist. These images were all posterioranterior (PA) views in the following wrist positions characterized by wrist rotation, wrist deviation and whether or not a gripping maneuver was being performed during image acquisition (Figure 1):
Neutral Rotation, Neutral Deviation, No Grip (NR-ND-NG) (a)
Neutral Rotation, Radial Deviation, No Grip (NR-RD-NG) (b)
Neutral Rotation, Ulnar Deviation, No Grip (NR-UD-NG) (c)
Neutral Rotation, Neutral Deviation, Grip (NR-ND-G) (d)
Neutral Rotation, Radial Deviation, Grip (NR-RD-G) (e)
Neutral Rotation, Ulnar Deviation, Grip (NR-UD-G) (f)
Pronated, Neutral Deviation, No Grip (P-ND-NG) (g)
Pronated, Radial Deviation, No Grip (P-RD-NG) (h)
Pronated, Ulnar Deviation, No Grip (P-UD-NG) (i)
Pronated, Neutral Deviation, Grip (P-ND-G) (j)
Pronated, Radial Deviation, Grip (P-RD-G) (k)
Pronated, Ulnar Deviation, Grip (P-UD-G) (l)
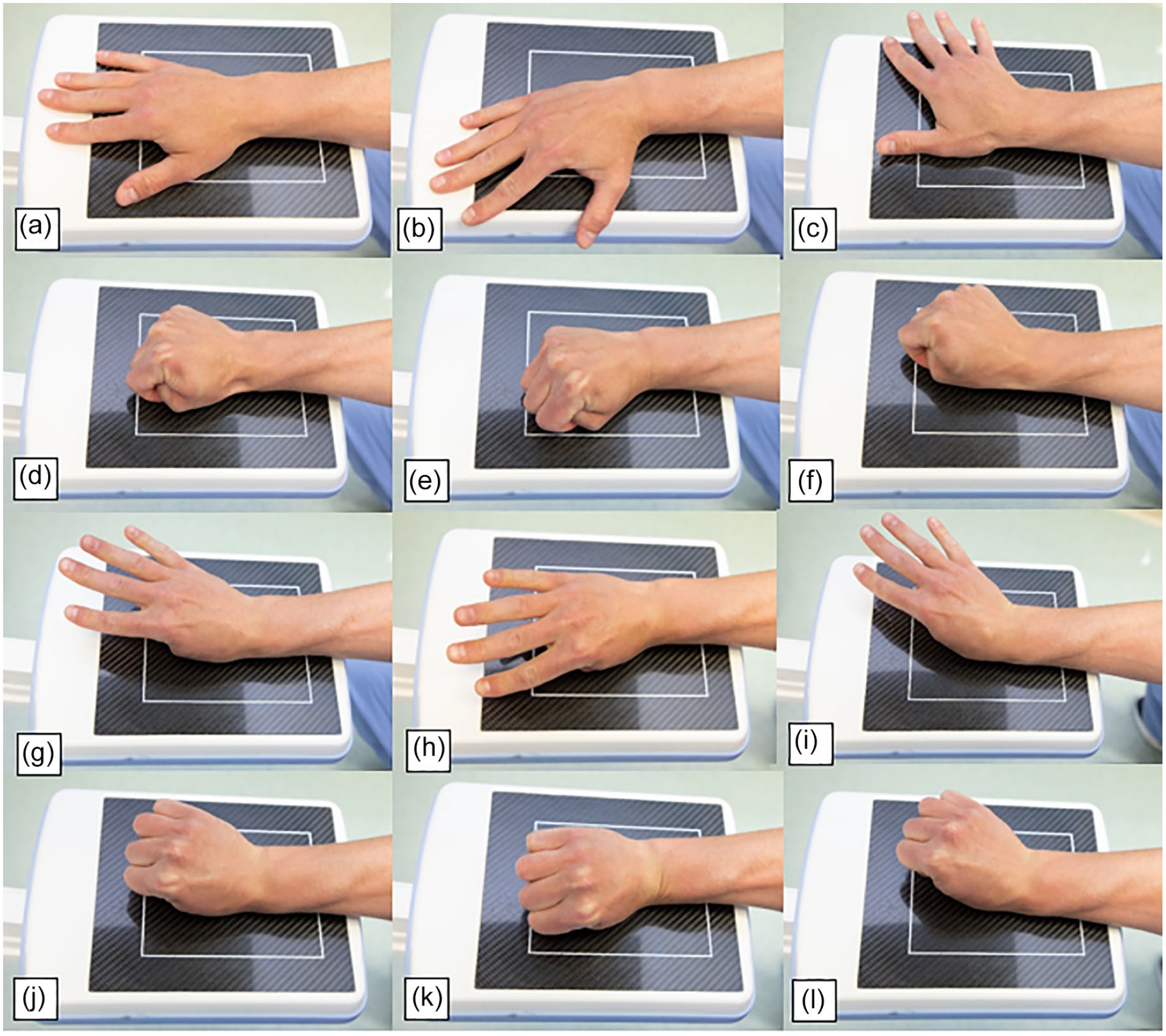
Fluoroscopic images were obtained in 12 different wrist positions characterized by wrist rotation, wrist deviation and whether or not a gripping maneuver was being performed during image acquisition.
To ensure consistency during radiographic examination, a certified radiologic technologist was available. A standard, neutral PA view of the wrist (NR-ND-NG) was obtained with the volunteer’s forearm in neutral rotation by positioning the arm in 90° of shoulder abduction and 90° of elbow flexion as has been previously used.8,9,14 A laser-aiming guide was used to mark the center of the wrist and maintain a centered wrist through all subsequent positions to reduce any parallax effect and ensure comparability of all measurements. Radially and ulnarly deviated views were obtained with the volunteer’s wrist actively in the maximum position of the respective motion. The arm was then repositioned to be at the volunteer’s side in complete adduction. Slight external rotation of the shoulder to 30° was instituted for ease of performing subsequent views. Grip views were obtained by asking the volunteer to make a fist with maximal force to maximize the relative length of the ulna. 14 Pronated rotation views were obtained by asking the volunteer to pronate the wrist such that the radial side of the thumb metacarpal was flat on the imaging detector.
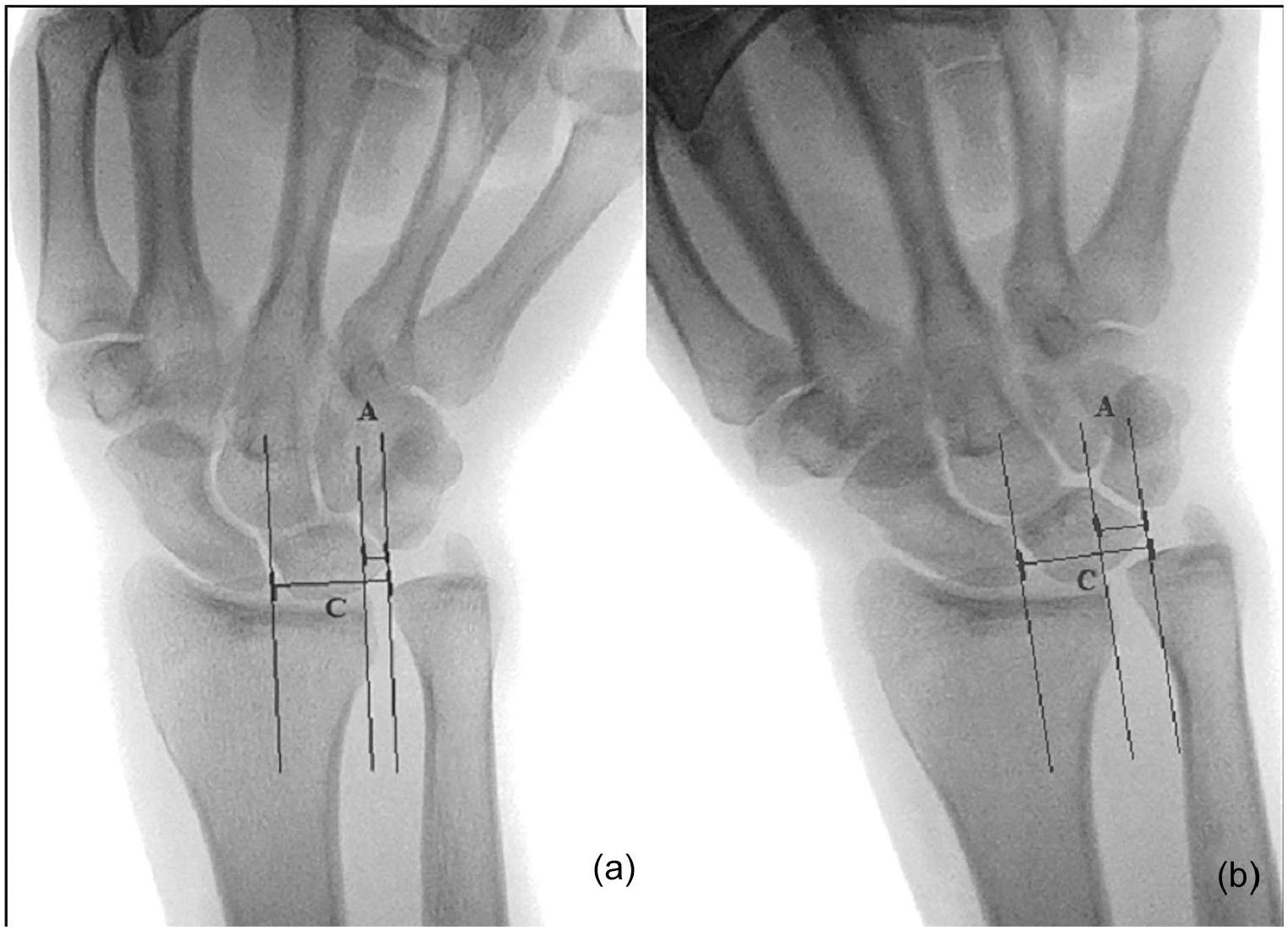
All fluoroscopic images were obtained using a single surgical mini C-arm (Fluoroscan Insight 2, Hologic, Inc., Danbury, Connecticut) and transmitted to a proprietary imaging viewer for collection of digital measurements (QREADS; Mayo Clinic, Rochester, Minnesota). All fluoroscopic images and all digital measurements were performed by a single researcher. Ulnolunate (UL) distance was measured as the shortest distance between the ulna and the lunate. 15 This was then repeated to obtain the ulnotriquetral (UT) distance. Example measurements of these distances are demonstrated in Figure 2. The lunate uncoverage ratio (LUR) was also digitally measured by taking the portion of the lunate extending ulnar to the border of the radius (A) and dividing by the entire width of the lunate (C) as determined by lines perpendicular to a line along the radial-most aspect of the distal radioulnar joint (DRUJ)10,16 (Figure 3). If none of the lunate extended ulnar to the border of the radius, than LUR was recorded as 0. A magnification marker taped to overlay the subcutaneous border of the ulna was used to scale each view.
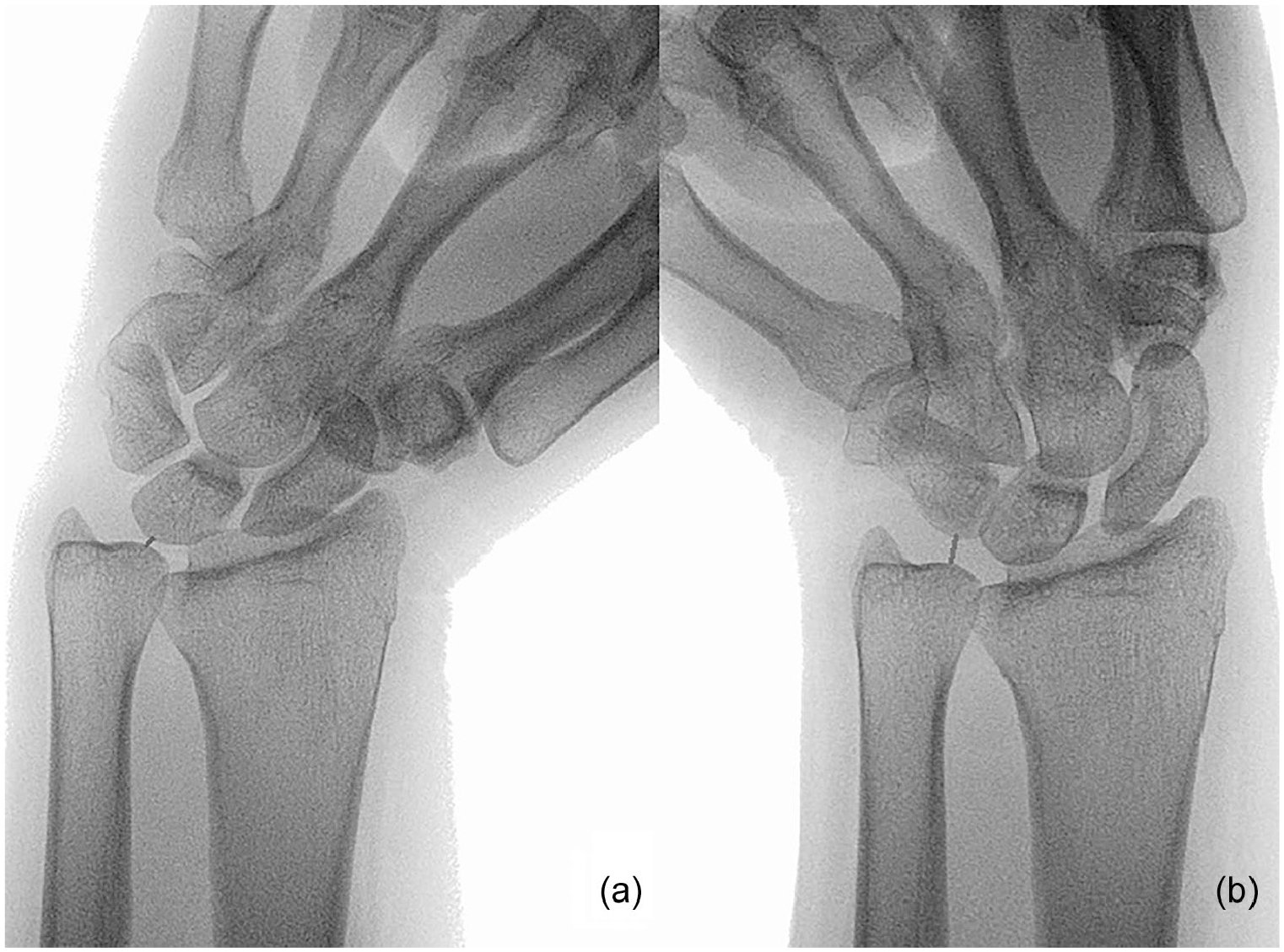
Left wrist demonstrating a pronated, grip (P-G) view with (a) radial deviation (RD)and (b) ulnar deviation (UD).
Each wrist, regardless of laterality or volunteer’s hand dominance, was considered independently for statistical analysis. Means were calculated for each dynamic fluoroscopic view. A repeated measures analysis of variance (ANOVA) followed by Tukey formal post hoc testing was then used to determine the significance of these results. Confidence intervals of 95% were used in all cases.
Results
Effect of Forearm Rotation on Ulnocarpal Distances
Pronation alone (P-ND-NG) significantly decreased UL and UT distances compared to neutral PA (NR-ND-NG) (UL 1.4 ± 0.3 mm, CI: 0.3-2.5, P < .05, UT 2.2 ± 0.6 mm, CI: 0.3-4.0, P < .05). Grip alone (NR-ND-G vs. NR-ND-NG) did not significantly change these distances (UL -0.9 ± 0.3 mm, CI: -0.2-2.0, P = .22, UT -1.5 ± 0.6 mm, CI: -0.4-3.3, P = .26). Pronated grip (P-ND-G) compared to grip alone (NR-ND-G) and neutral pronation alone (P-ND-NG) were also not significantly different (UL -1.1 ± 0.3 mm, CI: -0.0-2.2, P = .07, UT -1.3 ± 0.6 mm, CI: -0.6-3.1, P = .49; -UL 0.6 ± 0.3 mm, CI: -0.5-1.7, P = .83, UT -0.6 ± 0.6 mm, CI: -1.2-2.4, P = 1.00).
Effect of Wrist Deviation on Ulnolunate (UL) Distance
Mean UL and LT distances for each fluoroscopic view are included in Figure 4. The P-RD-G followed by the P-ND-G positions yielded the smallest UL distances (1.3 and 1.5 mm, respectively). Conversely, the NR-UD-NG followed by the NR-UD-G view had the largest distances (5.2 and 4.0 mm, respectively). The UL distance measured on the P-RD-G view was significantly different than 8/11 other positions (P < .05) (Table 1).
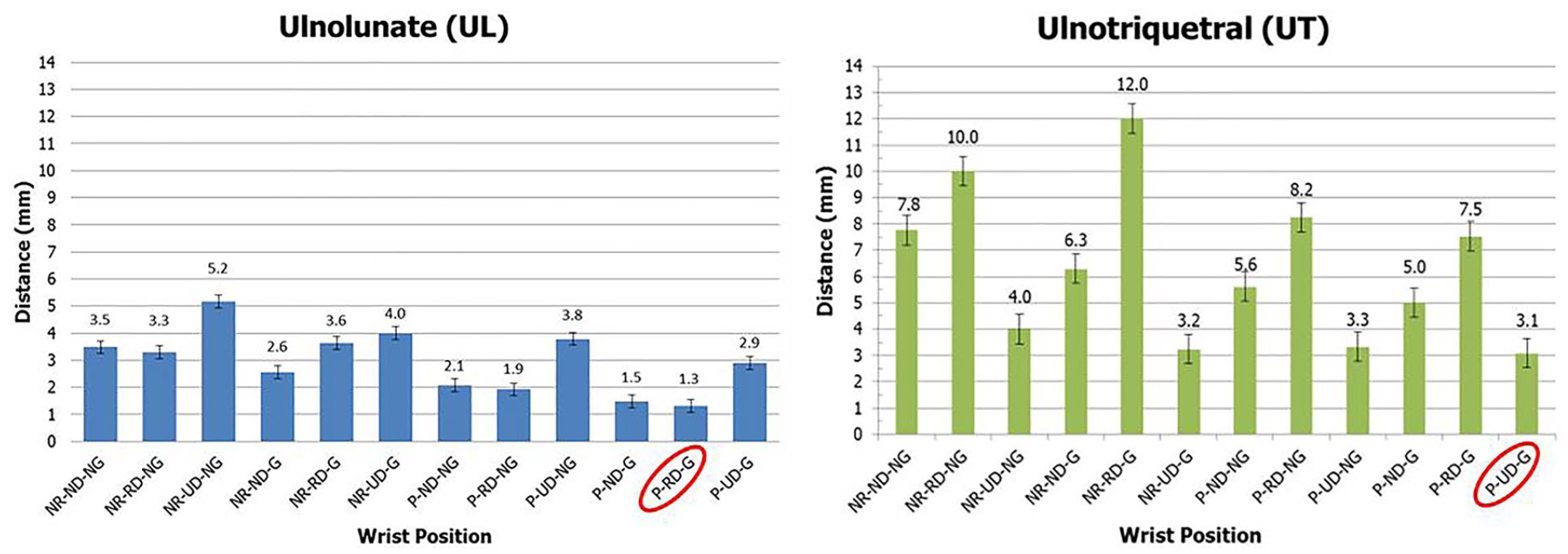
Mean ulnolunate (UL) and ulnotriquetral (UT) distances measured in various wrist positions. Error bars denote the pooled standard error estimate from the repeated measures ANOVA analysis.
Fluoroscopic Views With a Mean UL Distance That Was not Significantly Different From the P-RD-G Mean UL Distance of 1.31 mm.
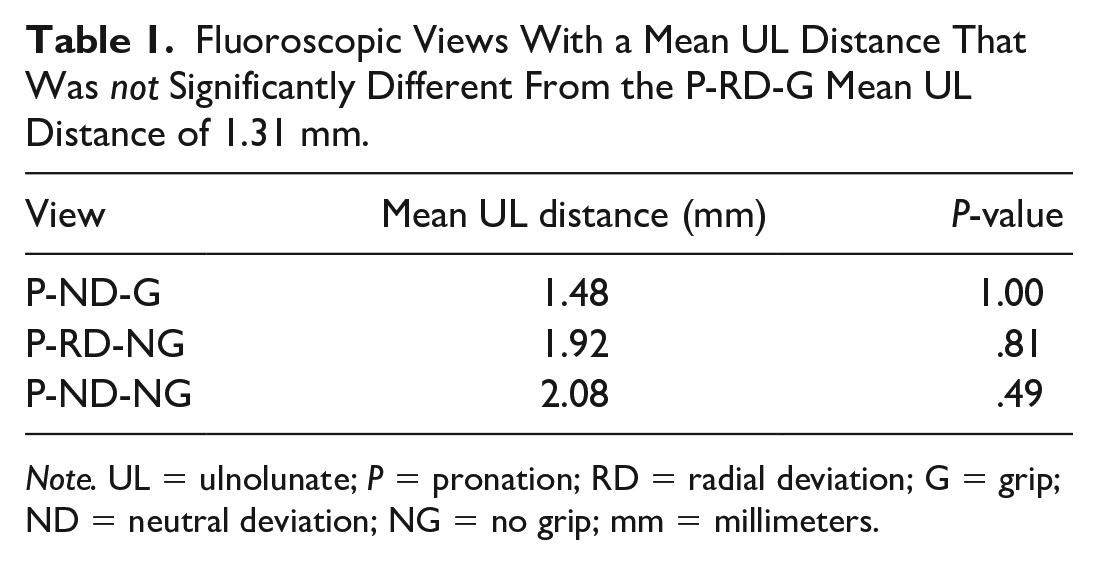
Note. UL = ulnolunate; P = pronation; RD = radial deviation; G = grip; ND = neutral deviation; NG = no grip; mm = millimeters.
While the mean absolute UL distances measured were smaller when comparing the P-RD-G and the P-ND-G, they were not significantly so (-0.2 ± 0.3 mm, CI: -0.9-1.3, P = 1.00).
Effect of Wrist Deviation on Ulnotriquetral (UT) Distance
The P-UD-G followed by the NR-UD-G view minimized UT distance the greatest (3.1 and 3.2 mm, respectively), while the NR-RD-G followed by the NR-RD-NG maximized UT distance (12 and 10 mm, respectively). The P-UD-G view yielded a UT distance that was significantly smaller than 8/11 other positions (P < .05) (Table 2).
Fluoroscopic Views With a Mean UT Distance That Was Not Significantly Different From the Pronated-Ulnar Deviation-Grip (P-UD-G) Mean UL Distance of 3.09 mm.
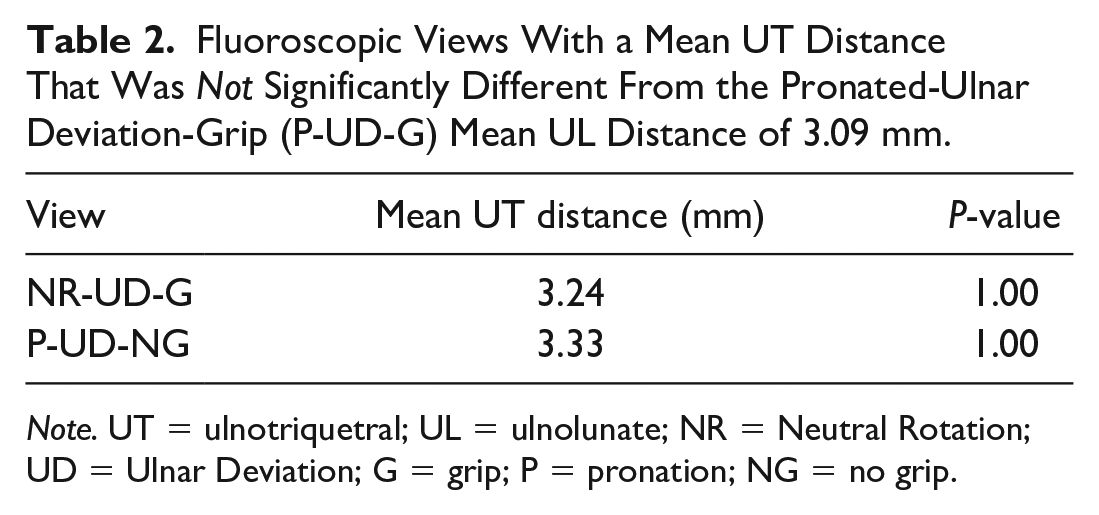
Note. UT = ulnotriquetral; UL = ulnolunate; NR = Neutral Rotation; UD = Ulnar Deviation; G = grip; P = pronation; NG = no grip.
Again, while the mean absolute UT distances measured were smaller when comparing the P-UD-G to the P-ND-G view, it was not significantly different (-1.7 ± 0.6 mm, CI: -0.2-3.5, P = .10).
Lunate Uncoverage Ratio (LUR)
In all instances NR-NG, NR-G, P-NG, P-G as the wrist moved from UD to neutral and from neutral to RD, LUR increased. This effect was significant from UD to neutral in all cases, but the effect of neutral to RD was only significant when grip (mean LUR of 0.3 with RD vs. 0.3 with ND, P < .05) or pronation (mean LUR of 0.3 with RD vs. 0.2 with ND, P = .03) were present alone and not when the wrist was in a neutral (NR-NG) position or a position of both pronation and grip (P-G). The mean LUR in all cases of UD was 0 (range: 0-0.3) compared to 0.3 (range: 0.1-0.6) in cases of RD. Finally, pronation (mean 0.2 vs. 0.4 with NR, P < .05) and grip (mean 0.2 vs. 0.4 with NG, P < .05) alone each significantly decreased LUR. In a position of pronation and ulnar deviation with and without grip (P-UD-G/NG), the lunate was almost completely covered (mean LUR = 0.03) in both positions.
Discussion
This study finds that a pronated grip view with the wrist in RD (P-RD-G) minimizes the distance of the distal ulna to the lunate, while a pronated grip view in UD (P-UD-G) minimizes the distance of the distal ulna to the triquetrum. Furthermore, in all cases of radial deviation, the proximal lunate surface area as determined by the LUR becomes more uncovered; conversely, a position of pronation and ulnar deviation (ie, the reported most clinically symptomatic position noted in patients with UCI) affords the lunate the greatest coverage. While these differences are small, the collective effect of radial deviation on a pronated grip may be clinically useful when attempting to demonstrate UCI in a clinical setting.
It is well known that the pathogenesis of UCI occurs under dynamic conditions. Both pronation and gripping maneuvers have been shown to relatively lengthen the ulna and reduce ulnar negative variance by a mean of 1 to 2 mm.1,8,9,10,14 While these changes are small, previous biomechanical work has shown that even minor changes in the proximity of the ulna to the ulnar carpus can substantially alter force distribution through the wrist joint. 17
However, while there is a higher incidence of impaction in ulnar positive wrists, this condition has also been observed in ulnar neutral and negative wrists.18,19 Furthermore, not everyone with an ulnar positive wrist has symptomatic UCI. 5 This suggests that pathologic impaction not only occurs dynamically, but that it cannot be explained by UV alone. The proportion of the axial load experienced by the distal ulna, the physical proximity of the distal ulna to the ulnar carpus, and, in our opinion, the amount of surface area of the proximal lunate exposed during dynamic maneuvers plays a role in the occurrence of pathologic UCI and may predict what portion of the carpus impaction will occur.
Compared to a standard, neutral PA of the wrist (NR-ND-NG), the present study found pronation alone (P-ND-NG) to significantly decrease UL and UT distances. We saw nonsignificant decreases in ulnocarpal distances with the addition of gripping to both a standard, neutral PA of the wrist (NR-ND) and a pronated wrist (P-ND). Logically, if grip had the effect of increasing UV in nonpathologic subjects, as has previously been shown,1,9,10,14 one would expect to see ulnocarpal distances decrease as well. Possible explanations for the absence of a significant “grip effect” in the present study include a dominating effect of pronation, a submaximal grip effort, insufficient sample size to show a significant difference, or the absence of a true effect due to gripping.
Clinically, worsening UCI symptomatology with grip, assuming grip did not have a significant effect on ulnar variance, could be explained by grip instead being a proxy for a loaded wrist. For example, the Nakamura test is not performed with a clenched fist but still can reproduce symptoms of UCI. 4 We would still recommend incorporating grip into imaging of patients with suspected UCI as it results in the lowest UL distance, despite it not being significantly different then with pronation alone. Further, we acknowledge that most patients with clinically apparent UCI describe pain with a loaded wrist.
Our study looked at ulnocarpal relationships during various wrist positions with and without static loading (ie, grip). We found a smaller but not significant difference in mean UL distance of 0.2 mm with RD (NR-RD-NG vs. NR-ND-NG) and a significant increase in UL distance of 1.7 mm with UD (NR-UD-NG vs. NR-ND-NG). We also found significantly different mean UT distances with wrist deviation of + 2.3 and -3.8 mm when comparing NR-RD-NG and NR-UD-NG to the NR-ND-NG view, respectively. Our interpretation of these findings is that the relationship of the proximal row to the distal ulna changes with wrist deviation, albeit less so with RD. During repetitive loading of a patient’s wrist through positions of wrist deviation, these smaller incremental reductions in ulnocarpal distances may account for the gradual genesis of symptomatic UCI in certain patients.
In a cadaveric study by Epner et al, it was noted that mean UV to change from negative 0.10 mm to negative 1.18 mm from pronation to supination. A further statistically significant increase in ulnar negative variance by 0.20 mm (P < .05) occurred when radial deviation was added to an already supinated wrist. 8 However, the authors found no effect on UV in the pronated wrist when wrist deviation was added. Thus, it seems that wrist deviation does not contribute to UCI through a mechanism of increasing UV. In contrast, the results from our study suggest that wrist deviation may play a role in UCI by decreasing the UL or UT distances or by changing the LUR.
The greatest change in the ulnocarpal relationship with wrist deviation, and perhaps the key to understanding the role of wrist deviation in UCI, is appreciating the LUR. To our knowledge, the effect of wrist deviation on LUR has not been previously examined in the literature. The present study found that a greater proportion of the lunate surface area is exposed when RD is added to a pronated or neutrally rotated wrist and that the lunate is almost always completely “covered” when UD is instead added. As such, in a position of RD, the uncovered lunate, articulating more with the TFCC and ulnar head, may in fact be in a more ompromising position for UCI.
Biomechanical data have demonstrated that an ulnarly deviated wrist position causes a greater proportion of axial load to be transmitted through the ulna when compared to RD. 17 Furthermore, the fact that patients complain of ulna-sided wrist pain and symptoms provoked by ulnarly directed stresses, would make it logical to conclude that the impaction event is occurring in ulnar deviation as well. 4 We propose 3 possible explanations to reconcile the results of this study with commonly reported clinical findings: (1) wrist deviation may be contributing to which aspect of the carpus is being pathologically loaded (ie, triquetrum in ulnar deviation and lunate in radial deviation), with pain generation from triquetral impaction being detected most during clinical evaluation; (2) impaction is occurring in radial deviation when the lunate is in closest proximity to the ulnar head and most “uncovered,” but an axial load through an ulnarly deviated wrist is most symptomatic due to greater force transmission through ulnocarpal joint in this position; and (3) when ulnarly deviated, less lunate surface area is uncovered and “available” for UCI. Thus, forces across the ulnocarpal joint in this position during loaded activities will be distributed over a smaller per unit area and may be a source of increased pressure and pain.
There were several limitations to this study. Radiographic measurements are prone to error. To mitigate this, we used a standard technique established by a certified radiologic technologist to acquire all images and did so on the same fluoroscopic device. We eliminated interobserver error by having 1 researcher take all fluoroscopic images and make all measurements while recognizing this can introduce intra-observer error. Further, a digital ruler was used to minimize errors in measurements. Still, it is always possible that minute discrepancies in image acquisition or measuring techniques impacted results. While we did encourage all subjects to put forth maximal effort with grip and maximal active motion into each desired position, the amount of grip force and the degree of motion, respectively, were not standardized across subjects. This may have contributed to the nonsignificant effect of grip on ulnocarpal relationships. Nonetheless, we feel that this would most replicate the clinical environment as patients with ulnar wrist pain may have differing levels of exertion and pain when asked to perform a grip view. We used fluoroscopic images for our volunteer cohort due to their lower radiation exposure, simplicity and speed of obtaining images in various wrist positions, and potential for the results of this study to be transferrable to a surgeon’s clinical practice. The fixed x-ray source and image receptor associated with fluoroscopy also eliminated changes in the x-ray beam incident angle inherent to conventional radiography. Our volunteer cohort was limited to a sample of 20 wrists from 10 subjects. This sample of convenience was chosen given the premise of previous research studies4,8,10,11,15 and to maximize sample size while also limiting the total number of subjects exposed to radiation. However, this approach may have subjected us to type II error. Even so, left to right comparison of ulnar variance within individuals has previously been shown to differ by > 1 mm in 40% of cases. 20 Left to right asymmetry was further appreciated in a more recent 3D analysis of radioulnar relationships for purposes of corrective osteotomy surgery. 21 Our volunteer cohort was without a comparison UCI cohort. Inclusion of a comparison cohort could be performed in the future to demonstrate how ulnocarpal relationships change in subjects with a diagnosis of UCI. Finally, variables such as the thickness of lunate cartilage, subchondral bone density, and quality and thickness of the TFCC were not explored and could have impacted measures recorded for analysis in this study.
Notwithstanding these limitations, this study demonstrates the purpose of obtaining different views to aid in the diagnosis of UCI. A P-RD-G and P-UD-G may assist the practitioner if ulna-lunate or ulna-triquetral impaction is suspected, respectively, by emphasizing their relative proximities with wrist deviation. Further study is needed to explore how wrist deviation affects LUR in patients with UCI and contributing to symptomatology. Specifically, we believe expanding on previous attempts 15 of using 3-dimensional computed tomography to more reliably and accurately measure ulnocarpal distances and LUR in various wrist positions and in a comparative cohort of patients with and without symptoms of UCI would be a potential area of future investigation.
Footnotes
Author Contributions
All the named authors actively involved in the planning, enactment and writing up of the study.
Ethical Approval
Statement of Human and Animal Rights
Procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 and 2008.
Statement of Informed Consent
Informed consent for research purposes was obtained per institutional protocol. Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kakar is a consultant for Arthrex and while a consultant for Arthrex, we had no funding and no relevant conflicts for this. The other author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.