
Abstract
Background
Returning to the office for an unplanned visit postoperatively can be burdensome to both the patient and provider. The purpose of this study was to quantify the rate of unplanned office visits after common soft tissue hand surgeries and assess the reasons for these unplanned visits.
Methods
Patients who underwent common soft tissue hand surgeries over a 6-month time period were queried from an electronic medical record database. Manual chart review was performed to record patient demographics, unplanned visits within 3 months postoperatively, and specific reasons for unplanned visits. A total of 1648 postoperative follow-up visits in 1224 patients were included in analysis.
Results
Within 3 months of surgery, 6.3% (103/1648) of postoperative visits were found to be unplanned. There was no difference in the rate of unplanned visits among the included surgeries (P = .46). The most common reasons for an unplanned office visit overall were wound problems (34%), pain (23.3%), and stiffness (17.5%). The trigger finger release group had significantly more patients return to the office for stiffness (P = .01), the De Quervain release group had significantly more patients return for pain (P = .02), and the carpal tunnel release group had significantly more patients return for persistent symptoms (P < .05).
Conclusions
Unplanned office visits represented about 1 of 16 postoperative visits. Orthopedic surgeons should be aware of the most common reasons for these visits and be prepared to address these problems promptly. Preoperative patient education on these potential problems may help decrease the frequency of unplanned follow-up visits.
Introduction
Unplanned office visits in the postoperative period can be burdensome to the patient and provider. Common soft tissue hand surgeries are generally effective and safe. 1 Given the low rate of complications with these procedures, a single postoperative visit for suture removal can be sufficient if a patient is otherwise doing well postoperatively and demonstrates appropriate symptom improvement. Any additional follow-up visits for common hand procedures can be planned if necessary.
Returning to the office for an unplanned office visit outside of scheduled follow-up is inconvenient and stressful for the patient. These visits may also place financial strain on the provider and practice, as additional visits during the global postoperative period are seldom reimbursed. The frequency of and reasons for unplanned postoperative office visits in hand surgical practice is presently unknown. We therefore sought to quantify the rate of unplanned office visits after common soft tissue hand surgical procedures. The factors contributing to such visits were secondarily assessed. We hypothesized that wound complications would account for most unplanned visits, and that there would be no difference in the rates of unplanned visits among common hand surgical procedures.
Materials and Methods
Institutional review board approval was obtained before initiation of this study, with a waiver of informed consent per institutional protocol. A query of our outpatient electronic medical record database was performed to identify all patients who underwent an isolated soft tissue hand surgery. We chose to evaluate 4 common soft tissue procedures (trigger finger release [Current Procedural Terminology {CPT} codes: 26145, 26055], open carpal tunnel release [CPT code: 64721], endoscopic carpal tunnel release [CPT code: 29848], and De Quervain release [CPT code: 25000]) performed by a fellowship trained orthopedic hand surgeon over a 6-month time period between January 31 and July 31, 2019. These procedures are typically followed by a single planned postoperative visit. Patients with a concomitant bony procedure on the same surgery date were excluded, and patients with more than 1 surgical procedure during this time frame were not collected to prevent potential crossover with office visits between separate procedures.
One thousand two hundred seventy-one individual patients were identified in the initial search. Forty-seven patients were excluded, leaving 1224 patients included in the analysis. Billing codes were reviewed to identify patients who had more than 1 postoperative visit based upon the CPT code 99024 within 3 months of surgery. Manual chart review was performed on all patients who had more than 1 postoperative office visit. Each clinical progress note was reviewed to identify whether the follow-up visit was planned or unplanned. An unplanned visit was defined as any office visit related to a patient’s surgical problem that occurred after the surgeon discharged the patient or gave the patient instructions at a prior visit to follow-up as needed. Basic patient demographics and specific reasons for unplanned office visits were recorded.
Descriptive statistics were used to report patient demographics and frequencies of surgical procedures and unplanned visits. A student’s t test was used to compare continuous variables between groups, and a χ2 test was used to compare the differences in categorical variables between groups. Statistical significance was set at P < .05.
Results
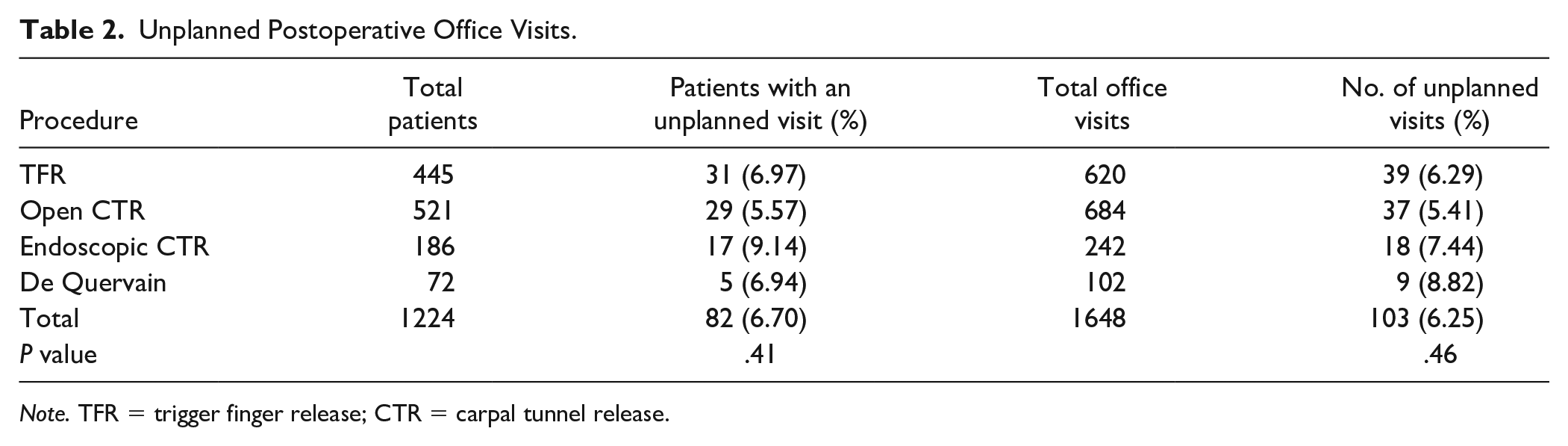
There were 1224 surgeries performed, and there were 1648 total postoperative follow-up visits included in analysis. Average age was 62.6 years (range: 18-96 years) with 464 men (37.9%) and 760 women (62.1%). (Table 1) The most common surgical procedure was open carpal tunnel release in 521 patients (42.6%), followed by trigger finger release in 445 patients (36.4%), endoscopic carpal tunnel release in 186 patients (15.2%), and De Quervain release in 72 patients (5.9%).
Demographics.
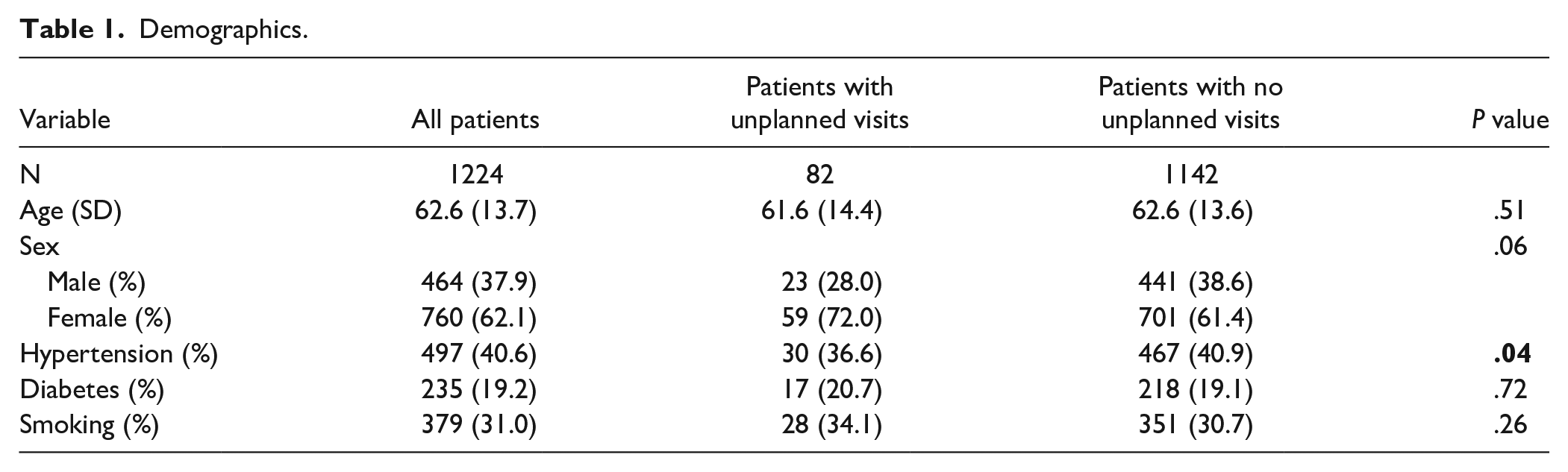
Eighty-two patients (6.7%) had an unplanned office visit postoperatively. These 82 patients had a total of 103 unplanned office visits, representing 6.3% of all postoperative office visits. There was a significantly higher percentage of patients with hypertension in the group without an unplanned office visit (P = .04). (Table 1) There were no other differences in demographics between patients with and without an unplanned office visit. There were no significant differences in the rates of unplanned visits between the 4 included surgical procedures (P = .46). (Table 2)
Unplanned Postoperative Office Visits.
Note. TFR = trigger finger release; CTR = carpal tunnel release.
The most common reasons overall for returning to the office for an unplanned visit irrespective of surgery type were wound problems (34%) followed by pain (23.3%) and stiffness (17.5%) (Table 3). The trigger finger release group had a significantly greater proportion of patients return to the office for stiffness (33.3%) compared with the other surgical procedures (P = .01). The De Quervain release group had a significantly greater proportion of patients (66.7%) return to the office for complaints of pain (P = .02). Carpal tunnel release patients had a significantly greater proportion of patients return with complaints of persistent symptoms (P < .05) compared with all procedures; however, there was no significant difference comparing this outcome between open versus endoscopic carpal tunnel release patients (P = .61). There were no other significant differences between the returning complaints for the different surgical procedures (P > .05) (Table 3). Open carpal tunnel release patients more commonly returned for an unplanned visit for wound problems (43.2%) compared with endoscopic carpal tunnel release patients (22.2%); however, this difference was not statistically significant (P = .13). Endoscopic carpal tunnel release patients returned for an unplanned visit more commonly for infection (22.2%) than did open carpal tunnel release patients (13.5%); however, this difference was also not statistically significant (P = .41).
Reason for Unplanned Postoperative Office Visits.
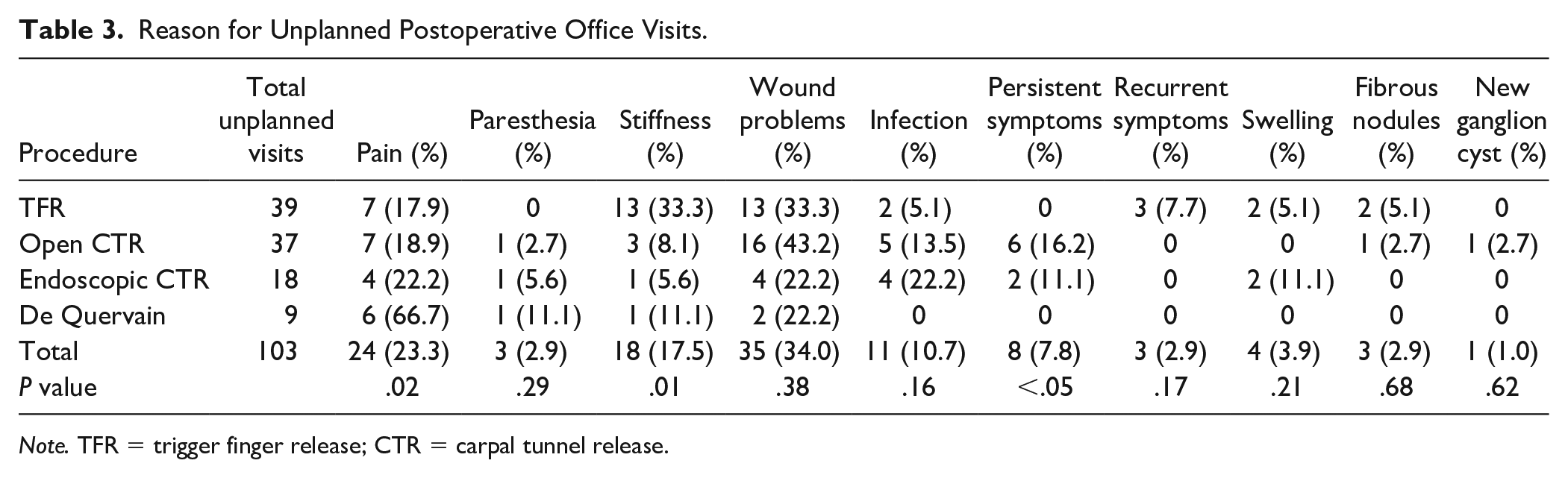
Note. TFR = trigger finger release; CTR = carpal tunnel release.
Discussion
This study found that 6.3% of office visits for postoperative patients within 3 months following hand surgery are unplanned visits. With about 1 of 16 postoperative office visits being unplanned, it is likely surgeons encounter these types of visits regularly in clinic, which likely represent more demanding encounters for the provider.
Wound problems, stiffness, and pain were the most common complaints for these unplanned follow-up visits. Few studies have evaluated unplanned return visits in outpatient settings. However, in a retrospective study of the National Surgical Quality Improvement Project database, Donato et al found that wound complications and uncontrolled pain were the most common diagnoses for unplanned hospital readmissions within 30 days following outpatient hand surgery. 2 Postoperative pain following outpatient hand surgery has also been recognized as the leading cause for emergency department visits within 30 days postoperatively. 3 Therefore, it is important for surgeons to recognize and address these problems early to prevent adverse outcomes such as emergency department visits and hospital readmissions in their postoperative patients. In our cohort, no patients who returned for an unplanned visit needed to be sent to the hospital or emergency department for higher level treatment, and all patients who returned with wound problems or infections resolved with conservative management and/or oral antibiotics.
In patients who underwent trigger finger release, the most common reasons for unplanned office visits were wound problems, stiffness, and pain. Our findings are consistent with those of Will and Lubahn, who reported the most common complications following trigger finger release in order of occurrence were stiffness, pain, and wound problems. 4 Recurrent triggering was noted as the reason for unplanned office visits in 3 patients (7.7%) in our study. Turowski et al observed recurrent triggering in 3.4% (2/59) of patients who underwent primary trigger finger release, all of which occurred within 6 months postoperatively, with 1 patient requiring reoperation. 5 Turowski et al collected their outcome data via phone calls, so it is unclear how many, if any, patients returned to their office for their complaints.
The most common reasons for patients to have an unplanned office visit following both open and endoscopic carpal tunnel release were wound problems, pain, infection, and persistent symptoms. A systematic review and meta-analysis of randomized controlled trials evaluating open versus endoscopic carpal tunnel release found that patients who underwent endoscopic carpal tunnel release had a significantly lower likelihood of scar complications than those who had open carpal tunnel release. 6 This is consistent with our findings in this study in which we found that wound problems were more common in open versus endoscopic carpal tunnel patients. While we did not find a significant statistical difference, we were likely underpowered in this subgroup. Also consistent with our findings, this meta-analysis found no statistical difference between postoperative infection, pain, or persistent symptoms between open and endoscopic carpal tunnel release patients. 6
De Quervain release patients in this study had a higher proportion of unplanned office visits that were due to postoperative pain compared with the other 3 procedures studied. These findings are consistent with those of Ta et al, who reported pain as the most common complication following De Quervain release, seen in 23% (10/43) of surgical patients in their study. 7 It is believed that persistent pain following De Quervain release could potentially be due to incomplete surgical decompression of the compartment, although no patients in our study required revision release or additional intervention. 8
New fibrous nodules were the reason for 3 unplanned visits (2.9%) overall. This occurred in 2 patients following trigger finger release, and 1 following open carpal tunnel release. Although anecdotal reports and limited published data suggest that Dupuytren nodules can occur after surgery or trauma, 9 we could not identify any study documenting the incidence of de novo fibrous nodules after hand surgery. This occurrence likely has a patient-specific genetic component rather than a direct correlation to the surgical procedure.
Both patients and surgeons should be aware that although soft tissue hand surgical procedures may be considered minor surgeries, complications and complaints can arise that could necessitate additional follow-up or an adjustment in standard follow-up protocols. Unplanned postoperative office visits can represent an opportunity for surgeons to identify these issues and treat them appropriately before patients experience more severe adverse outcomes. There is very limited literature available on postoperative follow-up visit protocols in hand surgery. After the initial office visit for an upper extremity fracture treated nonoperatively, Finger et al allowed patients to choose whether to have additional follow-up visits afterward. 10 They reported that 53% (64/120) of patients chose not to schedule an additional follow-up visit, indicating that for some low-risk hand musculoskeletal conditions, patients may feel comfortable to follow up on an as-needed basis. However, to ensure optimal outcomes, surgical patients likely necessitate more stringent follow-up protocols. Future studies should evaluate optimal postoperative follow-up protocols in hand surgery to further characterize and limit unplanned postoperative office visits.
Limitations of this study include its retrospective nature and the inherent biases of retrospective design. The data presented are the incidence of unplanned office visits and their reasons, not the overall complication rates in these procedures. We were unable to assess how many patients had complications or complaints that were managed via telephone calls with the office. In addition, we based our study on the 3-month postoperative time frame for visits, given the use of CPT code 99024 for the postoperative 90-day global period only. This method may not capture the entire scope of patient follow-up visits if follow-up extended beyond 3 months, and there could potentially have been even more unplanned office visits for these surgeries that occurred beyond the 3-month cutoff point.
While most patients who undergo common soft tissue hand surgical procedures require only a single postoperative visit, unplanned postoperative office visits do occur. Surgeons should be aware of the most common reasons for unplanned office visits following common hand surgical procedures. In light of the results of our study, we try to counsel patients preoperatively and at their initial postoperative follow-up visit about what to expect during the recovery period. Potentially, this better prepares patients for the symptoms they are likely to experience and may help decrease the need for in-person unexpected and unplanned follow-up.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
No human or animal subject was subjected to bodily or psychological harm in this study.
Statement of Informed Consent
No identifiable patient information was used in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.