
Abstract
Ligament reconstruction tendon interposition (LRTI) and suture-button suspensionplasty (SBS) are both common treatment options for trapeziometacarpal osteoarthritis. The primary purpose of this systematic review was to compare the subjective improvement in patient-reported outcomes in regard to disability for patients undergoing LRTI and SBS for trapeziometacarpal osteoarthritis. A secondary purpose was to compare the subjective improvement, objective outcome scores, and complication rates following both procedures. We performed a systematic review using PubMed, Scopus, and Embase to compare the clinical outcomes of LRTI and SBS. Inclusion criteria were level I-IV evidence articles reporting postoperative Disabilities of the Arm, Shoulder, and Hand (DASH) or QuickDASH scores. Study methodological quality, risk of bias, and recommendation strength were assessed. This systematic review included 31 studies for final analysis with 1289 thumbs undergoing LRTI (25 studies) and 113 thumbs undergoing SBS (6 studies). Both procedures demonstrated similar improvement in DASH and/or QuickDASH scores, while key pinch and grip strength inconsistently improved following both procedures. Complication rate was similar between the 2 procedures; LRTI 12% and SBS 13%. Although both LRTI and SBS seem to provide improved short-term patient-reported functional improvement and objective strength, there was significant heterogeneity within the included studies, and those studies discussing SBS were of lower quality evidence than those of LRTI. Thus, to truly delineate whether a difference exists between these 2 techniques for the treatment of first carpometacarpal joint arthritis, larger prospectively designed studies of high-quality evidence are necessary.
Introduction
Symptomatic osteoarthritis of the thumb (first) carpometacarpal (CMC) joint or trapeziometacarpal joint, also known as basilar thumb arthritis, can be a painful diagnosis, particularly when pinching or gripping objects. This diagnosis affects between 5% and 33% of adults in their 5th and 6th decades of life with a propensity for postmenopausal women.1-3 Post-mortem studies have demonstrated an incidence of close to 75%. 4 There are multiple potential etiologies of basilar thumb arthritis, but ultimately it leads many patients to report functional limitations including pain, weakness, loss of dexterity, pinch strength, or grip strength leading to significant disability.5-7 Often nonsurgical management of thumb CMC arthritis is effective including rest, activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), splinting, therapy, and corticosteroid injections.5,8,9 There is a poor correlation between radiographic Eaton-Littler stage and symptom severity.10,11 When nonsurgical management fails to improve a patient’s symptoms and functional disability, surgery may be indicated.
Hundreds of potential surgical techniques have been described for thumb CMC osteoarthritis including, but not limited to, metacarpal osteotomy, arthrodesis, and removal of the distal half of the trapezium or complete trapeziectomy followed by ligament reconstruction, interposition (tendon or other substance), suspensionplasty, or prosthetic arthroplasty. However, the gold standard remains trapeziectomy with ligament reconstruction with tendon interposition (LRTI) using the longitudinal radial one half or the entire width of the distal 10 to 12 cm of the flexor carpi radialis (FCR) tendon.12-14 With the development of minimally invasive implants, the use of suture-button suspensionplasty (SBS) with trapeziectomy has gained popularity after early studies utilizing this technique demonstrated good outcomes while allowing for early mobilization without thumb subsidence.15-17 However, comparative studies between these 2 techniques, LRTI and SBS, are not available.
The primary purpose of this systematic review is to compare the patient-reported outcomes, specifically Disabilities of the Arm, Shoulder, and Hand (DASH) and QuickDASH scores, between SBS and LRTI. A secondary purpose was to compare the subjective improvement, objective outcome scores, and complication rates following both procedures. The authors hypothesize that both interventions will result in similar functional outcomes, grip strength, pinch strength, and complication rates.
Materials and Methods
The systematic review was registered with PROSPERO (CRD42020214224) and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed. 18
Search Strategy
The authors conducted separate searches on November 9, 2020 utilizing the following databases: PubMed, Scopus, and Embase. The main search was performed in PubMed using controlled vocabulary (MeSH) and natural language (title, abstract, and other terms). Search terms focused on: (1) “disability” OR “patient outcome assessment” OR “strength” OR “pinch”; (2) [“trapeziometacarpal” OR “carpometacarpal” OR “base of the thumb” OR “basilar thumb”] AND [“osteoarthritis” OR “arthritis”]; and (3) “ligament reconstruction” OR “tendon interposition” OR “suture-button” OR “suspensionplasty” OR “tight-rope.” These terms were tested for relevancy in PubMed and, once finalized, were translated into Scopus and Embase for article retrieval. All duplicates were removed prior to screening to determine which articles were included in the final analysis.
Eligibility Criteria
Eligible studies consisted of Level I-IV studies published in the English language that investigated the results of LRTI or SBS for treatment of first CMC joint osteoarthritis. Both print and electronically published journal articles were eligible for inclusion. Screening was performed independently by 2 reviewers (A.E.W. and A.H.) using a prior methodology following PRISMA guidelines. 19 Initial screening of titles and abstracts were performed in Rayyan QCRI using the predetermined inclusion criteria on whether the manuscript contained DASH or QuickDASH scores for patients undergoing LRTI or SBS. After initial abstract screening, full-text articles were assessed for eligibility. Any disagreements at the end of each step were settled by discussion between the 2 reviewers. In all cases, a consensus was reached.
Study Selection
All references within included studies were cross-referenced and assessed for potential inclusion if missed by the initial search. LRTI was defined by harvesting a strip of the FCR tendon, re-routing this graft through a drill hole in the base of the first metacarpal (to mimic the anterior oblique ligament), and interposing the remaining FCR tendon in the void created after trapeziectomy.20-22 SBS was defined as any technique involving either a partial or complete trapeziectomy (open or arthroscopic) while utilizing at least one endobutton for suspension without the use of a tendon graft. Exclusion criteria included cadaver studies, biomechanical studies, traumatic causes of first CMC instability, and surgical techniques other than LRTI or SBS. Level V evidence (i.e. expert opinion), case reports, letters to editors, medical conference abstracts, and synthetic review articles (systematic review, meta-analysis, scoping review) were also excluded. In the situation of duplicate studies from the same author(s) and/or institution(s) reporting on the same or overlapping subjects, only one study was retained (highest level of evidence, largest number of subjects, longest follow-up, most pertinent primary outcome score) while the other(s) were excluded.
Data Extraction and Synthesis
From each article, details regarding the participants (female/male, mean age, diagnosis), intervention (SBS or LRTI), and outcomes (subjective patient-reported outcomes [DASH or QuickDASH scores], objective outcomes [grip strength, key pinch], and complications) were extracted. When possible, the outcome score and strength measurement from the furthest postoperative time measurement were utilized. Based on prior studies, a 10-point difference in mean DASH score was considered to represent the minimal clinically important difference (MCID),23-26 while MCID was represented by a 15-point difference in mean QuickDASH score.24,26,27 Data extracted from graphs that was not reported in data tables was rounded to the nearest whole number. When available, the range was provided for patient age and length of follow-up. Study type and design were assessed. Levels I, II, III, and IV of evidence were assigned to studies according to the Oxford Center for Evidence Based Medicine. 28 Evidence of each study was evaluated using Grading of Recommendations of Assessment, Development, and Evaluation (GRADE) criteria. 29 Meta-analysis was precluded based on the heterogeneity of the included studies and their mostly retrospective, noncomparative nature.
Appraisal of Evidence
The methodological quality of the included studies was rated out of 24-points using the methodological index for nonrandomized studies (MINORS) criteria for nonrandomized, comparative studies. 30 Given the inherent biases with retrospective case series, only study designs containing a comparative group were assessed for bias. For nonrandomized, comparative studies, the risk of bias in nonrandomized studies-of interventions (ROBINS-I) criteria was used to assess bias. 31 For randomized control trials, bias was assessed using the revised Cochrane risk-of-bias for randomized trials (RoB 2) criteria. 32 Recommendation regarding the quality, quantity, and consistency of evidence was made using Strength of Recommendation Taxonomy (SORT) criteria. 33 These assessments were performed by 1 author (A.E.W.) and independently checked by another author (A.H.).
Results
Database searches of PubMed, Scopus, and Embase produced a total of 1164 titles, which was reduced to 541 unique titles after de-duplication. After screening the abstracts of these unique titles, 350 failed to meet the inclusion/exclusion criteria. This left 191 full-text articles, which were assessed for eligibility. After this assessment, 31 articles met all inclusive/exclusive criteria and were included in the final analysis—as demonstrated in a PRISMA flowsheet (Figure 1). 18
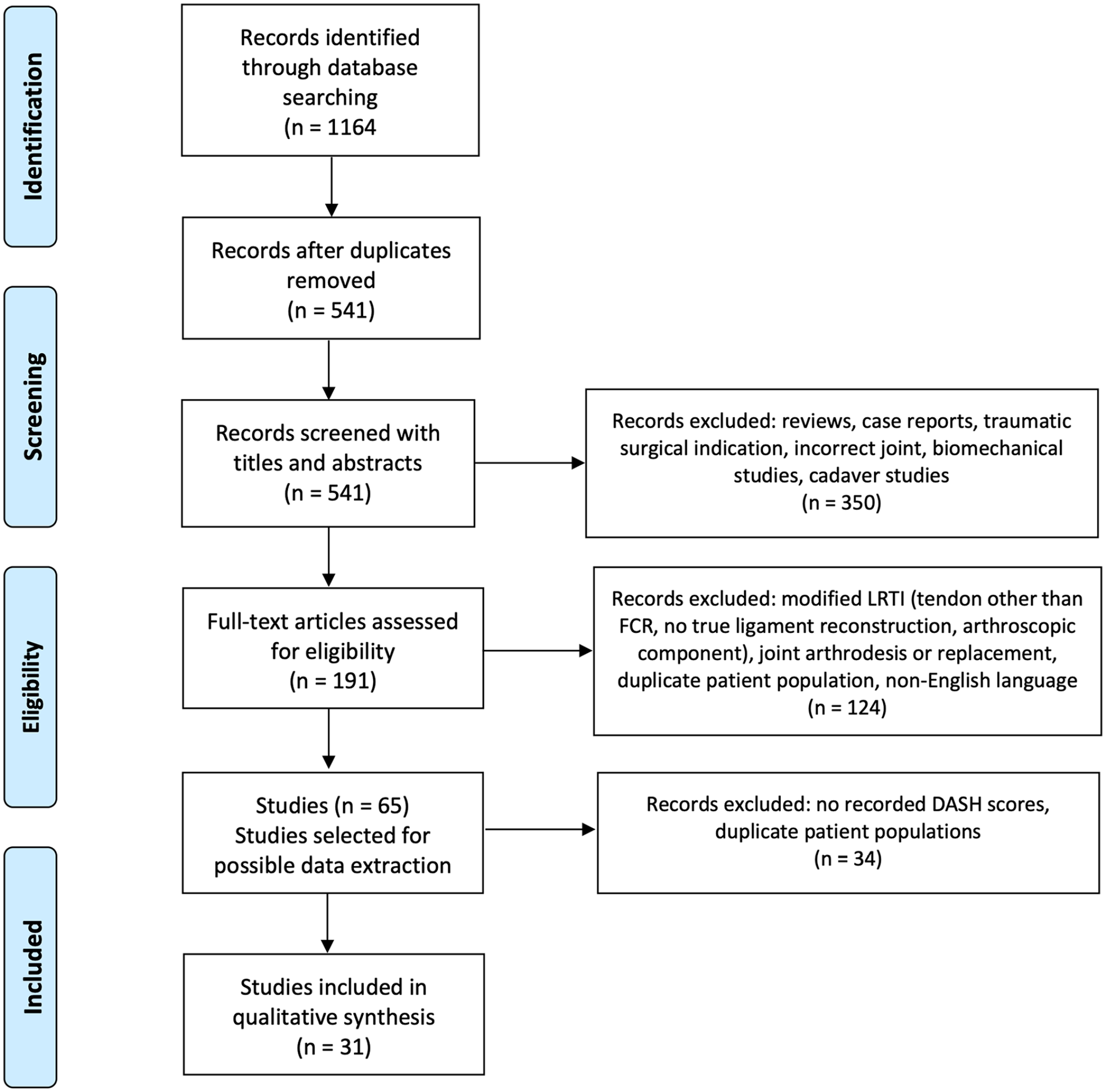
Flow chart application of exclusion criteria for study inclusion.
Design and Appraisal of Evidence
All 31 included publications were therapeutic studies, with 14 being level-IV evidence, 9 level-III evidence, 5 level-II evidence, and 3 level-I evidence (Supplemental References). Only 2 studies were given high level of evidence via GRADE, which were both level-I evidence randomized controlled trials containing LRTI patient cohorts. Based on the level and quality of evidence, MINORS criteria, and the ROBINS-I or RoB 2 assessments, the included LRTI studies are SORT B recommendation (based on inconsistent or limited-quality patient-oriented evidence) and the included SBS studies are SORT C recommendation (based on case series) (Table 1).
Summary of Included Studies.
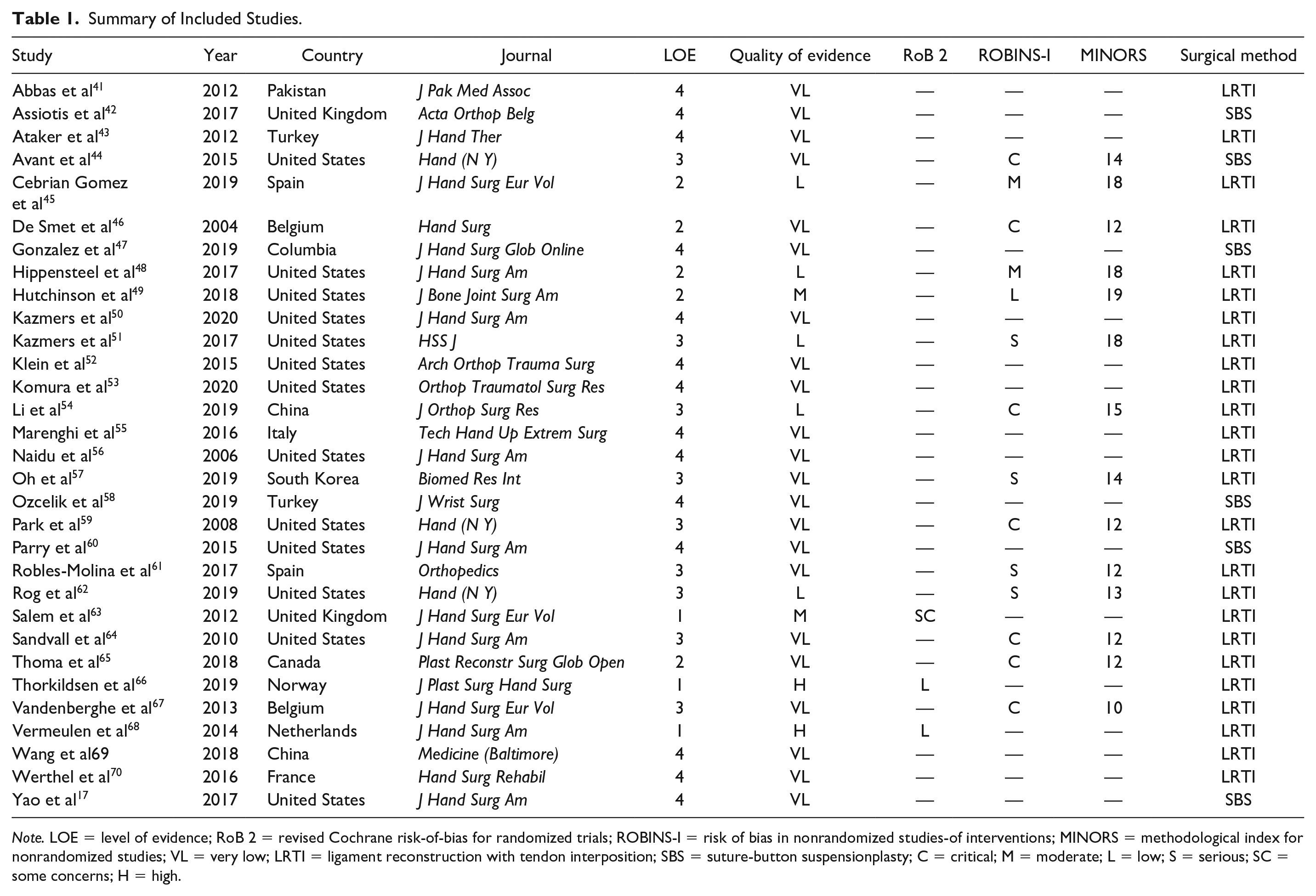
Note. LOE = level of evidence; RoB 2 = revised Cochrane risk-of-bias for randomized trials; ROBINS-I = risk of bias in nonrandomized studies-of interventions; MINORS = methodological index for nonrandomized studies; VL = very low; LRTI = ligament reconstruction with tendon interposition; SBS = suture-button suspensionplasty; C = critical; M = moderate; L = low; S = serious; SC = some concerns; H = high.
Population
Overall, there were 25 studies that reported DASH or QuickDASH scores following LRTI on 1289 thumbs from 1158 patients (897 females, 189 males), which excludes 1 study that did not report sufficient data on included patients. There were 6 studies that reported DASH or QuickDASH scores following SBS on 113 thumbs from 109 patients (87 females, 22 males). The average patient age was greater than 60 in 17 of the 25 LRTI cohorts and 5 of the 6 SBS cohorts. All patients were diagnosed with osteoarthritis of the trapeziometacarpal joint based on history, physical exam, and imaging. Twenty-three of 25 LRTI studies had a mean follow-up greater than 12 months, and 4 of 6 SBS studies had a mean follow-up greater than 18 months. Only 3 LRTI studies and 1 SBS study had mean follow-up greater than 60 months (Tables 2 and 3).
Individual Study Demographics and DASH Scores for LRTI Cohorts.
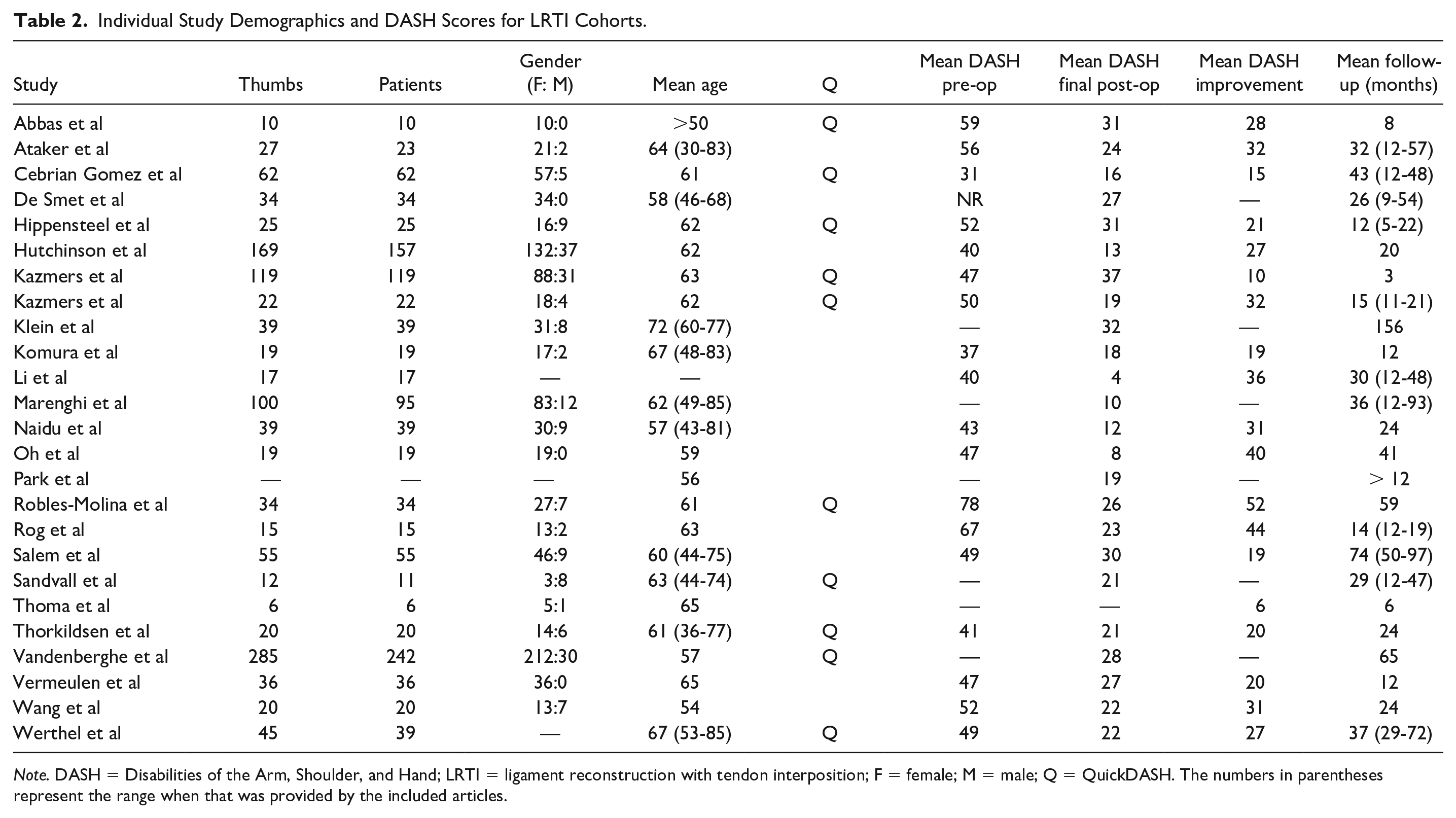
Note. DASH = Disabilities of the Arm, Shoulder, and Hand; LRTI = ligament reconstruction with tendon interposition; F = female; M = male; Q = QuickDASH. The numbers in parentheses represent the range when that was provided by the included articles.
Individual Study Demographics and DASH Scores for SBS Cohorts.
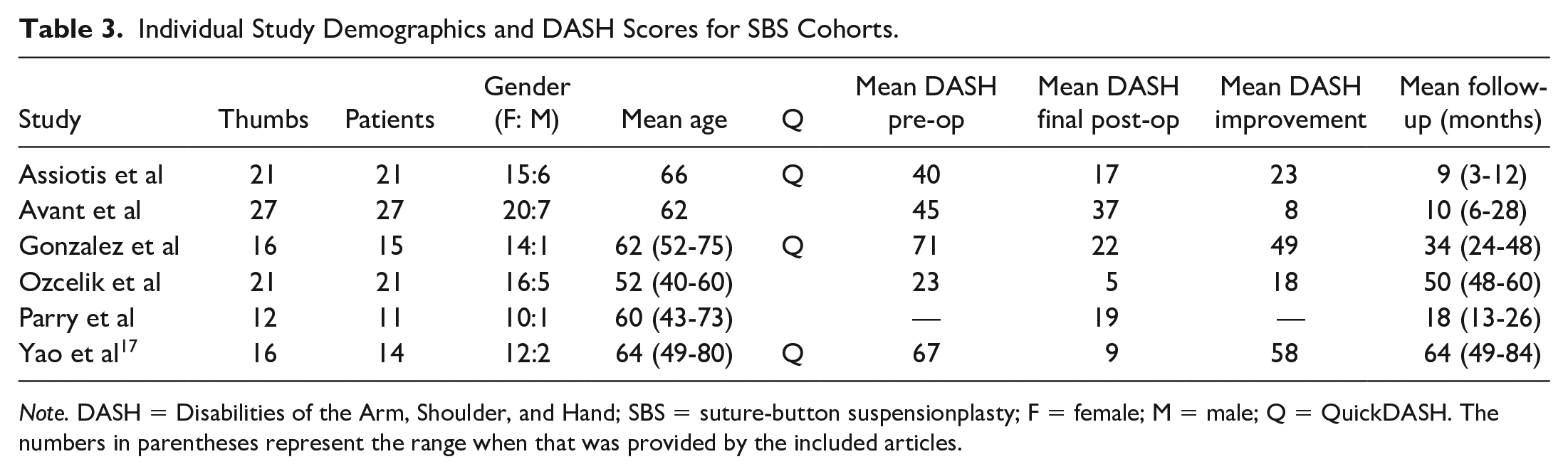
Note. DASH = Disabilities of the Arm, Shoulder, and Hand; SBS = suture-button suspensionplasty; F = female; M = male; Q = QuickDASH. The numbers in parentheses represent the range when that was provided by the included articles.
Outcomes
When collected both pre- and postoperatively, mean DASH and QuickDASH questionnaire scores always improved following both LRTI and SBS. Six of the LRTI studies included only postoperative DASH or QuickDASH scores, and the improvement was not reported. Of the remaining 19 LRTI studies, 10 of 11 utilizing DASH scores reported mean improvement greater than the MCID of 10 points, and 7 of 8 utilizing QuickDASH scores reported mean improvement greater than the MCID of 15 points (Table 2). One of the SBS studies included only postoperative mean DASH score and the improvement was not reported. Of the remaining 5 SBS studies, 1 of 2 studies utilizing DASH scores reported mean improvement greater than the MCID of 10 points and 3 of 3 studies utilizing QuickDASH scores reported mean improvement greater than the MCID of 15 points (Table 3).
Results of grip strength and key pinch were more inconsistently reported across cohorts undergoing both procedures (Supplemental Tables S1 and S2). For LRTI studies, 17 reported a change in grip strength following surgery, of which 16 studies demonstrated increased strength, and 18 reported a change in key pinch following surgery, of which 10 demonstrated increased strength. For SBS studies, 4 reported a change in grip strength following surgery, of which all 4 demonstrated increased strength, and 4 studies reported a change in key pinch following surgery, of which 3 demonstrated increased strength.
Adverse Events
Reporting of complications differed greatly between studies. Overall, when reported, complications occurred in 12.2% of the 740 patients undergoing LRTI and 13.3% of the 113 patients undergoing SBS (Table 4). Paresthesias, dysesthesias, or neuromas of the superficial radial nerve were the most common complication within both patient populations. There were 6 re-operations in the LRTI studies (of which 4 came from randomized controlled trials) and 2 re-operations in the SBS studies. The reasons given for re-operation in the LRTI patients were metacarpophalangeal hyperextension, tendinitis, neuroma, or persistent pain.The reasons given for re-operation in the SBS patients were both hardware related, one for prominent hardware and the other for hardware loosening.
Complications and Their Incidence Among Both LRTI and SBS Cohorts.
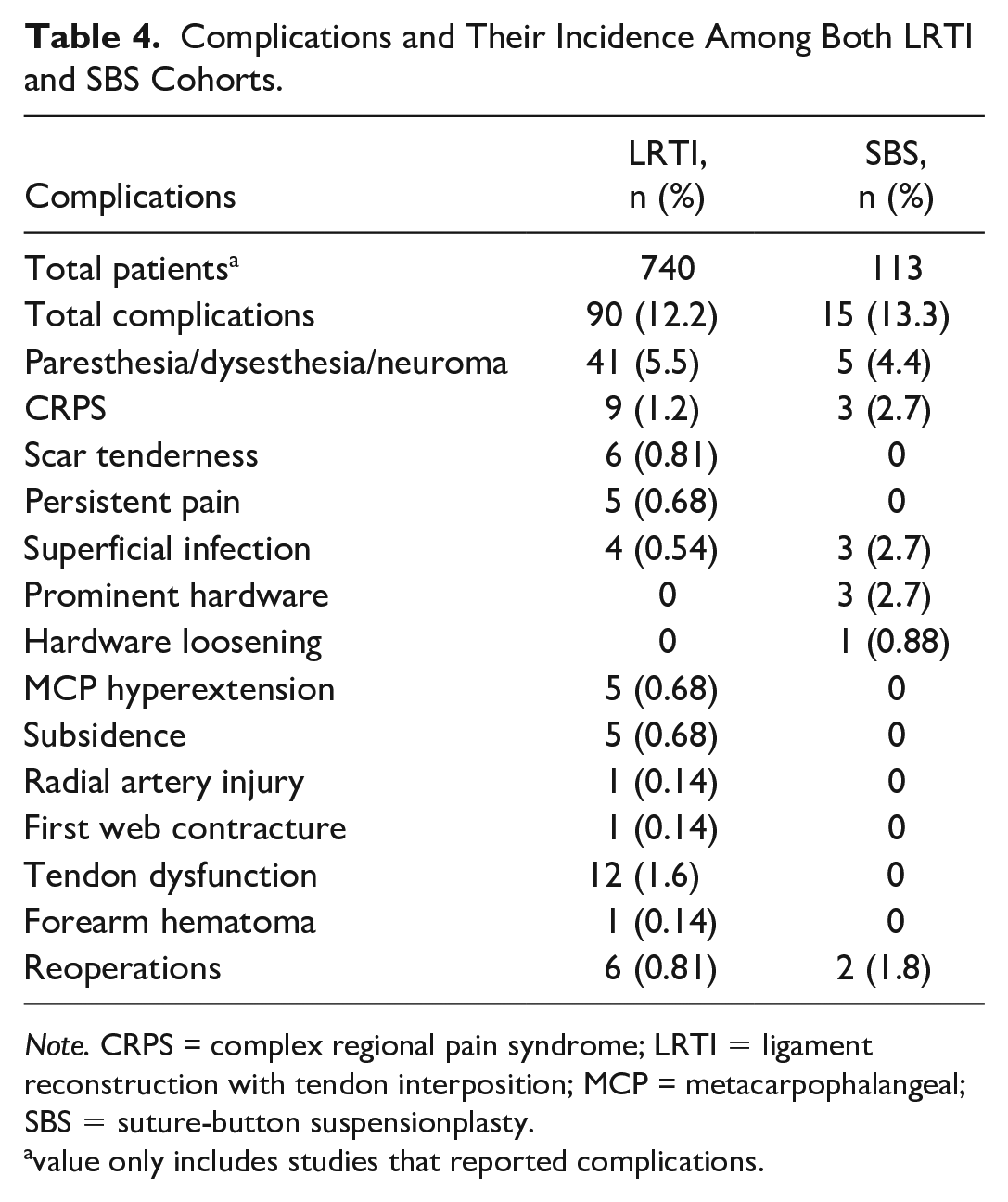
Note. CRPS = complex regional pain syndrome; LRTI = ligament reconstruction with tendon interposition; MCP = metacarpophalangeal;SBS = suture-button suspensionplasty.
value only includes studies that reported complications.
Discussion
This systematic review supports the authors’ hypotheses that both techniques (LRTI and SBS) lead to improvements in short-term patient-reported outcomes—primarily DASH and QuickDASH scores. Objective outcomes, such as grip strength or key pinch strength, were found to have less predictable, but similar, improvement after each technique. Finally, complication rates were similar between the 2 techniques. Prior systematic reviews looking at multiple available techniques have suggested that no current surgical technique holds superiority. 34 In fact, there is nearly universal improvement of subjective symptoms, patient-reported outcomes, and functional improvement despite varying techiques. 2 The “gold standard” surgical technique for treatment of first CMC joint osteoarthritis remains the classical LRTI. However, newer techniques allow for improved biomechanical stability16,35,36 in the early postoperative period, which allows for earlier mobilization and faster recovery, in addition to removing the need for external fixation using k-wires (to protect the graft in the immediate postoperative period) and potential decreased morbidity by negating the need for a tendon autograft harvest.
This is the first systematic review specifically investigating the outcomes of SBS for first CMC joint osteoarthritis. Standardized patient-reported outcomes, such as DASH and QuickDASH scores, are becoming more widely used and allow for more “true” comparison of subjective improvement between techniques. Of the 19 LRTI studies included in this review that reported patient-reported outcomes using either DASH or QuickDASH, 91% (10 of 11 studies) for DASH and 88% (7 of 8 studies) for QuickDASH demonstrated an improvement that met the previously defined MCID, 10-points and 15-points, respectively. 24 Of the 5 SBS studies included, 50% (1 of 2 studies) and 100% (3 of 3 studies) demonstrated improvement that met MCID for DASH and QuickDASH scores, respectively. Given there is a plethora of subjective assessment measures, a strength of this systematic review was specifically including studies that used the DASH and QuickDASH questionnaires as a measure of subjective physical function. Prior systematic reviews have only briefly touched on DASH scores and have reported variability in regard to patient-reported outcome measures due to lack of standardization and selective reporting.13,34,37 Strength (grip and pinch) was shown to generally increase following both LRTI and SBS, but there was great heterogeneity in the reported change post operatively. Overall, suture suspensionplasty led to more consistent improvement in both grip and pinch strength, but the small sample size and lower quality evidence of SBS studies makes this conclusion difficult to generalize. Prior systematic reviews have failed to demonstrate that any treatment method for first CMC joint osteoarthritis results in superior outcomes in regard to strength.13,34 Outcomes such as strength and range of motion are important tools to measure patient function, but are included in standardized outcome scores, such as the DASH and QuickDASH.
This study suggests an equivalent complication rate between the 2 techniques, while prior systematic reviews have reported a higher complication rates (as much as 20%) for LRTI, including scar sensitivity, superficial radial neuritis, and tendonitis—when compared with trapeziectomy alone (approximately 10%).13,37 The 2 re-operations within the SBS group in our study were due to hardware complications (i.e. hardware prominence or loosening), while the 6 re-operations for the LRTI group were performed for FCR tendon pathology, metacarpophalangeal hyperextension, and thumb subsidence. The low rate of revision surgery following LRTI (0.8%) and SBS (1.8%) could be to the high retrospective nature of included studies, whereas higher revision rates are seen when studies directly investigate the frequency of revision surgery, especially when it is done prospectively.38,39 Thumb subsidence postoperatively has been shown to be limited biomechanically with use of an artificial suspension using a button.16,35,36
Limitations of this systematic review include the predominantly lower level (i.e. retrospective, III and IV) evidence included for review leading to an increased risk for bias. This is especially true for the SBS studies, where 5 of the 6 included studies were level-IV evidence, and 1 was level-III evidence. The authors chose to utilize only DASH and QuickDASH scores as the patient-reported outcomes used for comparison. However, this potentially prevents the inclusion of higher quality studies that may have utilized other patient-reported outcome measures. Moreover, follow-up times were generally short and not all studies clearly labeled at what postoperative timepoint outcome scores and strength measurements were recorded. This also excludes the present study from commenting on long-term complications associated with each procedure. Although LRTI remains the “gold standard” for the treatment of first CMC joint osteoarthritis, recent evidence suggests no advantage when compared simple trapeziectomy alone. 40 This study does not compare the potential economic implications of using either LRTI or SBS, which include operative time and the effect that maintenance of FCR has on grip strength. No studies have evaluated the economic implications, including the hardware or implants utilized for either LRTI or SBS—or the cost of re-operation and time off work. True randomized controlled trials for first CMC joint osteoarthritis are made difficult by potential unblinding due to surgical scars.
Although both LRTI and SBS seemed to provide improved short-term patient-reported functional improvement and objective strength, there was significant heterogeneity within the included studies and those studies discussing SBS were of lower quality evidence than those of LRTI. Thus, to truly delineate whether a difference exists between these 2 techniques for the treatment of first CMC joint arthritis, larger prospectively designed studies of high-quality evidence are necessary.
Supplemental Material
sj-pdf-1-han-10.1177_15589447211043217 – Supplemental material for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis
Supplemental material, sj-pdf-1-han-10.1177_15589447211043217 for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis by Austin E. Wininger, Erin I. Orozco, Alex Han, Matthew B. Burn and Shari R. Liberman in HAND
Supplemental Material
sj-pdf-2-han-10.1177_15589447211043217 – Supplemental material for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis
Supplemental material, sj-pdf-2-han-10.1177_15589447211043217 for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis by Austin E. Wininger, Erin I. Orozco, Alex Han, Matthew B. Burn and Shari R. Liberman in HAND
Supplemental Material
sj-pdf-3-han-10.1177_15589447211043217 – Supplemental material for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis
Supplemental material, sj-pdf-3-han-10.1177_15589447211043217 for Systematic Comparison of Ligament Reconstruction With Tendon Interposition and Suture-Button Suspensionplasty for Trapeziometacarpal Osteoarthritis by Austin E. Wininger, Erin I. Orozco, Alex Han, Matthew B. Burn and Shari R. Liberman in HAND
Footnotes
Supplemental material is available in the online version of the article.
Author’s Contributions
A.E.W., E.I.O., A.H., M.B.B., and S.R.L. contributed to the research design and data interpretation. A.E.W., E.I.O., and A.H. contributed to the literature search, data collection, and data analysis. A.E.W., E.I.O., and A.H. drafted the manuscript. A.E.W., S.R.L., and M.B.B. critically revised the manuscript. All authors read and approved the final manuscript.
Ethical Approval
This study did not require review by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
No patients were recruited for this study and therefore informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AEW, EIO, and AH declare they have no conflicts of interests. MBB does not have disclosures relevant to the current study but does report Medinc of Texas: educational support; Arthrex Inc: educational support. SRL does not have disclosures relevant to the current study but does report Acumed: educational support.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Consent for Publication
All authors have agreed to the publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.