
Abstract
Background:
The goal of zone II flexor tendon surgery is to perform a repair with sufficient strength to withstand the forces encountered during rehabilitation. Postoperative rerupture and adhesion formation may lead to reoperation. This study aimed to determine the factors associated with reoperation after primary zone II flexor tendon repair.
Methods:
In this retrospective case series, a total of 252 fingers in 201 patients underwent zone II flexor tendon repair. A medical record review was performed to collect data regarding patient demographics, injury and treatment characteristics and postoperative complications including reoperation. Reoperation was defined as any unplanned surgical procedure performed after initial flexor tendon repair.
Results:
There were 49 fingers (19%) in 42 patients that underwent reoperation at a median of 5.5 (interquartile range: 2.8-7.9) months. Older age, workers’ compensation, and a Kessler-type repair of the flexor digitorum profundus were independently associated with reoperation.
Conclusions:
In vitro studies suggest that Kessler-type repairs are inferior compared with other suture configurations. Our study demonstrates a clinical correlation to these biomechanical studies. Our results suggest that Kessler-type repairs are inferior compared with non-Kessler-type repairs, due to postoperative complications requiring secondary surgeries.
Introduction
The goal of zone II flexor tendon surgery is to perform a repair with sufficient strength to withstand the forces encountered during rehabilitation. Reoperation rates are higher in zone II than in other flexor tendon zones1,2 and have been reported to occur in about 6% of patients. 3 Older age, workers’ compensation, and concomitant nerve repair are associated with reoperation in patients after flexor tendon repair in any zone. 4 In zone II injuries, older age, injury severity, and smoking have been associated with inferior results.1,5,6 Studies specifically assessing reoperation after zone II flexor tendon repair are uncommon, but nonsharp mechanisms of injury, such as saw and crush injuries, and combined flexor digitorum profundus (FDP)/flexor digitorum superficialis (FDS) injuries, may be associated with reoperation, 6 which may consist of either surgery for tendon rupture or tenolysis.
In vitro studies demonstrate that suture configuration,7,8 suture size,9,10 the use of an epitendinous suture, 11 and the number of core strands12-14 are related to repair strength. In an in vivo canine model, epitendinous repair increased repair strength by 22%. 11 Other biomechanical analyses have shown that a 10-strand repair has increased ultimate load failure by 106% compared with a 4-strand repair. 14 However, few clinical studies demonstrate a clear difference between suture repair techniques in actual practice. Therefore, the goal of this study was to investigate what factors are associated with reoperation and how evaluation of reoperation should incorporate factors related to biomechanical strength due to the risk of rerupture. We tested the null hypothesis that there are no factors associated with reoperation after primary zone II flexor tendon repair.
Methods
After institutional review board approval (IRB), we retrospectively identified adult patients who underwent primary zone II flexor tendon repair from January 2000 through September 2016 at 3 urban academic medical centers using Current Procedural Terminology codes (Appendix A). All records were verified through medical chart review (n = 663). Zone II flexor tendon injuries were identified if the term “zone II” was used in the medical chart or if the tendon injury was described to be in between the insertion of the FDS and the A1 pulley in the operative reports. We excluded patients with injuries of the thumb (n = 123), isolated FDP or FDS injury (n = 83), associated phalangeal fractures (n = 73), non–zone II injuries (n = 48), unknown FDP repair technique (n = 36), finger amputation without replantation (n = 23), a mangled hand (n = 21), miscoding (n = 20), partial flexor tendon laceration (n = 10), finger amputation with replantation (n = 9), initial surgery at an outside hospital (n = 8), nonacute repair (n = 7), and pregnancy (which was a mandatory IRB exclusion) (n = 1). Our final study cohort included 252 fingers in 201 patients with zone II flexor tendon injuries.
This was a retrospective case series with a level of evidence of III. We reviewed medical records to collect data regarding patient demographics, injury and treatment characteristics, and postoperative complications including reoperation. Reoperation was defined as any unplanned surgical procedure performed on the same finger after the initial flexor tendon repair. A Kessler-type repair technique was recorded when the specific term “Kessler” was used in the operative note, and a Modified Becker repair technique was recorded when the term “Modified Becker” or “MGH repair” was used in the operative note. Other repairs included Tajima or cruciate techniques. Flexor tendon injuries defined as “sharp” included injuries caused by knifes or glass, whereas the “nonsharp” injuries included saw and crush injuries. Rupture was based on determination by the treating physician or imaging reported in the medical chart. Finger stiffness was recorded if this was reported in the physician or occupational therapy notes. Follow-up time was defined as the time from surgery to the last clinical visit recorded in the medical charts.
Study Population
We identified 252 fingers in 201 patients that underwent repair of flexor tendon zone II injuries with a median follow-up of 2.0 (interquartile range [IQR]: 0.24-6.8) years. The median age was 32 (IQR: 25-45) years, and 141 patients (70%) were men (Table 1). The mechanism of injury included sharp injury (n = 204, 84%) and nonsharp injury (n = 39, 16%), such as saw and crush injuries. The dominant hand was injured in 87 patients (49%). The index finger was injured in 64 fingers (25%), the middle finger in 49 fingers (19%), the ring finger in 59 fingers (23%), and the small finger in 80 fingers (32%). There were 137 patients (68%) with 1 injured finger, 47 patients (23%) with 2 injured fingers, and 17 patients (8.5%) with more than 2 injured fingers (Table 2). Digital artery injuries were present in 45 fingers (18%), of which 17 fingers (37%) were dysvascular, and 31 digital arteries (69%) were repaired. Digital nerve injury was present in 157 fingers (62%), and 155 of these fingers (99%) underwent nerve repair (Table 3).
Association Between Patient Characteristics and Reoperation After Zone II Flexor Tendon Repair.
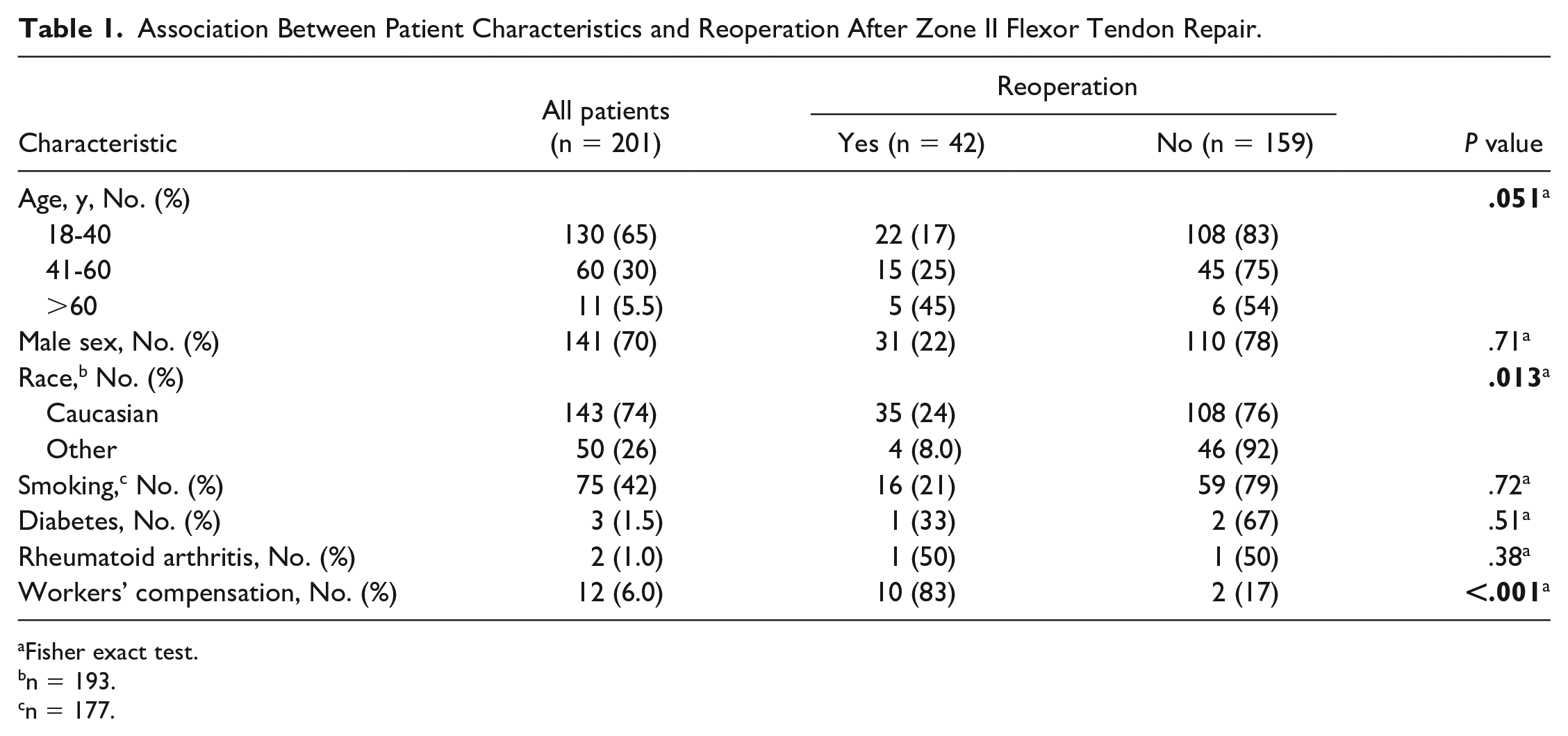
Fisher exact test.
n = 193.
n = 177.
Association Between Injury Characteristics and Reoperation After Zone II Flexor Tendon Repair.
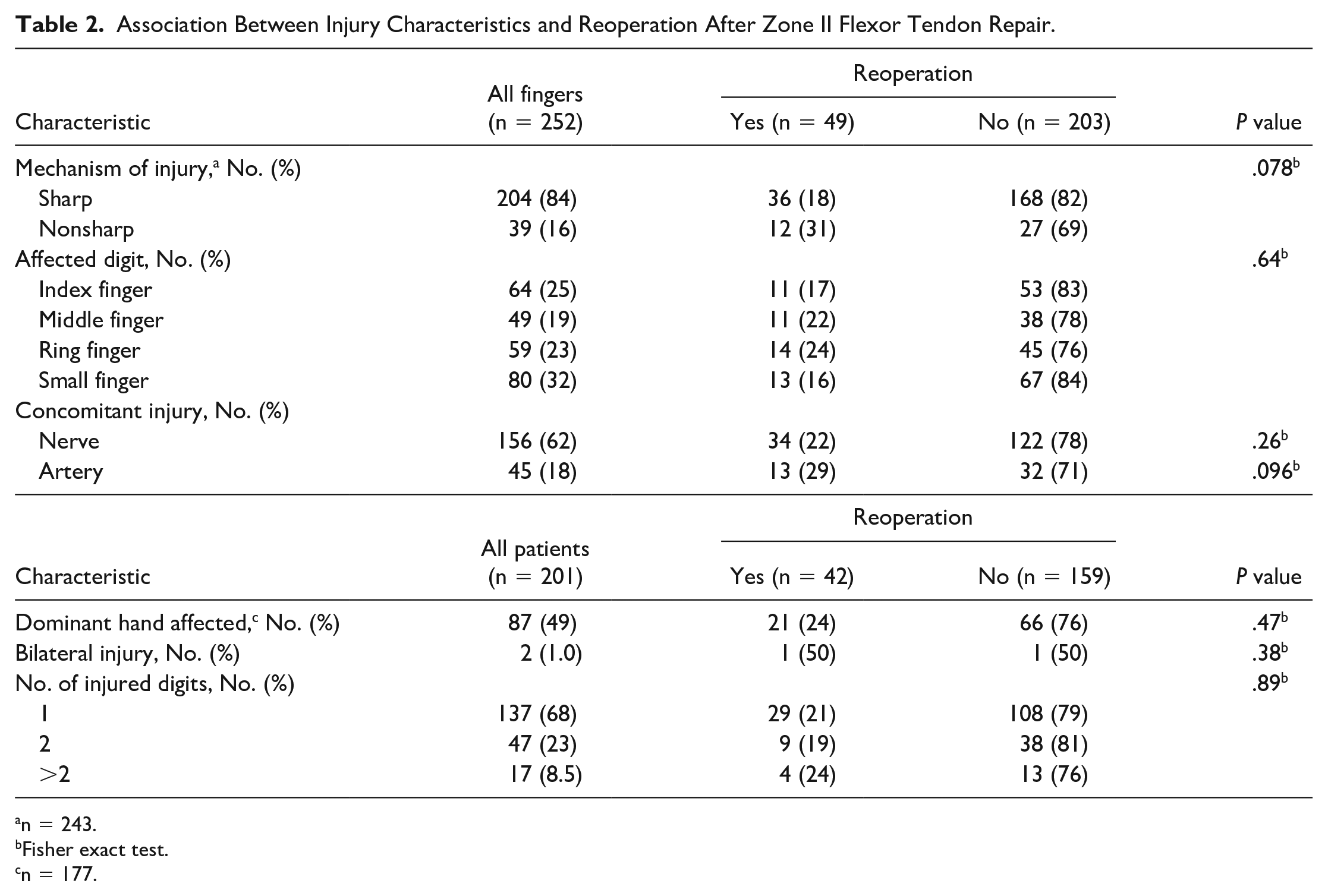
n = 243.
Fisher exact test.
n = 177.
Association Between Surgery Characteristics and Reoperation After Zone II Flexor Tendon Repair.
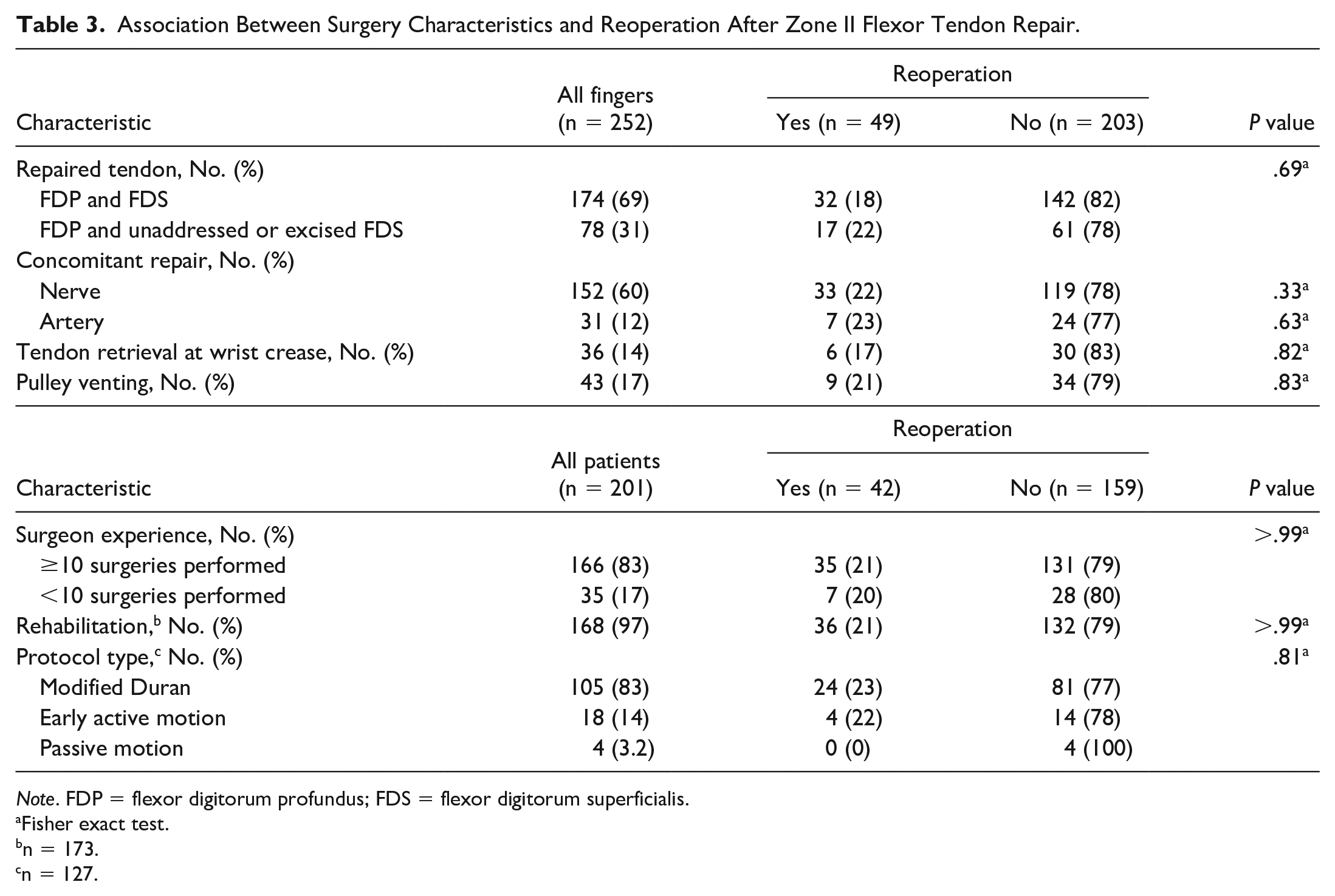
Note. FDP = flexor digitorum profundus; FDS = flexor digitorum superficialis.
Fisher exact test.
n = 173.
n = 127.
Surgical Procedure
Flexor tendon repairs were performed by 55 surgeons in this cohort, but most of the repairs (52%) were performed by 7 surgeons who each performed 10 or more repairs. The median time from injury to initial surgery was 4.0 (IQR: 1.0-7.0) days. Flexor tendon repair techniques included Kessler, Modified Becker, cruciate, or other repair techniques (Appendix B). Both FDP and FDS tendons were repaired in 174 fingers (69%), the FDS was excised in 41 fingers (16%), and the FDS was unaddressed in 37 fingers (15%). For the FDP tendon, a Modified Kessler repair was most commonly performed (n = 194, 77%), followed by the Modified Becker repair (n = 22, 8.7%). An epitendinous suture was used in 195 (77%) patients.
Most FDP repairs were 4-strand repairs (n = 215, 86%), followed by 2-strand (n = 8, 3.2%) or more than 4-strand repairs (n = 28, 11%). Braided suture materials were used in 198 (90%) fingers and monofilament suture materials in 22 (10%) fingers. A 3-0 suture was the most commonly used suture size (n = 140, 63%), followed by a 4-0 suture or smaller size (n = 74, 33%), a 2-0 suture (n = 8, 3.6%), or a combination of 2-0 and 3-0 sutures (n = 1, 0.45%) (Table 4). Nerve allografts were not used in any of the repairs; in 3 nerve repairs (2.0%), a nerve conduit was used as a nerve wrap at the neurorrhaphy; and in 1 repair (0.66%), a nerve conduit was used to bridge a nerve gap of 1.5 mm. Pulley venting was reported in 43 fingers (17%), of which the A2 pulley was vented in 21 fingers (49%), the A4 pulley was vented in 10 fingers (23%), and pulley venting of both A2 and A4 pulleys was reported in 11 fingers (26%). In 1 patient, venting was reported, but the specific pulley was not documented. All A2 pulleys were partially vented; in 1 case it was not clearly described whether it was partial or complete. Rehabilitation protocols were documented in 127 patients (63%). This included the modified Duran protocol (n = 105, 83%), early active motion (n = 18, 14%) or passive motion protocol (n = 4, 3.2%). 15 In 74 patients, the exact rehabilitation protocol was unclear from the records.
Surgery Characteristics of Zone II FDP Repair.
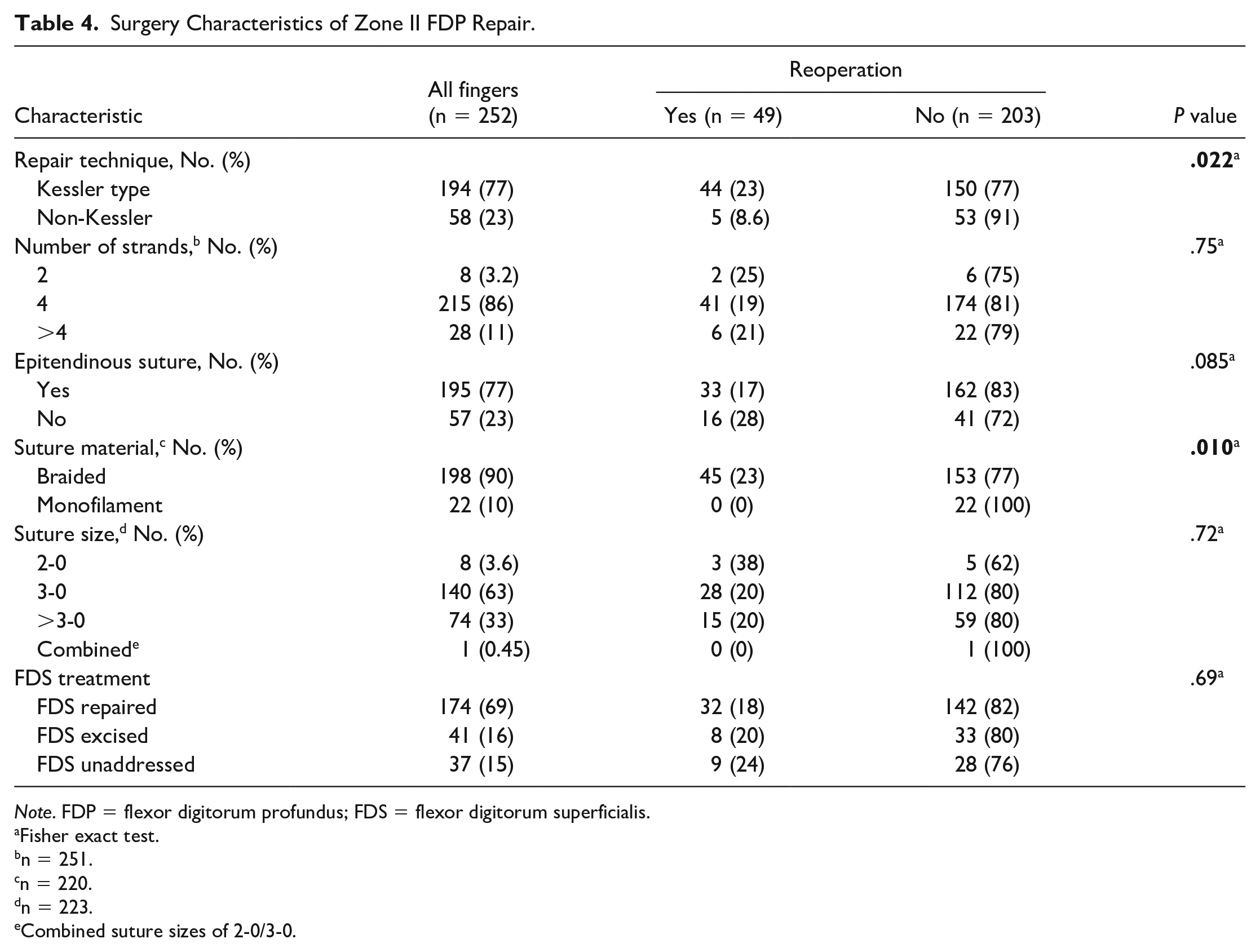
Note. FDP = flexor digitorum profundus; FDS = flexor digitorum superficialis.
Fisher exact test.
n = 251.
n = 220.
n = 223.
Combined suture sizes of 2-0/3-0.
Statistical Analysis
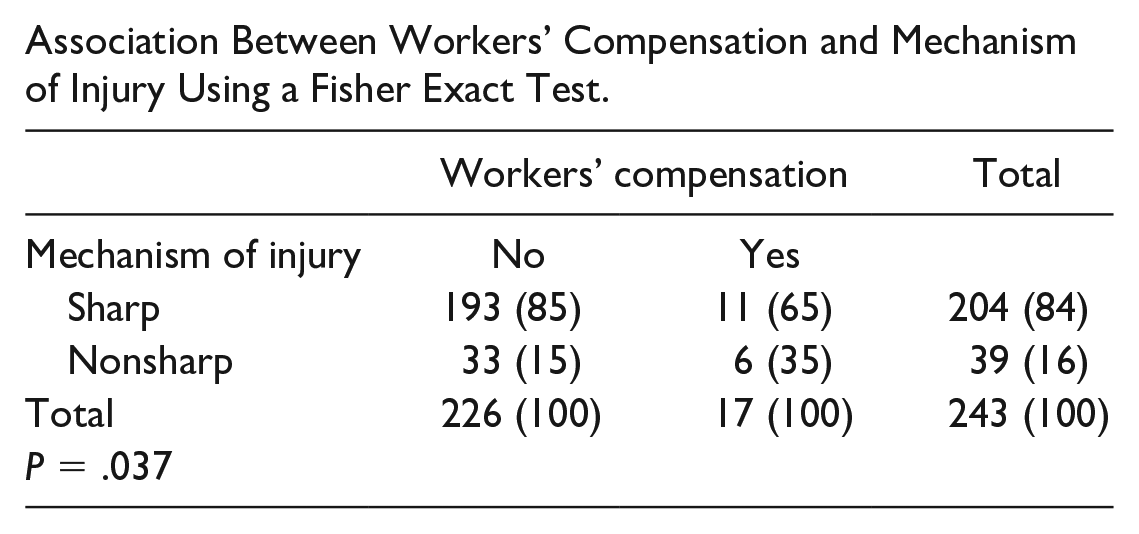
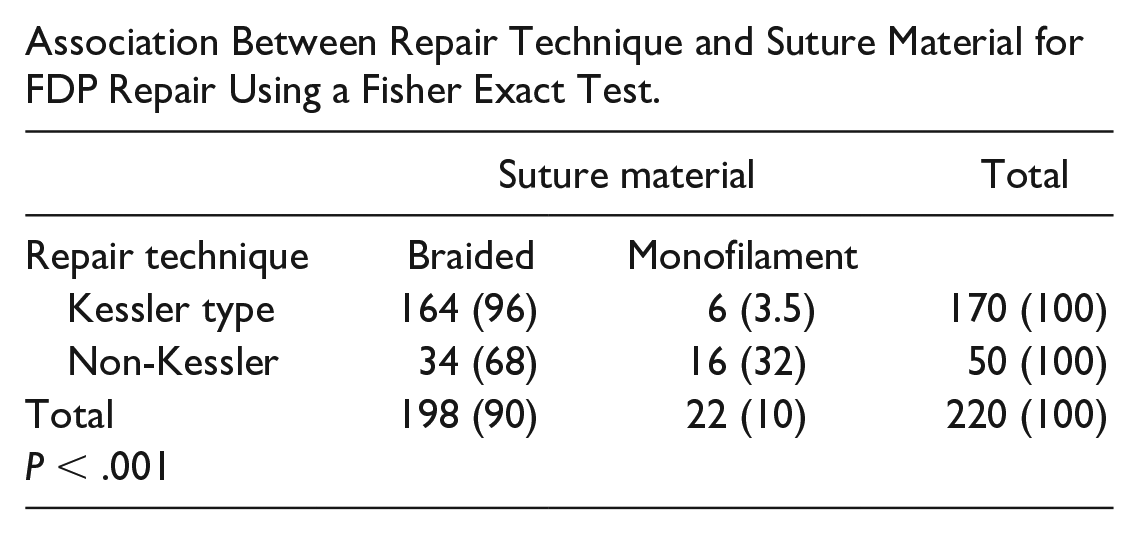
Categorical variables were presented as absolute values and percentages. Continuous variables were presented as median and IQR. To evaluate the factors associated with reoperation, a bivariate analysis was performed using the Fisher exact test for categorical variables and the Mann-Whitney U test for nonparametric outcomes. Unknown repair techniques were included in the group of non-Kessler repair techniques in analysis. All explanatory variables that had a value of P < .1 in the bivariate analysis were included in a multivariable logistic regression model using generalized estimated equation to correct for confounding. This method was used to correct unique patients with multiple injured fingers. We performed a multivariable model for all patient and injury characteristics meeting the criteria mentioned above, including the FDP repair technique. We did not include mechanism of injury as this was significantly correlated with workers’ compensation (P = .037) (Appendix C). Suture material was not included in the multivariable analysis as this was significantly correlated with the repair technique for FDP (P < .001) (Appendix D). Race was included in the bivariate analysis (Table 1); however, it was not included in the multivariable analysis because the distribution of patients was primarily Caucasian, and the association was likely to be spurious because of our regional demographics. A value of P < .05 was considered statistically significant for all tests. We used STATA 13.0 (StataCorp, College Station, Texas) to perform all analyses.
Results
There were 49 fingers (19%) in 42 patients (21%) that underwent reoperation at a median of 5.5 (IQR: 2.8-7.9) months. Indications for reoperation included stiffness or adhesion (n = 35, 71%), suspected tendon rupture (n = 12, 25%), and infection (n = 2, 4.1%) (Table 5). In addition, there were 7 fingers (2.8%) that underwent a third operation following index repair at a median of 6.2 (IQR: 0.9-7.1) months. Two fingers (0.79%) underwent a fourth operation following index repair at a median of 10.7 (IQR: 1.4-20.0) months. Complications in patients who did not undergo a reoperation included finger stiffness (n = 32, 17%), clinical rerupture (n = 5, 2.5%), and infection (n = 4, 2.2 %) (Table 6).
Indications for Reoperation.

Complications Without Reoperation.
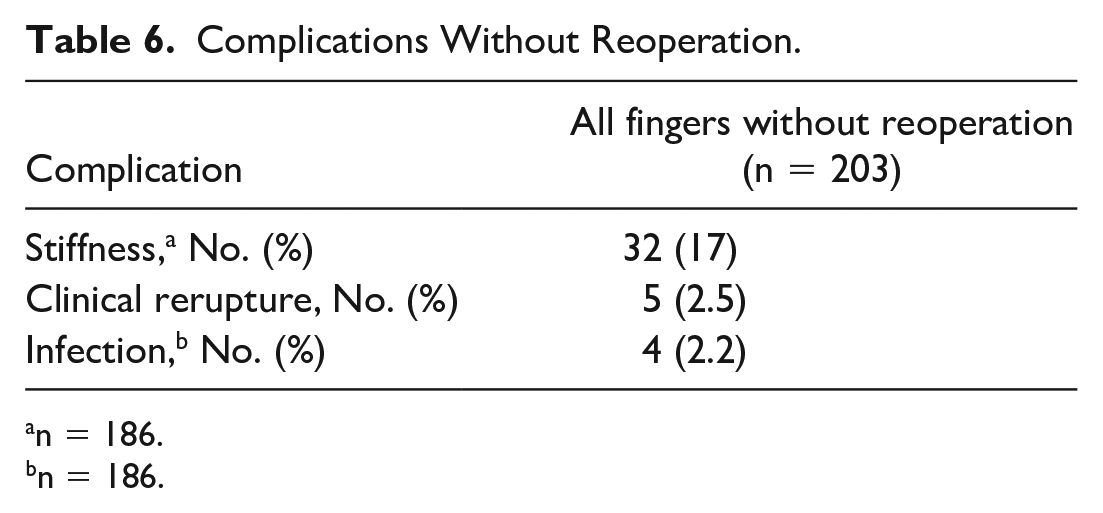
n = 186.
n = 186.
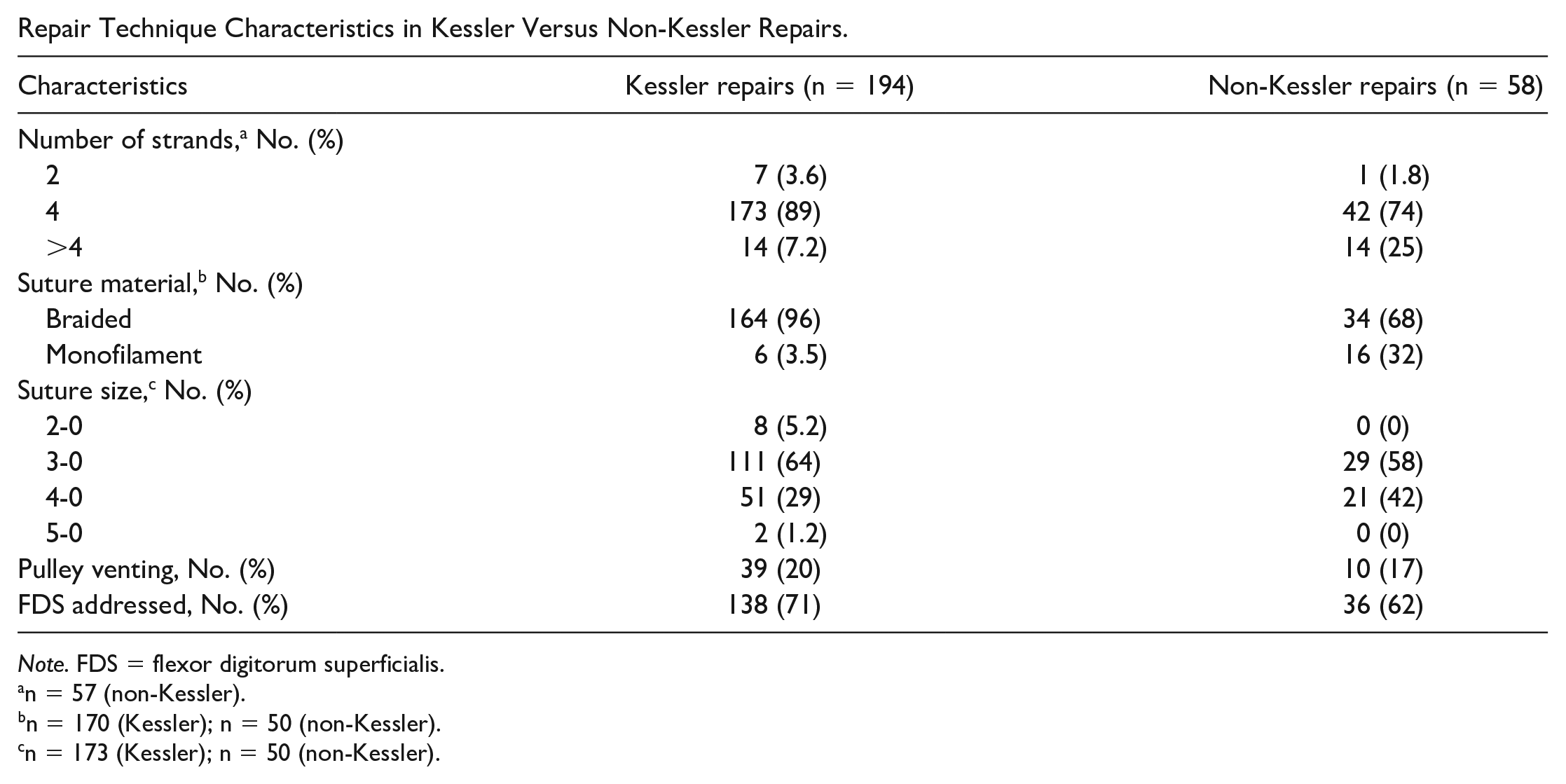
In this study, most Kessler repairs of the FDP tendon consisted of a 4-strand repair (n = 173, 89%) with an intratendinous knot and a braided (n = 164, 96%) 3-0 suture (n = 111, 64%). The FDS was addressed in most of the Kessler repairs (n = 138, 71%). The non-Kessler repairs also mostly consisted of a 4-strand repair (n = 42, 74%), and more often a braided (n = 34, 68%) and 3-0 (n = 29, 58%) or 4-0 (n = 21, 42%) suture was used. The FDS was addressed in 36 (63%) non-Kessler repairs (Appendix G).
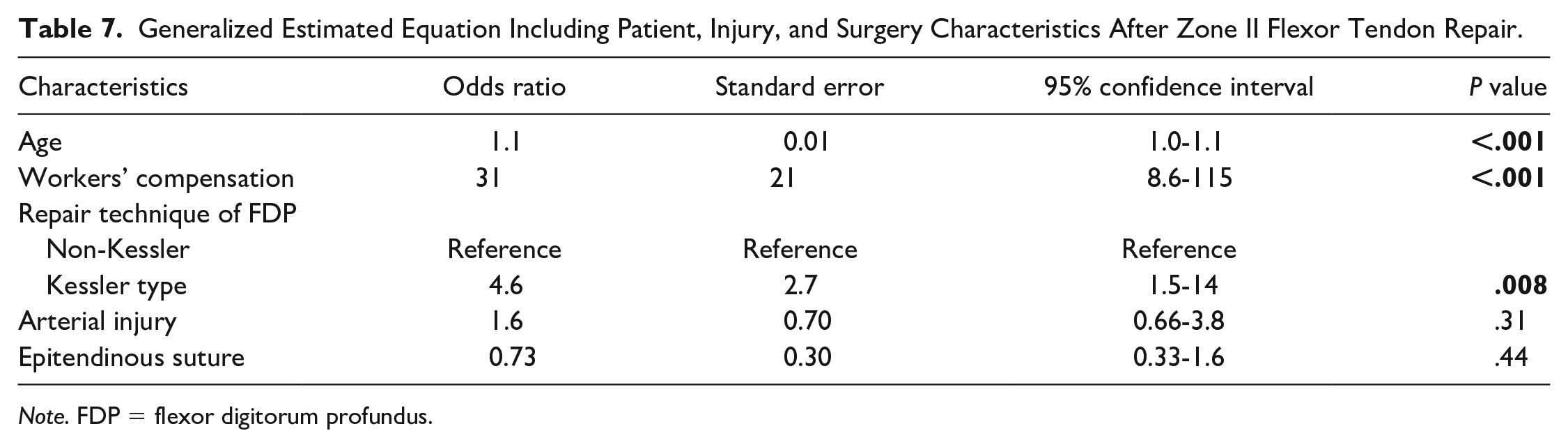
Evaluation for predictors of reoperation after flexor tendon repair showed older age (odds ratio [OR], 1.1; 95% confidence interval [CI], 1.0-1.1; P < .001) was independently associated with reoperation. Furthermore, insurance through workers’ compensation (OR, 31; 95% CI, 8.6-115; P < .001) and the use of a Kessler-type repair for the FDP tendon (OR, 4.6; CI, 1.5-14; P = .008) compared with non-Kessler repair techniques were independently associated with reoperation [Table 7].
Generalized Estimated Equation Including Patient, Injury, and Surgery Characteristics After Zone II Flexor Tendon Repair.
Note. FDP = flexor digitorum profundus.
Discussion
In this study, we analyzed factors associated with reoperation after primary zone II flexor tendon repair in 201 patients with 252 injured fingers. Reoperation occurred in 19% of fingers, of which 71% were for stiffness and suspected adhesions. Overall, the suspected tendon rerupture rate was 7.1%, of which 67% underwent reoperation. Patient factors that were independently associated with reoperation were older age and workers’ compensation. Furthermore, the use of a Kessler repair technique when repairing the FDP was associated with higher reoperation rates compared with non-Kessler repair techniques.
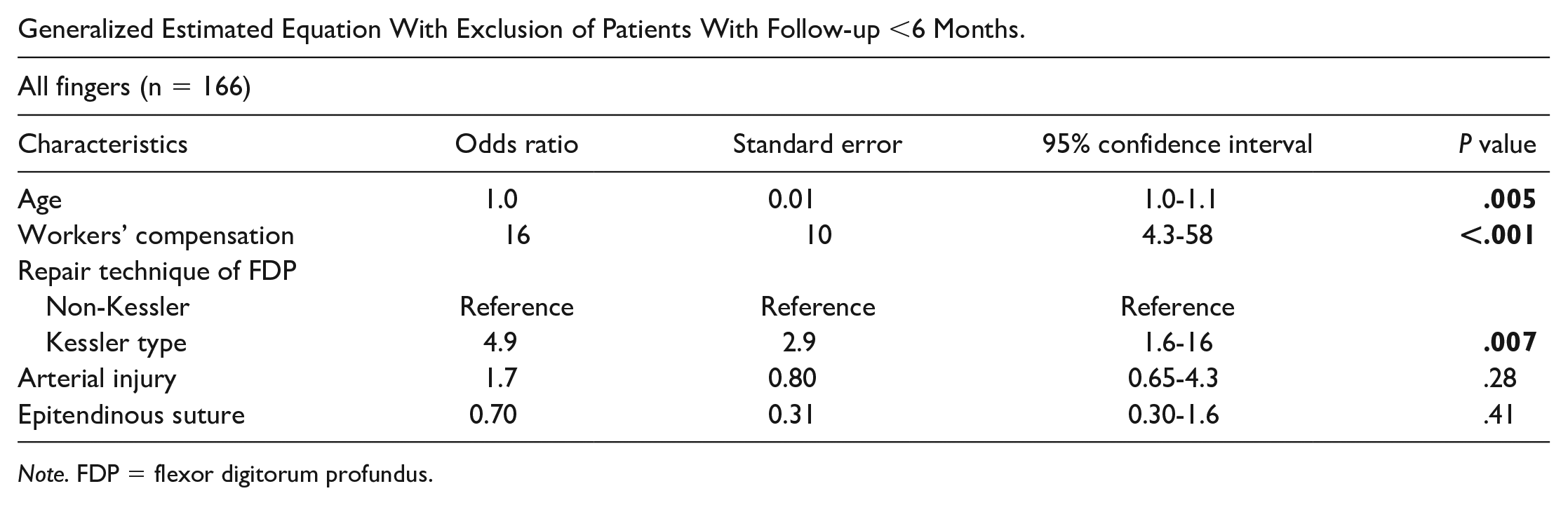
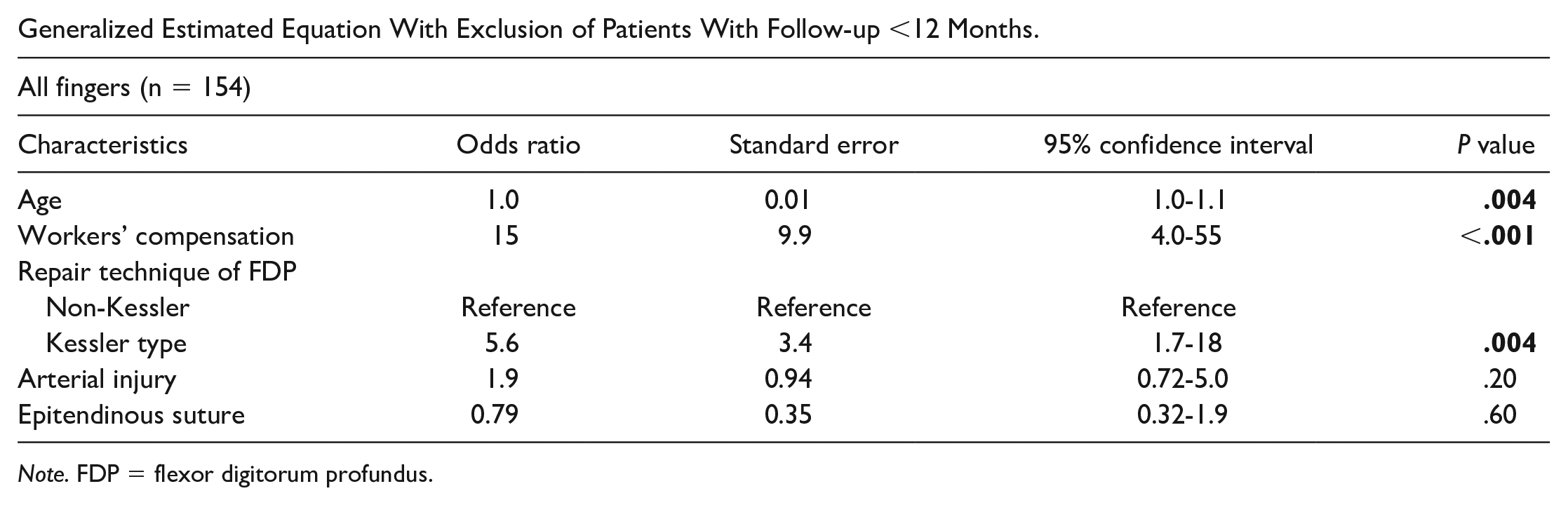
This study should be interpreted in the context of its strengths and limitations. First, the retrospective nature of this study depends on correct coding to identify cases. Second, all surgical procedures included in this study were performed at teaching hospitals where some repairs are performed by fellows. Despite the large number of operating surgeons, we tested this variable and found reoperation rates were similar for surgeons who performed less than 10 surgeries and surgeons who performed 10 or more surgeries (P > .99) (Table 3). Third, to undergo reoperation was a clinical decision made at the discretion of the operating surgeon. There were no predetermined guidelines for reoperation, and it is unclear why some patients with restricted range of motion did not undergo surgery. Presumably, the impact on daily activities was limited, or risk of surgery outweighed potential benefit. Fourth, the follow-up was less than 3 months for 25% of the patients. However, excluding the patients with a follow-up less than 6 or 12 months yielded similar results (Appendices E and F). Fifth, the type of rehabilitation protocol and the duration of and adherence to postoperative rehabilitation are confounding factors. The type of rehabilitation protocol, however, was not associated with reoperation (Table 3). Sixth, the ratio of patients in the Kessler-type and non-Kessler-type repairs lies around 4 to 1. Due to our clinical study design and the given standard with the Kessler-type repairs, it was not possible to reach a 1-to-1 ratio. Finally, it should be taken into consideration that the Kessler repair technique is an eponymous term that may be used differently among surgeons. All these variants include an extratendinous link component in 4 corners with intratendinous longitudinal and transverse components; however, the type of link component, number of strands, and number of knots may vary among surgeons. 16 By definition, a Modified Kessler involves a loop extratendinous link component with 1 intratendinous knot at the junction of the tendon ends, whereas a Modified Becker consists of crisscrossing running sutures with 2 extratendinous knots. In this study, most Kessler repairs of the FDP tendon consisted of a 4-strand repair (n = 173, 89%) with an intratendinous knot and a braided (n = 164, 96%) 3-0 suture (n = 111, 64%). Univariate analyses showed the use of braided suture material was associated with reoperation. However, as explained in Appendix D, suture material was significantly correlated with the FDP repair technique and was therefore not included in the multivariate analysis. The FDS was addressed in most of the Kessler repairs (n = 138, 71%). The non-Kessler repairs also mostly consisted of a 4-strand repair (n = 42, 74%), and more often a braided (n = 34, 68%) and 3-0 (n = 29, 58%) or 4-0 (n = 21, 42%) suture was used. The FDS was addressed in 36 (63%) non-Kessler repairs (Appendix G).
The reoperation rate of 19% identified in this study is consistent with other studies. Reoperation rates range from 11% to 29%.5,6,17 However, it is higher than the reoperation rate of 6% reported in a meta-analysis of Dy et al. 3 The tenolysis rate of 14% in this study is higher than that in previous studies 3 ; however, the rerupture repair rate of 7.1% is in line with prior findings.3,4 Surgery for adhesions and stiffness varies among surgeons and patients as this surgery is relatively discretionary and may explain this variation.
We found that a Kessler-type repair for the FDP was associated with higher reoperation rates compared with non-Kessler repair techniques. Most non-Kessler repairs consisted of Modified Becker repair and cruciate repairs; however, the description in the operative note of some repair techniques was not detailed enough to classify the repair. The indications for reoperation of FDP tendons that were repaired with a Kessler technique were adhesions (n = 30, 68%), reruptures (n = 12, 27%), and infection (n = 2, 4.6%), which is similar to the distribution of indications for reoperation in the entire cohort (Table 5). We found that the FDS was addressed in 138 (71%) patients who underwent a Kessler repair and in 215 (85%) patients of the total cohort. Our analysis showed that leaving the injured FDS unaddressed was not associated with higher reoperation rates, compared with excision of the injured FDS (Table 3). When comparing the postoperative rehabilitation programs, we found that the modified Duran protocol was used most often in the Kessler repairs (n = 114, 89%). The early active motion protocol was used more significantly in the non-Kessler repairs (n = 13, 37%) compared with the Kessler repairs (n = 10, 7.8%). We theorize that patients who undergo Kessler-type repairs may not advance with rehabilitation as rapidly as other biomechanically stronger repairs and undergo reoperation more frequently.
Time zero tensile strength of a Kessler-type repair is inferior to that of the Modified Becker repair and cruciate repair in multiple in vitro biomechanical studies.1,18,19 In an in vitro porcine model, modified Kessler repair had inferior tensile strength and the highest rate of suture pull-out failure compared with a Modified Becker, Adelaide, or Lahey repair. 18 Peltz et al also found that gapping and rotation occurred more often in a Kessler repair. 20 Our findings are in contrast to those of Dy et al who found modified Kessler repair was associated with lower reoperation rates. 3 Our study had a larger cohort than most of the studies included in the meta-analysis by Dy et al and is less prone to small sample effects and reporting biases.
In this study, the use of an epitendinous suture was not associated with higher reoperation. Despite the suggestion that use of an epitendinous suture may lead to increased bulk at the repair site causing adhesion formation, 21 other studies have shown that the use of an epitendinous suture increases tensile strength,22,23 creating a strong repair, which corresponds to our results. Furthermore, the mechanism of injury was not significantly associated with reoperation. However, we found that a tearing mechanism of injury and workers’ compensation were significantly correlated (Appendix C). Although the dysvacular fingers (n = 17, 6.7%) were splinted 1 to 2 weeks before starting rehabilitation, no association with reoperation was found in these fingers. Finally, race was found to be significantly associated with reoperation in the bivariate analysis (Table 1), which is most likely spurious as a result of small sample phenomenon.
In this study, patients with insurance through workers’ compensation had higher reoperation rates, which is similar to other studies.4,24 Workers’ compensation cases have slower return to work, 25 greater degree of disability, 26 and worse outcome after orthopedic surgical procedures.27-29 This may be related to the fact that the aim of the insurer is to allow the patient to return to work as quick as possible. Furthermore, we found that patients with workers’ compensation suffered saw and crush injuries more frequently, a proxy for higher injury severity. In addition, we found that age was associated with reoperation. 30 Younger patients with an age of 18 to 40 years had a reoperation rate of 17%. The rate of reoperation was 25% in patients who were 41 to 60 years old. Of the patients who were 60 years or older, 45% underwent reoperation. This is consistent with the retrospective database study by Dy et al. 4 With increased age, digital stiffness may be more common, and the capacity for tendon healing may be diminished, which may affect the rate of reoperation.31,32
In conclusion, in vitro studies suggest that Kessler-type repairs are biomechanically inferior compared with other suture configurations. Our study demonstrates a clinical correlation to these data in that Kessler-type repair was associated with higher reoperation rates. Our study showed that older age, workers’ compensation, and a Kessler-type repair for the FDP tendon were significantly associated with reoperation. Our results suggest that Kessler-type repairs are inferior compared with non-Kessler-type repairs, due to postoperative complications requiring secondary surgeries.
Footnotes
Appendix A
Appendix B
Other Repair Techniques.
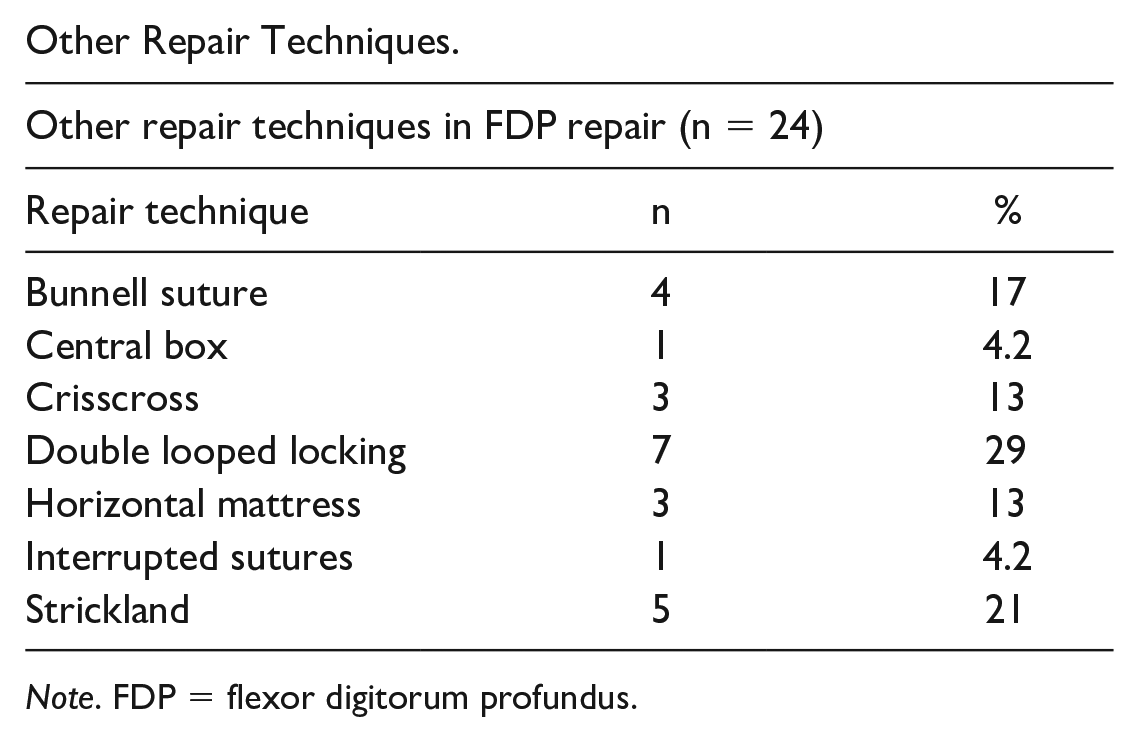
| Other repair techniques in FDP repair (n = 24) | ||
|---|---|---|
| Repair technique | n | % |
| Bunnell suture | 4 | 17 |
| Central box | 1 | 4.2 |
| Crisscross | 3 | 13 |
| Double looped locking | 7 | 29 |
| Horizontal mattress | 3 | 13 |
| Interrupted sutures | 1 | 4.2 |
| Strickland | 5 | 21 |
Note. FDP = flexor digitorum profundus.
Appendix C
Association Between Workers’ Compensation and Mechanism of Injury Using a Fisher Exact Test.
| Workers’ compensation | Total | ||
|---|---|---|---|
| Mechanism of injury | No | Yes | |
| Sharp | 193 (85) | 11 (65) | 204 (84) |
| Nonsharp | 33 (15) | 6 (35) | 39 (16) |
| Total | 226 (100) | 17 (100) | 243 (100) |
| P = .037 | |||
Appendix D
Association Between Repair Technique and Suture Material for FDP Repair Using a Fisher Exact Test.
| Suture material | Total | ||
|---|---|---|---|
| Repair technique | Braided | Monofilament | |
| Kessler type | 164 (96) | 6 (3.5) | 170 (100) |
| Non-Kessler | 34 (68) | 16 (32) | 50 (100) |
| Total | 198 (90) | 22 (10) | 220 (100) |
| P < .001 | |||
Appendix E
Generalized Estimated Equation With Exclusion of Patients With Follow-up <6 Months.
| All fingers (n = 166) | ||||
|---|---|---|---|---|
| Characteristics | Odds ratio | Standard error | 95% confidence interval | P value |
| Age | 1.0 | 0.01 | 1.0-1.1 |
|
| Workers’ compensation | 16 | 10 | 4.3-58 |
|
| Repair technique of FDP | ||||
| Non-Kessler | Reference | Reference | Reference | |
| Kessler type | 4.9 | 2.9 | 1.6-16 |
|
| Arterial injury | 1.7 | 0.80 | 0.65-4.3 | .28 |
| Epitendinous suture | 0.70 | 0.31 | 0.30-1.6 | .41 |
Note. FDP = flexor digitorum profundus.
Appendix F
Generalized Estimated Equation With Exclusion of Patients With Follow-up <12 Months.
| All fingers (n = 154) | ||||
|---|---|---|---|---|
| Characteristics | Odds ratio | Standard error | 95% confidence interval | P value |
| Age | 1.0 | 0.01 | 1.0-1.1 |
|
| Workers’ compensation | 15 | 9.9 | 4.0-55 |
|
| Repair technique of FDP | ||||
| Non-Kessler | Reference | Reference | Reference | |
| Kessler type | 5.6 | 3.4 | 1.7-18 |
|
| Arterial injury | 1.9 | 0.94 | 0.72-5.0 | .20 |
| Epitendinous suture | 0.79 | 0.35 | 0.32-1.9 | .60 |
Note. FDP = flexor digitorum profundus.
Appendix G
Repair Technique Characteristics in Kessler Versus Non-Kessler Repairs.
| Characteristics | Kessler repairs (n = 194) | Non-Kessler repairs (n = 58) |
|---|---|---|
| Number of strands, a No. (%) | ||
| 2 | 7 (3.6) | 1 (1.8) |
| 4 | 173 (89) | 42 (74) |
| >4 | 14 (7.2) | 14 (25) |
| Suture material, b No. (%) | ||
| Braided | 164 (96) | 34 (68) |
| Monofilament | 6 (3.5) | 16 (32) |
| Suture size, c No. (%) | ||
| 2-0 | 8 (5.2) | 0 (0) |
| 3-0 | 111 (64) | 29 (58) |
| 4-0 | 51 (29) | 21 (42) |
| 5-0 | 2 (1.2) | 0 (0) |
| Pulley venting, No. (%) | 39 (20) | 10 (17) |
| FDS addressed, No. (%) | 138 (71) | 36 (62) |
Note. FDS = flexor digitorum superficialis.
n = 57 (non-Kessler).
n = 170 (Kessler); n = 50 (non-Kessler).
n = 173 (Kessler); n = 50 (non-Kessler).
Authors’ Note
This work was presented at American Society for Surgery of the Hand (ASSH) Annual Meeting 2019 in Las Vegas, Nevada.
Author Contributions
J.L. and N.C.C. were involved in study design. L.L.B. and J.L. were involved in data assembly. L.L.B., J.L., F.W., and N.C.C. were involved in data analysis. L.L.B., J.L., F.W., K.R.E., and N.C.C. were involved in writing the initial draft. L.L.B., J.L., F.W., K.R.E., and N.C.C. were involved in final approval of the manuscript.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
No identifying information is published in this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.C.C. is a consultant for Miami Device Solutions. K.R.E. is a consultant for AxoGen and Integra. L.L.B., J.L., and F.W. declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Jesse B. Jupiter Fund.