
Abstract
Background:
Multiple techniques for the repair of flexor tendon injuries in zone 1 have been proposed over time. While pull-out suture techniques and bone anchor seem to be stronger than internal suture techniques, they are associated with a higher complication rate. We therefore developed an alternative internal suture repair with similar biomechanical stability to those of pull-out sutures and bone anchors.
Methods:
Twenty porcine distal phalanges and deep flexor tendons were randomized to 2 groups of 10 each. The tendons were transsected at the level of the distal interphalangeal joint. In group 1, repairs were performed with a well-established intraosseous suture repair and in group 2 with our new multistrand technique. The repairs were biomechanically tested with linear distraction until failure.
Results:
We recorded a significantly higher 2-mm gap force (2GF)—and thus higher stability—of the repairs in group 1 in comparison to group 2. With a 2GF of more than 50 N, our suture technique allows for a modern early active motion rehabilitation protocol. Breakage of the suture construct occurred at random places in the repair in both groups. No pull-outs were noted.
Conclusions:
This study presents a strong transosseous multistrand repair technique for flexor tendon repair in zone 1 that is simple and fast to perform and should have enough strength to withstand early active motion rehabilitation.
Introduction
In the past decades, a plethora of new techniques for flexor tendon repairs in zone 1 have been proposed.1-4 In general, these methods can be grouped into 2 categories: external and internal suture repairs. 5 External techniques represent the traditional repair methods with placement of the suture knot on the surface of the distal phalanx (fingertip, pulp, or nail plate), usually stabilized by an underlay (“button”). The pull-out button suture and its modifications have long been the standard for tendon-to-bone repairs.6-8 However, these techniques are often associated with complications, namely local skin irritation up to pressure sores, pulp dystrophy, soft tissue or bone infections, as well as nail deformities in the long term.2,4,9-11 To avoid these problems, purely internal repair methods have been invented. In recent years, bone anchors have been promoted in particular as a simple and fast alternative to pull-out sutures. 12 Despite advances in material and design, these devices still have their limitations. Several studies and reviews reported relevant complications, such as foreign body reactions, dorsal protrusion, intra-articular placement, and pull-out from the bone . Apart from that, the implants are often too large for the distal phalanx (eg, in up to 97% of little fingers in 1 study), and poor bone quality in elderly patients or a fracture at the distal phalanx are seen as additional limitations. Apart from the (now quite popular) techniques that use bone anchors, 12 these factors have led to the emergence of anchorless “all-inside” repairs in the 2000s.4,13
Our department has long used the technique described by Langer et al, 14 which in itself is a technical modification of the transverse intraosseous loop technique (TILT) repair by Tripathi et al. 15 However, even when reinforced with an epitendinous suture, 16 the repair does not allow for rehabilitation with a modern early active motion (EAM) protocol due to a relatively low 2-mm gap force (2GF) and thus insufficient stability. The 2GF is defined as the force needed to create a 2-mm gap at the repair site, with a higher value denoting a more stable repair. Clinical studies have shown that a gap formation greater than 2 mm is associated with a higher failure rate of the suture repair and worse clinical outcomes. 17 Furthermore, the TILT repair can be laborious necessitating 3 cannulas to pass the suture through and an additional free needle (Figure 1a-e). We therefore developed an alternative internal suture repair with 4 strands, the “transosseous internal four strand” (TIFS) technique. The aim of this study is to evaluate the biomechanical properties of our new technique in comparison to the modified Langer technique (mLT).
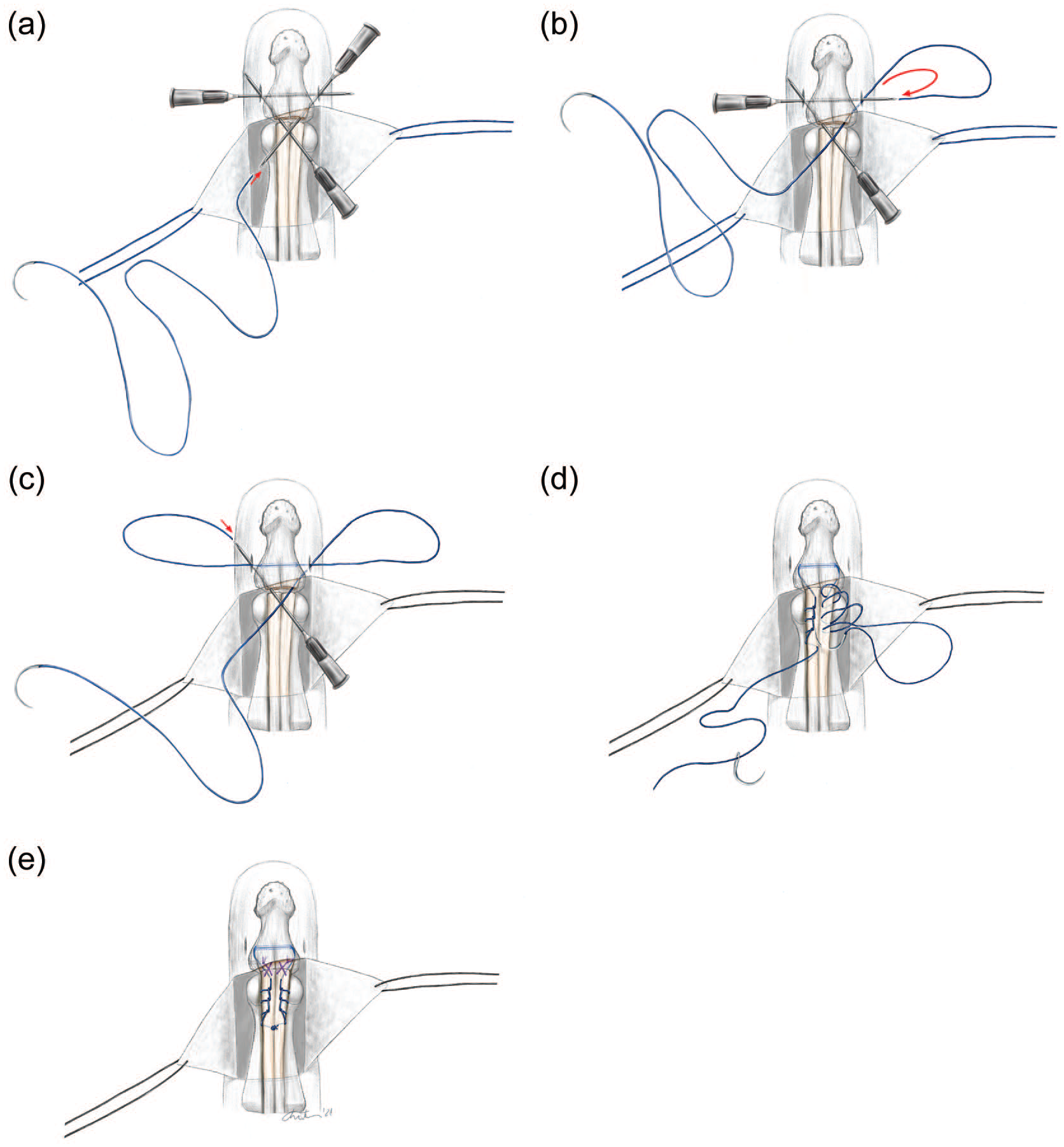
Illustration of the TILT technique by Tripathi with its technical modification described by Langer and further modification by the addition of an epitendinous repair (mod. Langer technique).
Materials and Methods
The distal phalanges and deep flexor tendons of the feet of freshly butchered domestic pigs were freed from surrounding soft tissue and exarticulated through the distal interphalangeal joint. This model was chosen for the similar dimensions and biomechanical properties of porcine and human flexor tendons.18-20 The pigs’ claws were randomly assigned to 2 groups, 10 each (n = 10 per group, 20 in total). The tendons were transsected at the level of the interphalangeal joint, which left an about 2- to 3-mm tendon stump attached to the claw. The always present sesamoid bone of the pig distal interphalangeal joint was removed. The tendons of the mLT group were repaired in the previously described modified TILT/Langer technique using USP 3-0 Polydioxanon (PDS-II; Ethicon Inc, Bridgewater, New Jersey) suture and an USP 5-0 monofilament polydioxanon suture (PDS-II, RB-1 needle; Ethicon Inc) for the epitendinous repair 16 (Figure 1a-e). In biomechanical testing, no significant difference for ultimate failure load (UFL) and 2GF was found when performing the repair with braided or nonbraided suture material. We therefore decided to use a monofilament suture for the modified TILT/Langer repair in our experiment as proposed by Tripathi in his original description.
Transosseous Internal Four Strand Technique
The tendons of the TIFS group were repaired in the TIFS technique as illustrated in Figure 2a-f: An 18G hypodermic needle is manually bored transversely through the base of the distal phalanx. The looped end of a USP 4-0 braided pseudomonofilament nylon suture (Supramid Loop; Resorba Medical GmbH, Nuremberg, Germany) is passed through the hypodermic needle (Figure 2a). Afterwards, the hypodemic needle can be removed pulling the suture loop through the bone channel. Then, the looped end of a second Supramid suture is passed through and around the loop in place, creating a sliding knot (Figure 2b). The knot has to be pulled tight and placed to the center of the bone channel. The needles on each end are then passed through the periosteum and (if present) the remaining distal tendon stump. The proximal tendon stump is then fixed to the distal phalanx with a Kessler-like locking suture, positioning the knot between the 2 locking loops and tightening it to the distal stump with 4 square knots (Figure 2c). The repair is reinforced with 2 additional locking loops on each side as described by Krackow (Figure 2d), 21 gripping about 2 mm of tendon with each stitch. Finally, both needles are passed to the center and again tied with another 4-square knot (Figure 2e). In analogy to the mLT group, the repair is augmented with 2 figure-of-8 stitches (Figure 2f) with USP 5-0 monofilament polydioxanon suture (PDS-II, RB-1 needle; Ethicon Inc).
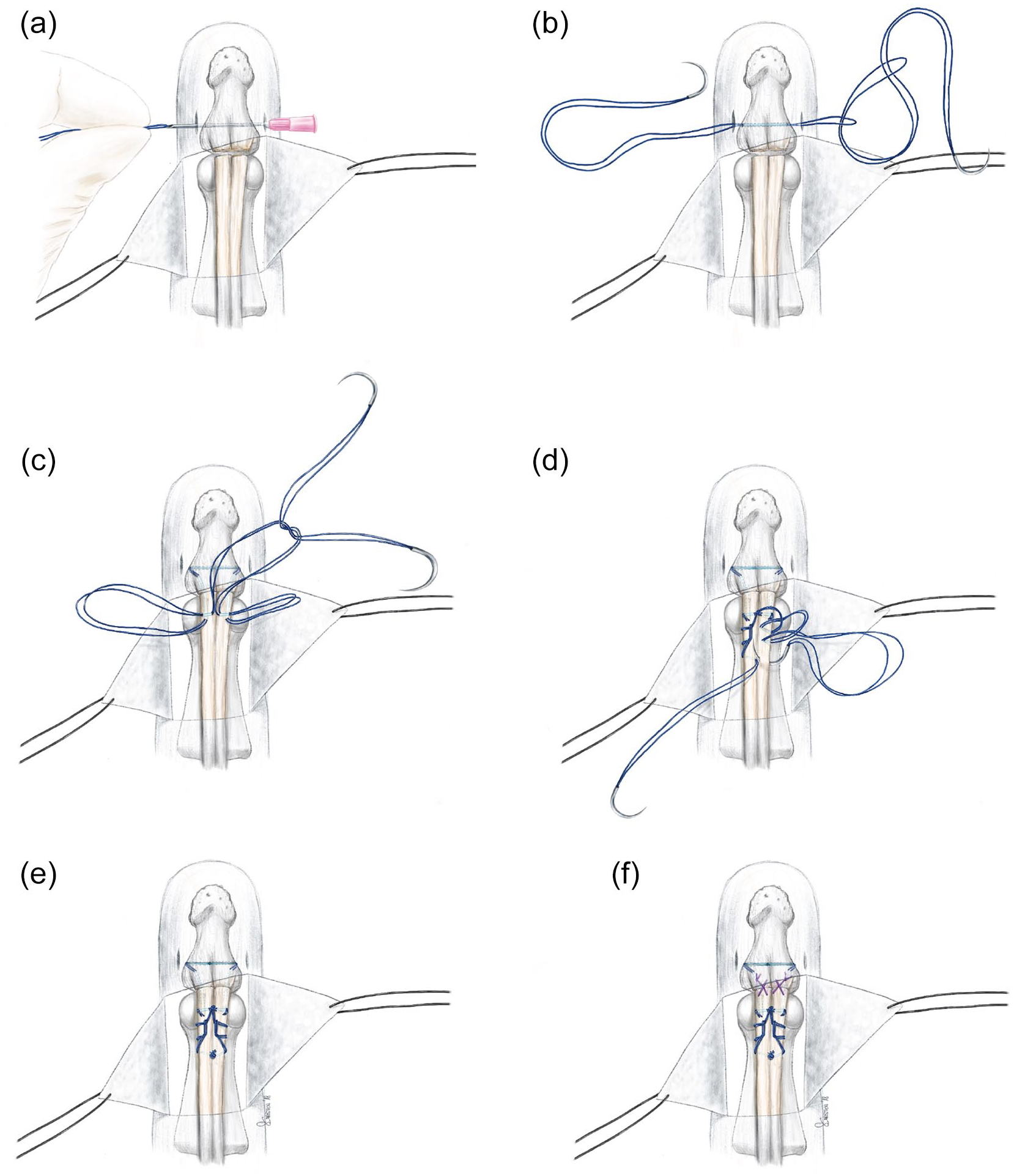
Illustration of the TIFS technique. (a, b) Threading of two 4-0 looped sutures through the distal phalanx; (c) Kessler stitch into the proximal stump; (d, e) reinforcement with 2 Krackow stitches per side; (f) Addition of 2 figure-of-8 stitches. TIFS = transosseous internal four strand.
Possible weak points (lock between the 2 loops, egress points from the bone, knots) were marked with a colored waterproof office supply marker (Edding 3000; Edding AG, Hamburg, Germany). For biomechanical testing, the specimens were fixed to a metal receptacle with a 2.5-mm K-Wire (Synthes AG, Solothurn, Switzerland) and placed in the top fixture of the material testing machine (Zwick-Roell, Ulm, Germany) with the free end clamped to the mobile sled of the machine at a length of 3 cm. The sutured tendons were tested with a standard protocol (1 N preload, distraction 1 cm/min) based on previous biomechanical studies for tendon suture repairs.22,23 Current tension force was recorded with control software for the testing machine (testXpert; Zwick-Roell) as well as correlated to images taken in 2 orthogonal planes at a rate of 10/second (Limess GmbH, Krefeld, Germany) with a millimeter scale placed next to the tendon for calibration.
For each reconstructed tendon, 2GF and UFL as well as place of rupture of the core suture were documented.
The data were tested for normality with the Shapiro-Wilk test. Descriptive statistics were calculated and the groups were compared with an independent sample t test.
Results
Descriptive statistics are shown in Table 1.
Descriptive Statistics.
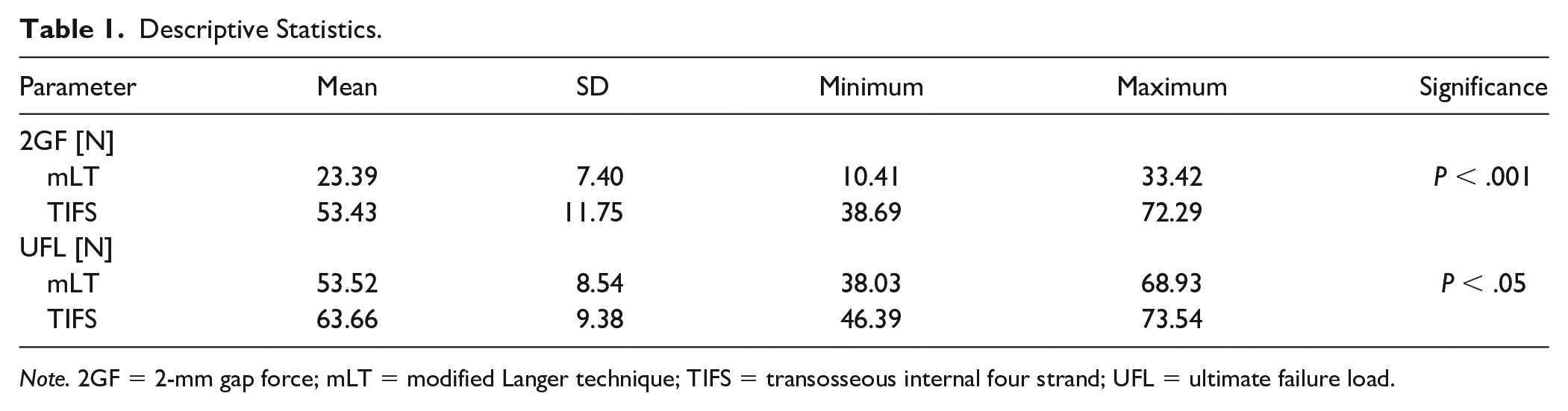
Note. 2GF = 2-mm gap force; mLT = modified Langer technique; TIFS = transosseous internal four strand; UFL = ultimate failure load.
The Shapiro-Wilk test revealed no significant difference (P > .05) between the distribution of the data and normal distribution.
While the 2GF was more than twice as high in the TIFS group, the difference in the UFL between the 2 groups was smaller although still significant. Independent sample t test revealed a significant difference between the groups for 2GF at P < .001 with a mean difference of 30.05 N and a significant difference of UFL at P < .05 with a mean difference of 10.15 N (Figure 3).
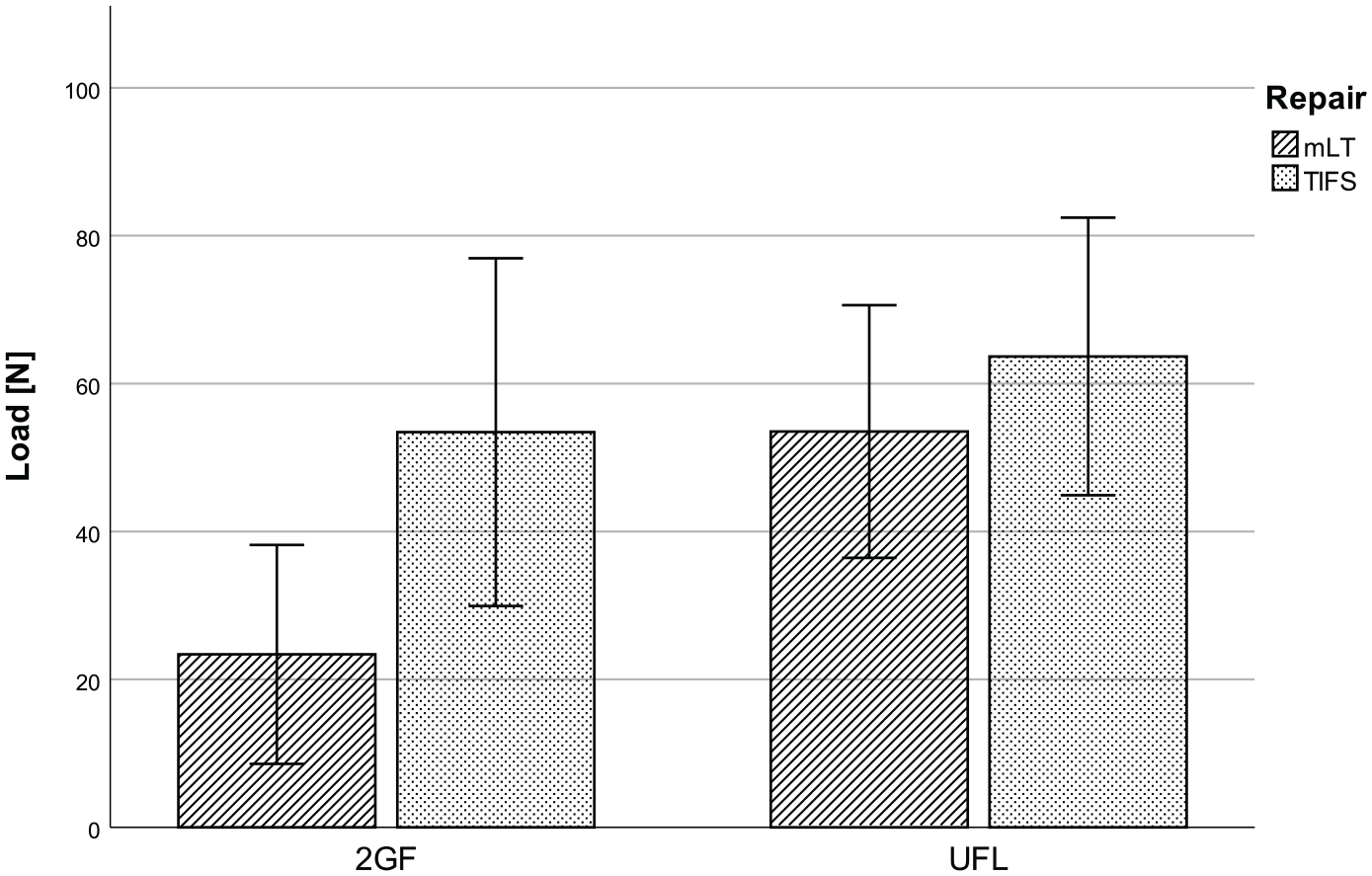
Comparison of 2GF and UFL (error bars ±2 SD). mLT = modified Langer technique; TIFS = transosseous internal four strand; 2GF = 2-mm gap force; UFL = ultimate failure load.
Comparing the 2GF against the expected load of 35 N for unresisted active flexion, 24 1-sample t test showed a statistically significantly lower mean for group 1 (difference: −11.61 N, P < .001) and a statistically significantly higher mean difference for group 2 (difference: 18.43 N, P < .001).
At UFL, all core sutures ruptured at random places in the repair gap. No loosening of the knot, rupture at the bone interface, or pull-outs (tendon or bone) were observed.
Discussion
The clinically relevant advantages of internal suture techniques for zone 1 tendon injuries have been discussed and proven by multiple studies.4,13 While entirely all-inside repairs rarely cause problems, external repair techniques are associated with a relatively high complication rate: Guinard et al 25 reported an infection rate of 13% and 1 case (4%) of digital pulp atrophy when using the Mantero technique (suture tied over a button at the fingertip). Kang et al 10 noticed an infection rate of 22% and nail deformities in 35% of patients when using the classic pull-out-button technique (button on the fingernail). Another study by Rigo and Rokkum 9 found 12 complications in 35 patients treated with a pull-out suture through the nail plate as opposed to no complications in 13 patients treated with the Tripathi TILT repair. 15 Four cases of the pull-out repair group required an operative revision, whereas none of the TILT repairs had to be reoperated.
Because internal suture repairs can be technically demanding, 26 refixation of the tendon with bone anchors has been proposed as a simple and straightforward approach. Over the last decades, a variety of repair methods with different bone anchor systems have been published, using 1 (eg, Skoff et al) 27 or 2 (eg, McCallister et al) 28 devices, sometimes even in combination with a pull-out suture (eg, Lee et al) 29 . Although bone anchor repairs are not associated with the typical soft tissue problems of pull-out sutures (6), they showed some device-related complications, including malplacement or secondary dislocation of the implant, infection, and foreign body reactions.30-32 In addition, bone anchors are not universally applicable: Apart from a potential injury to the growth plate in pediatric patients, the devices are sometimes oversized for the distal phalanx, in particular, in children and women. 33 Other contraindications for the use of bone implants are elderly patients (>75 years), osteoporosis, infections, or a concomitant fracture of the distal phalanx.34,35 Nevertheless, from the biomechanical point of view, recent bone anchor systems seem to be superior to traditional repair methods.12,36 In biomechanical testing, bone anchors revealed an UFL and a 2GF of up to 115 and 59 N, respectively, 12 while the highest UFL for pull-out sutures reported in the literature are 73.5 N. 37 Data about biomechanical properties of internal transosseous suture techniques however are scarce and the measured parameters are often not standardized.37-40
In this biomechanical experiment, we were able to show that our modification of the TILT/mLT repair greatly strengthens the repair. The 2 additional strands can be seen as main contributors for the overall strength. However, according to our observations during the first test runs, the Kessler-like locking suture (Fig. 2c) appeared to be crucial, first, for pulling the tendon tight to the bone and second for the avoidance of an early gapping.
The results of an in vivo study on canine flexor tendons by Gelberman et al 17 indicate that gapping at the repair site is the clinically most relevant parameter for tendon healing. They found that gap formation of more than 3 mm resulted in persistent weakness of the tendon and, as a consequence, a higher risk for rerupture. The tendon-bone interface seems even more susceptible to gap formation, especially in 2-strand repairs. 3 This makes the 2GF the most appropriate measure of static biomechanical testing for flexor tendon repairs. The results of several studies including 2-strand and multistrand suture techniques underline the superiority of the latter.3,38 Furthermore, avoiding gap formation in tendon-to-bone repairs seems even more important because healing of a flexor tendon in zone 1 is significantly slower than in zone 2. 3 Therefore, the mean 2GF of 53 N of the TIFS technique makes it comparable in strength to bone anchor techniques 12 and puts it well in the safe zone for EAM rehabilitation with respect to the expected load of up to 35 N for active, unresisted flexion previously described by Schuind et al. 24
However, our study has several limitations: It is a purely biomechanical ex vivo study in an animal model with a slightly different bone and tendon configuration. The model only applies a direct, linear force vector, and thus, is not able to replicate the complex vectors of the tendon-pulley relationship of the human hand in the clinical situation. Furthermore, the “one-shot” character of the linear distraction testing cannot predict the durability over the long run of tendon rehabilitation. Moreover, the clinical reliability and advantages of the TIFS technique have to be proven in a comparative and, ideally, randomized prospective in vivo study.
Conclusion
The TIFS technique is a simple and biomechanically strong all-inside transosseous suture technique for the repair of flexor tendon injuries in zone 1 or tendon-to-bone fixation of tendon grafts. In our biomechanical study, we were able to show that this multistrand repair has comparable mechanical properties as pull-out suture or bone anchor repairs.
Footnotes
Ethical Approval
No ethical approval was required, as no human specimens or data and no living animals or animals that were specifically killed for this study were used. All specimens were obtained from already butchered animals from a local butcher’s shop.
Statement of Human and Animal Rights
As per the regulations of the authors’ jurisdiction, ethical approval was not sought for this study because no animals were killed specifically for this study. All specimens were obtained from already butchered animals from a local butcher’s shop.
Statement of Informed Consent
Informed consent was not sought for the present as no human subjects were involved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No outside funding was obtained. The used materials were obtained with internal funds of the Department of Hand, Plastic and Reconstructive Surgery, Kantonsspital St. Gallen