
Abstract
Hirayama disease is a rare condition of cervical myelopathy. Its early identification and correction can optimize functional outcomes. However, late presentation and some more severe cases may be associated with loss of hand function. Among the cases described, there are no reports of nerve transfers for this condition. We presented the first case report of a Hirayama disease of isolated ulnar nerve impairment managed with nerve transfer. Electroneuromyography showed isolated preganglionic involvement of C7, C8, and T1, with no sensory changes. The patient underwent nerve transfer with anterior interosseous nerve to ulnar nerve supercharge end-to-side, recovering hand function in 7 months.
Introduction
Hirayama disease is a rare nonprogressive cervical myelopathy. It is also known as asymmetric juvenile muscular atrophy of unilateral upper extremity. It is caused by the anterior displacement of the posterior cervical dural sac on cervical flexion resulting in spinal cord compression and/or venous congestion. It is characterized by a pure motor focal amyotrophy in the C7, C8, and T1 myotomes leading to weakness and atrophy of intrinsic muscles of the hand. It differs from other motor neuron diseases due to its nonprogressive course.1,2
It is 3 to 7 times more common in men and the Asian population. There are few bilateral upper limb involvement cases and a tendency to affect the right upper limb, regardless of hand dominance.1-3
Among the few cases described in the literature, no studies are available regarding ulnar nerve impairment and its management. The other reports available are describing the condition and the management by a cervical collar on early diagnosis or spinal decompression.1-4 There is 1 study describing thumb opposition restoration by palmaris longus transfer. 5
It is the first case report of a patient with unilateral Hirayama disease presenting ulnar claw and symptoms managed by anterior interosseous nerve (AIN) to ulnar supercharge end-to-side (SETS) nerve transfer. There was severe atrophy and volume loss in the hypothenar mass leading to loss of hand function. The patient improved hand function and recovered the hand function in 7 months after the surgical procedure.
Case Report
A 24-year-old male patient, a right-handed accountant without comorbidities, presented with an ulnar claw for 10 years on the fifth finger and weakness in the left hand. He complained of abduction deformity of the fifth finger of his left hand since he was 14 years old, with weakness to adduct it.
He played handball in childhood when he began to have the perception of weakness in holding the ball. He had spasms in the fourth and fifth fingers that progressed to the fifth finger claw and atrophy of the hypothenar muscles for 5 years when the neurological condition stopped progressing.
However, he referred worsening in the cold 12 months ago, seeking orthopedic care. At the time of the evaluation, he featured complaints of “lameness,” weakness, and difficulty in sports activities, in addition to difficulty to extension and adduction of the fifth finger, with no sensory changes or other motor complaints in the upper limb.
There was substantial atrophy of the hypothenar musculature and fifth finger ulnar claw (Figure 1). There was an irregular tremor (so-called minipolymyoclonus) on the fifth finger extension.
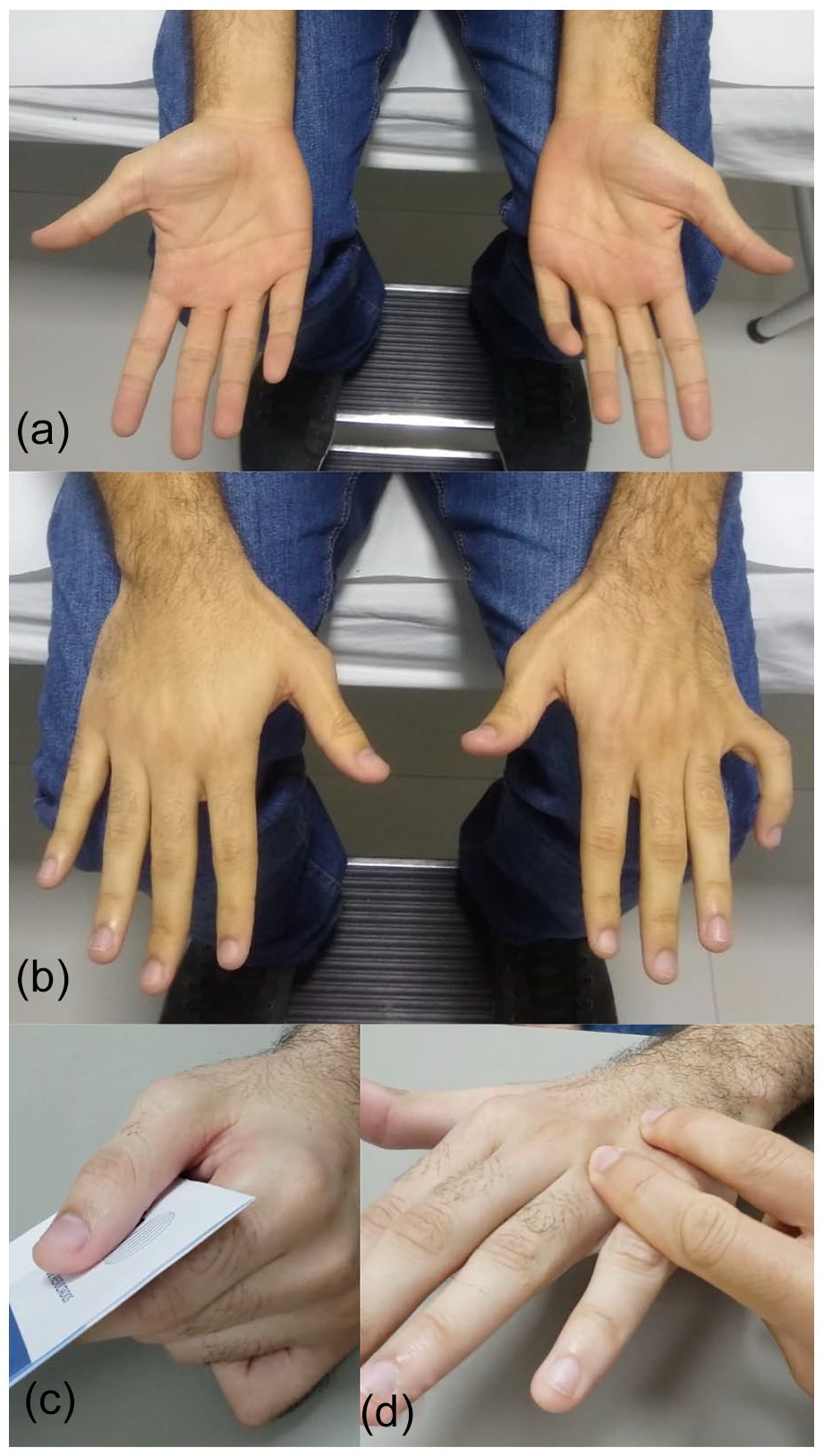
(a) Ulnar claw and a hypothenar atrophy, (b) dorsal interossei atrophy, (c) positive Froment sign, and (d) Bouvier maneuver correcting the ulnar claw.
The Medical Research Council evaluation found grade 2/5 to the abductor digiti minimi (ADM) muscle and the third and fourth lumbricals; grade 3/5 to the dorsal interosseous muscles, adductor pollicis, and flexor pollicis brevis; and grade 4/5 to the flexor carpi ulnaris and fourth-fifth digit flexor digitorum profundus. There were no changes in the brachioradialis, biceps, and triceps deep tendon reflexes. The Froment and Wartenberg signs were positive, and the Tinel and Scratch collapse tests were negatives. The 2-point discrimination test had no difference between both fifth fingers. There were no changes in sensitivity, no presence of palpable masses or cysts, and no vascular changes in the hand or abnormalities in the Allen test.
Preoperative grip strength measures by the JAMAR dynamometer were 25 kg for the left hand and 41.5 kg for the right hand, and the lateral pinch strength was 0 kg/f for the left hand and 10 kg/f for the right hand. The measurement by the goniometer showed a lack of 70° of proximal interphalangeal joint extension.
Electroneuromyography showed denervation of the ulnar nerve intrinsic muscles of the left hand, and the ulnar F waves were not detected. There were no sensory changes or other compression points. Isolated axonal motor preganglionic impairment of the C7, C8, and T1 of the anterior horn cells (Hirayama disease) was the principal diagnosis.
Dynamic magnetic resonance imaging (MRI) showed the distancing of the posterior dural sac on cervical flexion, increasing the posterior epidural space in the lower cervical segment. The entire length of the visible thoracic segment and the coexisting vascular structures in a posterior epidural situation effaced, determining effaced the posterior cerebrospinal fluid column and compressed on the spinal cord’s dorsal surface, from most evidently at the C5-C6 and C6-C7 levels. Decreased medullary thickness in the segment between C5 and T1, more evident at the level of C6-C7 and predominates in the left half (Figure 2). There were no abnormalities in blood tests and genetic tests, excluding other conditions.

Dynamic magnetic resonance image. (a) Sagittal and (b) (axial) showing the spinal cord at rest, and (c) sagittal and (d) axial showing posterior epidural enlargement space during the cervical flexion. Arrows showing the posterior epidural space and * showing C7.
The patient was submitted to surgical approach through access over the region of the forearm and wrist, including releasing the Guyon channel. The intraoperative electrostimulation confirmed the conductivity of the deep motor branch of the ulnar nerve. Thus, the AIN to ulnar nerve SETS transfer procedure was performed (Figure 3).
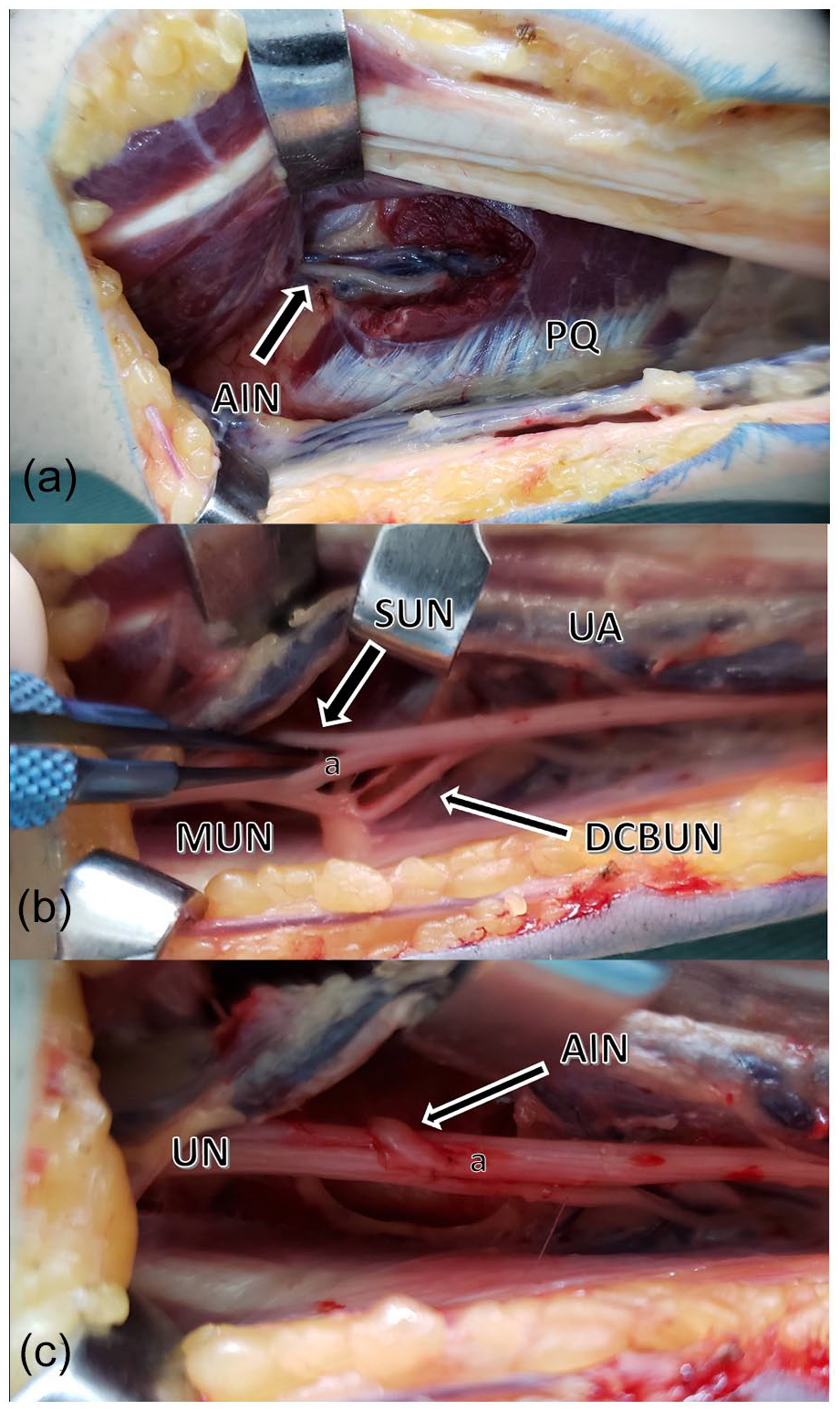
Intraoperative AIN to ulnar SETS. (a) AIN location in the PQ. (b) Locating the MUN between the SUN and the DCBUN near the UA. (c) AIN to UN SETS.
The patient accomplished postoperative hand therapy for 7 months, showing significant improvement in hand function, partial recovery of the hypothenar muscle volume, and partial recovery of the fifth finger ulnar claw (Figure 4). There was also an improvement in grip strength, and its measurement by the JAMAR dynamometer reached values of 40.0 kg in the left hand and 42.0 kg in the right hand at 7 months of the postoperative period. The lateral pinch strength was 2 kg/f for the left hand and 10 kg/f for the right hand. The goniometer measurement showed a lack of 32° of PIP extension. Thus, marking an improvement of 38° of extension compared with the preoperative evaluation.
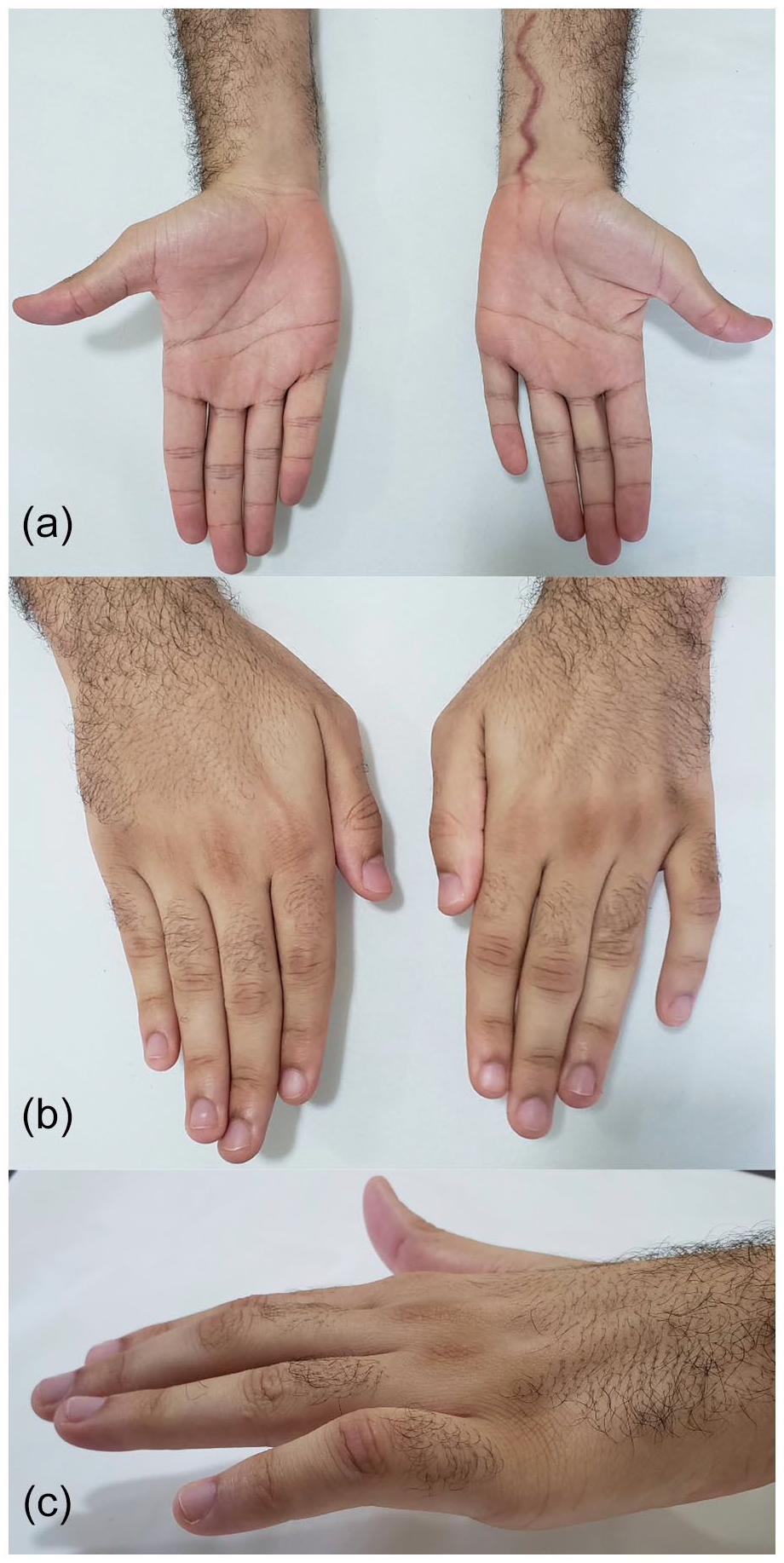
Postoperative clinical findings. (a) Palmar, (b) dorsal, and (c) lateral view partial recovery of the hypothenar volume and ulnar claw.
Discussion
Hirayama disease with isolated ulnar impairment is an atypical condition in the clinical scenario. Despite the few studies described in the literature, there is no consensus about the best management. Since its description, few studies were available to guide the best management.1-5
Clinical features do not include sensory changes, although atrophy of the intrinsic hand musculature was always present. Weakness in pinching and grip are common, especially loss of dexterity. Pain symptoms are not included, but at least 80% of patients complain of worsening in the cold and tremors (minipolymyoclonus) as a common finding. Only 10% of cases are bilateral. Clinical evaluation and electroneuromyography can show abnormalities in the motor pattern of the hand intrinsic muscles, with the absence of sensory symptoms.1,2,4 Electroneuromyography also presents a preganglionic pattern. Dynamic MRI is the gold standard for the diagnosis, showing epidural crescentic enhancing region. 6
The intrinsic muscle features in the hands are described as involving predominantly atrophy of the hypothenar muscles, mainly ADM, concerning the thenar muscles (abductor pollicis brevis). There may also be a loss of function of the dorsal interosseous, markedly of the first dorsal interosseous. Thus, ulnar claw, Froment, and Wartenberg are common findings during evaluation.2,3,6-8
Reports on the management of Hirayama disease include cervical collar therapy and spinal decompression surgery. There is a report of tendon transfer to restore thumb opposition in a patient with Hirayama’s disease with the motor impairment of the median and ulnar nerves. At least 62.5% of patients who had no therapeutic intervention had progression arrest within 3 years and 85% within 5 years, like our patient. However, the deformities caused may be permanent, such as the ulnar claw reported in this study.1,2,7,8
Anterior interosseous nerve to ulnar nerve SETS is a known nerve transfer approach to recover motor ulnar nerve function. 9 This report believes that we could find a suitable indication for this technique because there was still intrinsic ulnar nerve function under intraoperative electrical stimulation.
After 7 months of the postoperative period, the hand function was better than the initial evaluation, and there was a partial improvement in the ulnar claw. The patient reported improvement of the tremor. Despite seeming to be a minimal improvement for this patient, it allowed him to optimize typing on the computer and smartphones. He also returned to some types of physical activity and regained hand dexterity. Although ulnar nerve palsy is a devastating condition and often challenging to manage, we believe that the nerve transfer helped this patient.
We believe the role of the hand surgeon should be focused on actively participating in the diagnosis, interpreting electroneuromyography, and restoring functional hand capacity based on the available donor nerve options or tendon transfer. In this case, we chose the AIN to ulnar nerve SETS.
Despite the few reports in the literature of tendon transfers and no reports of nerve transfers for Hirayama disease, we believe that an adequate clinical diagnosis through predominantly motor symptoms and electroneuromyographic findings may allow the hand surgeon to assist the management of ulnar nerve palsy. Given this, we hope our report may encourage hand surgeons to manage these conditions.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This report has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Statement of Informed Consent
The patient and his family were informed that data from the case would be submitted for publication and gave their consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.