
Abstract
Background:
The regenerative potential of the nail bed after trauma remains controversial.
Methods:
We performed a retrospective review of 51 patients who underwent nail bed reconstruction with 2 techniques (direct flow island flap or a Tranquilli-Leali “Atasoy” flap) due to trauma involving the nail bed complex. These 2 flaps were used to support the loss of distal substance and to allow the regeneration of the nail bed. Outcomes were analyzed for at least 18 months. There were 34 men (66.7%), and the average age was 16.1 years. Most patients (56.9%) had crush injuries. The little (16) and index (14) fingers were the most affected. Twenty-seven were children (range: 4-11) with an average age of 7.4 ± 1.9 years. The middle finger was the most affected (29.2%).
Results:
The outcomes were good to excellent in 41 operated patients (80.4%). Hook nail was absent in 84.3% of the patients. Most patients (98%) did not develop necrosis. Children had an excellent/good outcome rate of 85.2%, while in adults, the rate was 75% of cases (P = .485).
Conclusion:
The direct flow island flap is superior in terms of outcome, regardless of age, sex, affected finger, dominant hand, type of trauma, and injury zone. In cases where there was a correct reconstruction of the hyponychium, there was regeneration of the nail bed.
Introduction
Multiple factors may lead to fingernail loss, most commonly mycotic infection, third-degree burns, trauma, tumor excision, or untreated subungual hematomas, with resultant cosmetic and functional deformities. 1 Missing or deformed nails are more of a cosmetic concern than a functional one. The development of self-image and comparison to peers can lead to adverse psychological effects in cases of nail loss secondary to trauma. A recent study found the 3 most important concerns for parents regarding their child’s nail bed injury are regrowth of the nail, infection, and long-term appearance. 2 Initial reports of free nail bed grafting onto decorticated bone produced inconsistent results. Currently, the most successful surgical treatment for restoration of the nail bed includes microsurgical transfer of the great toe nail bed to the thumb or a part of great toe nail bed to a long finger. Although some options for nail bed reconstruction in adults have been proposed, the capacity for regeneration of the nail bed in pediatric patients has not been fully described. Rather than simply describing different treatment methods for fingertip reconstruction, we have sought to shed light on the fact the nail bed has greater regeneration potential in pediatric and adult patients. Because the nails are a relatively underappreciated structure, controversy remains regarding formation of the nail as well as how the nail bed heals. Studies have shown that approximately 80% of the nail thickness is formed by the germinal matrix, while 21% is formed by the nail bed. Johnson and Shuster demonstrated that nail production, measured as the change in dry nail thickness, occurs at a rate of 0.13-mm thickness per millimeter of length along the germinal matrix, and at a rate of 0.02-mm thickness per millimeter of length along the entire proximal and distal nail bed. 3
Materials and Methods
We performed a retrospective chart review of 51 patients who underwent fingertip reconstruction with 2 techniques (direct flow island flap or a Tranquilli-Leali “Atasoy” flap) due to trauma involving the nail bed complex between January 2014 and August 2017 at our institution’s division of Hand Surgery and Microsurgery Service.
We divided the patients into groups by age and compared their results separately. The variables analyzed were age and sex, affected finger(s), mechanism of trauma (laceration, crush, avulsion), hand (dominant or nondominant), type of injury (Zook type) (Figure 1), and time from trauma to surgery.
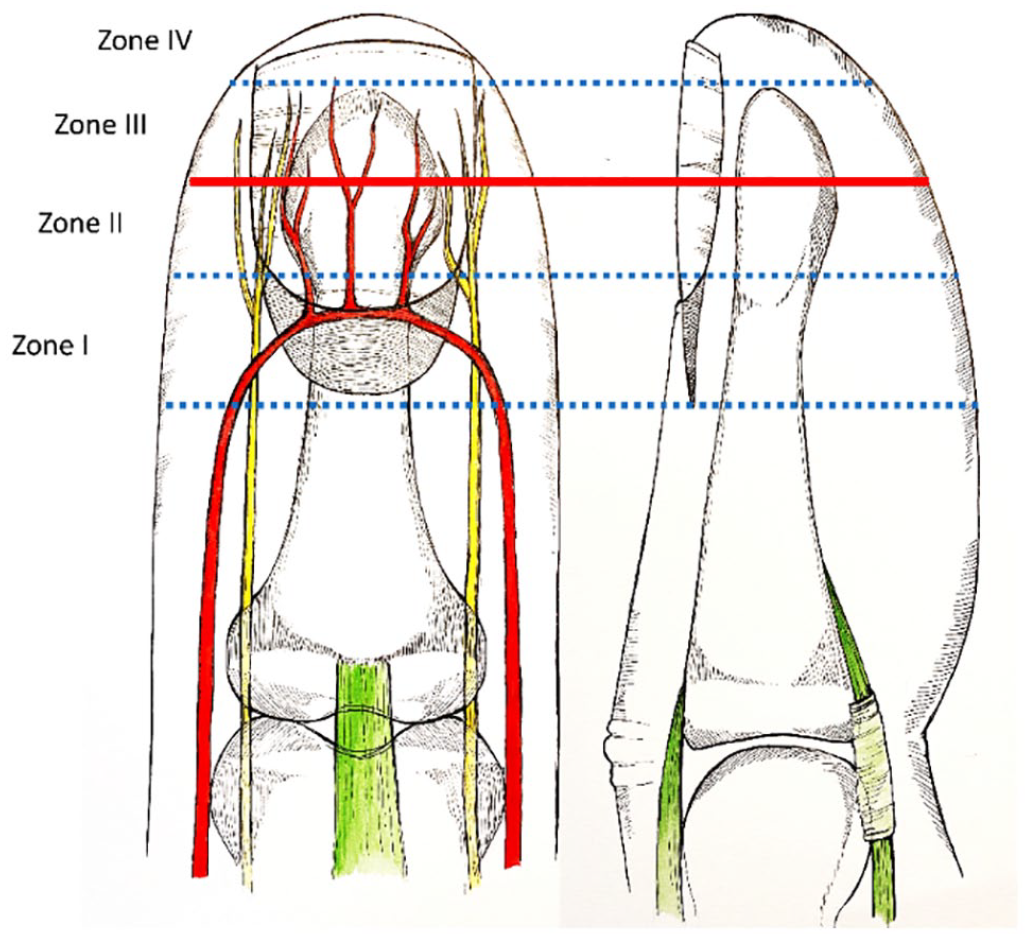
Zook classifications.
Complete data were available for all 51 patients. There were 34 men (66.7%), and the average age was 16.1 years (range: 3-35). Most patients (56.9%) had crush injuries, while 33.3% presented avulsions and 9.8% lacerations. The little (16) and index (14) fingers were the most commonly affected, followed by the middle (12) and ring (9) fingers. The dominant hand was affected in 40% of patients. According to the Zook classification for fingertip injuries, 25 patients had a type 2 injury, 17 patients had a type 3 injury, and 9 had a type 1 injury. Average time between trauma to surgery was 5.8 hours (range: 1-12). Mean patient follow-up was 27.5 months (range: 18-61).
The patients were separated by age groups. Twenty-seven were children (range: 4-11) with an average age of 7.4 ± 1.9 years, of whom 20 were boys (74.1%). Most of the children suffered crush injuries (58.3%) with Zook type II being the most commonly found, affecting 48.1% of the children, followed by types III (33.3%) and I (18.5%). The little finger was the most affected (37%), followed by the index (29.6%), middle (18.5%), and ring (14.8%) fingers. The dominant hand was injured in 74.1% of the cases.
Among the adults (range: 18-35 years), 24 patients were identified, with an average age of 25.8 ± 5.3 years, of whom 14 were men (58.3%). The most prevalent injury was crush (54.2%) and 50% had Zook type II, followed by Zook types III (33%) and I (16.7%). The middle finger was the most commonly affected (29.2%), followed by index (25%), little (25%), and ring (25%) fingers. Most of the injuries involved the dominant hand (83.3%).
This study is in accordance with the ethical standards of the institutional research committee (approval number: 2.915.202) and with the 1964 Helsinki declaration on research in human subjects and its later amendments or comparable ethical standards.
In our series, 12 (23.5%) cases were treated with Tranquilli-Leali technique and 39 (76.5%) cases with direct flow island flap technique. The average interval between trauma and surgery was 5.0 ± 1.7 hours among the adults and 6.6 ± 2.7 hours among the children.
Outcomes were evaluated based on 3 criteria. First, presence and degree of tissue necrosis (1—absent, 2—less than 50%, 3—greater than 50%). Second, nail appearance classification, measured by physicians not involved in the treatment who evaluated the results using photographs taken before and after surgery. The results were classified as excellent, good, fair, or poor according to the length of the reconstructed fingertip and the appearance of the nail unit 4 (Supplemental material Table 1). And the last criterion was range of motion, which was measured in degrees of active and passive mobility, compared with the contralateral (CL) phalange and classified as 1—100% CL, 2—75% CL, 3—50% CL, and 4—25% CL.
The characteristics of comparing the techniques by age group are divided into groups that analyze the length of the fingertip reconstruction and the appearance of the nail. Excellent results obtained over 90% opposite normal fingertip length and no nail deformity. Good results obtained 70% to 90% of opposite normal fingertip length and mild decrease in nail size. Fair results obtained 50% to 70% of opposite normal fingertip length and moderate decrease in nail size. Poor results obtained less than 50% of opposite normal fingertip length and severe decrease in nail size (hook nail, scarred nail, disturbance of nail growth).
Surgical Technique
The operations were always performed by the same surgeon, with regional anesthesia for adults and general anesthesia for the children and with use of a pneumatic cuff on the upper arm, which was released only at the end of the procedure. In all cases, there was a loss of substance from the distal extremity that compromised the pulp and nail bed and 2 types of flaps were performed to reconstruct the digital pulp and provide adequate support for the bed to regenerate and bring the nail with it. The Tranquilli-Leali, V-Y flap consists of a temporary flattening of the fingertip, with a moderate advancement of 0.4 to 0.5 cm available, thus limiting the indications for its use to distal. I routinely used a fine needle inserted transcutaneous through the distal edge of the flap, skewering the skin to the bony segment.5,6 The direct flow island flap is useful for coverage of major pulp loss and has the principal advantage of improved mobility. This flap may be raised on a single pedicle, and this is its real value in the management of extensive loss of substance in digits which are used in precision pinch.7,8 In this series, these flaps were made to maintain the regeneration of the nail bed (Figures 2-7).
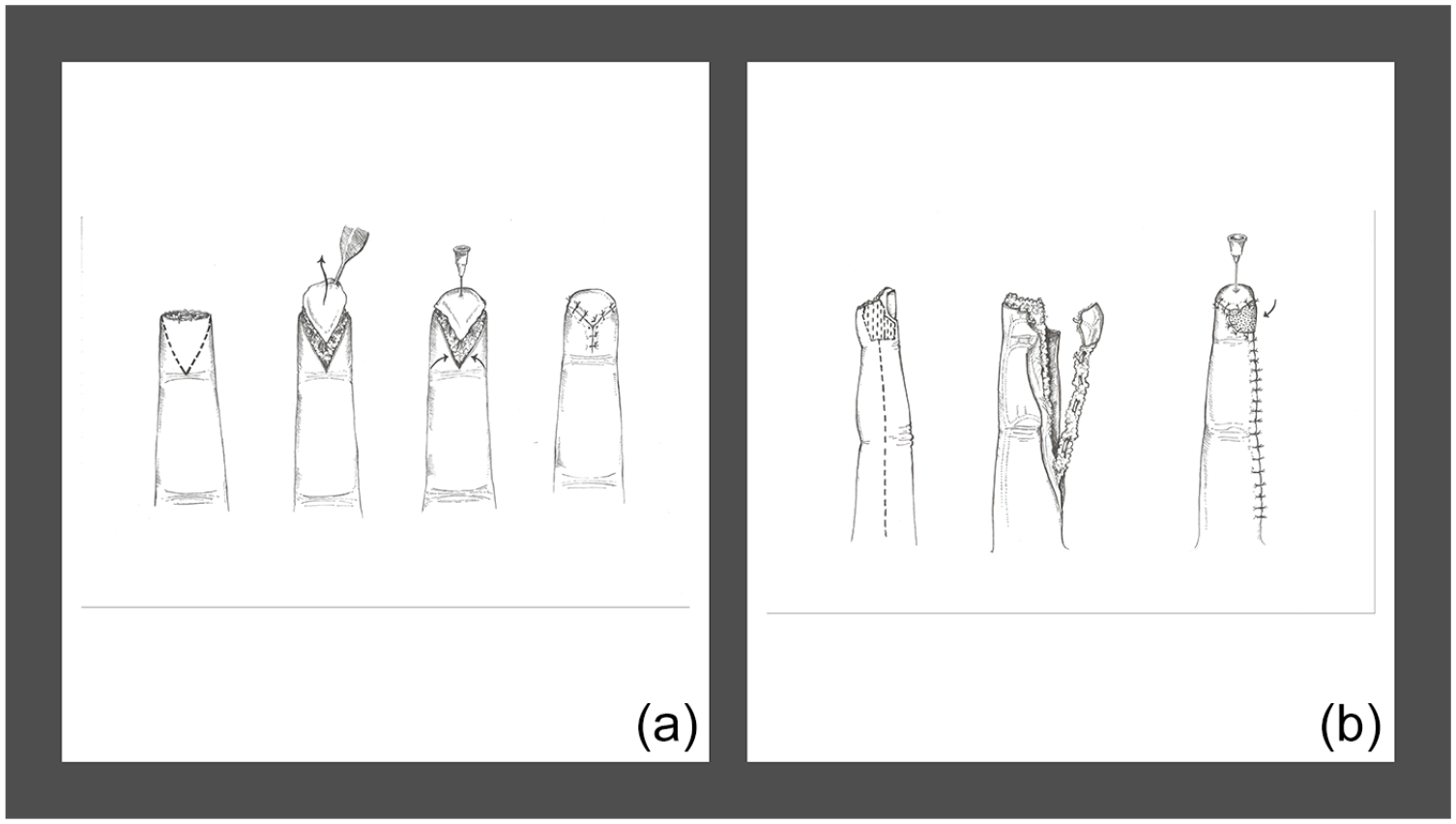
(a) Tranquilli-Leali Atasoy flap. (b) Direct flow island flap.
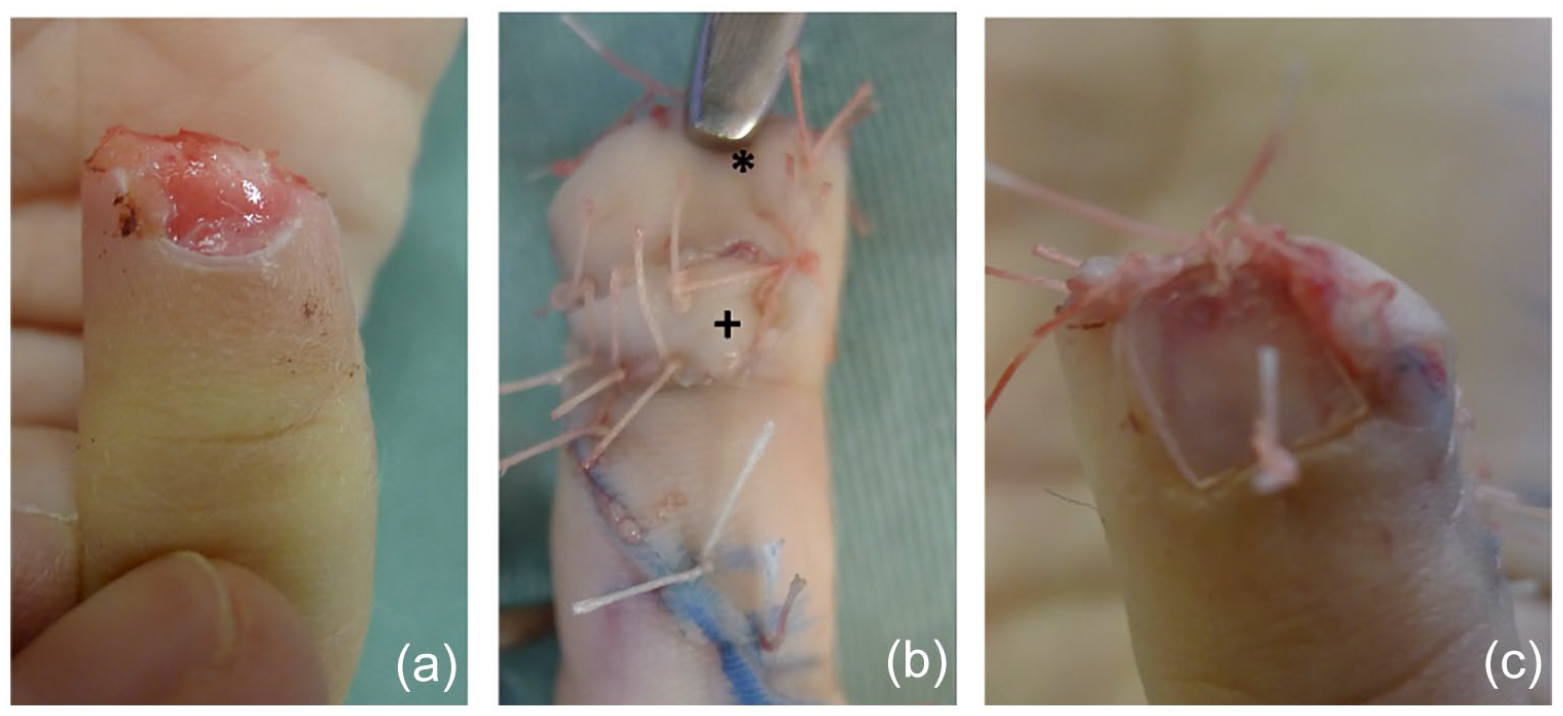
(a) Distal trauma, loss of nail bed substance and finger pulp, Zook II. (b) Direct flow island flap dissected and placed in the recipient area. Positioned volarly and distally (*)/skin graft in the donor area of the flap (+). (c) Placing a silicone sheet to unify the nail bed, minimize pain when changing dressings and connect to the distal edge of the direct flow island flap.
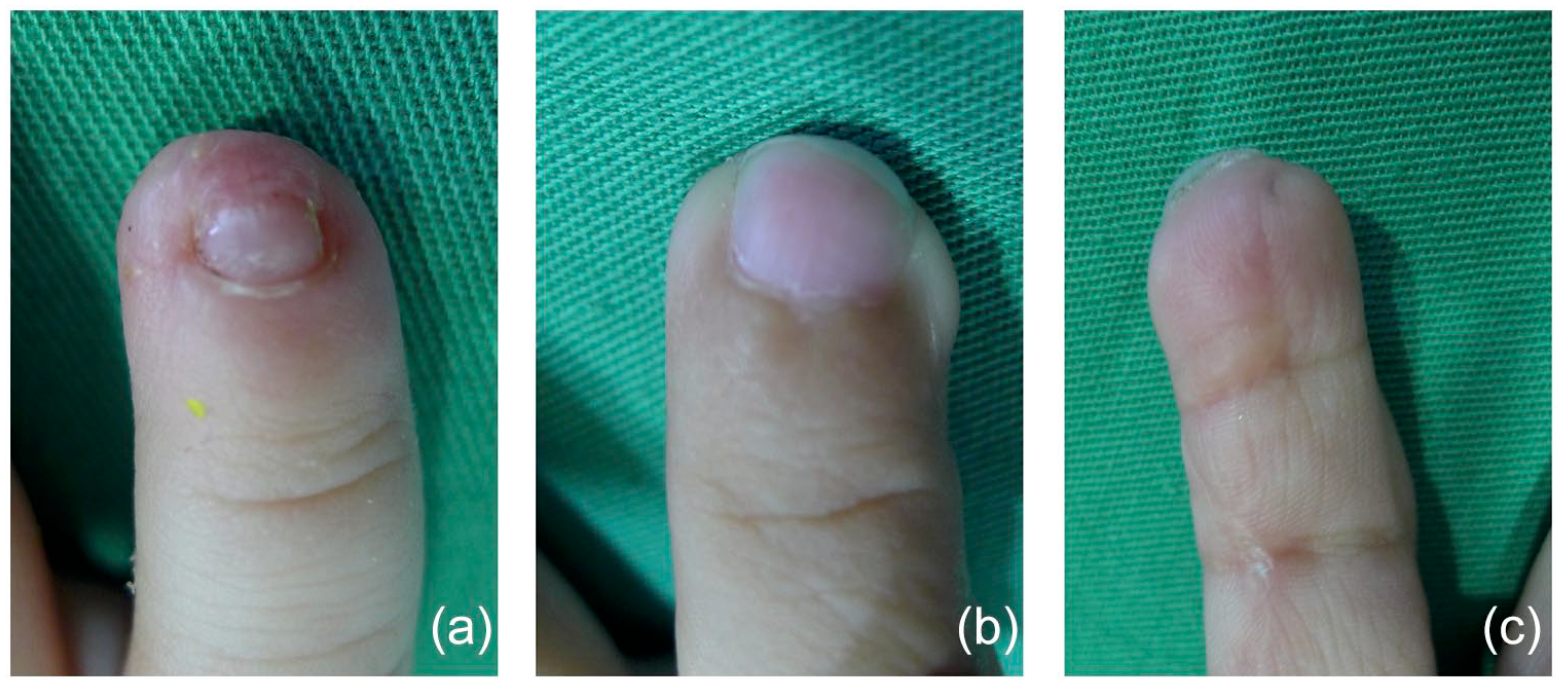
(a) Aspect of the nail complex at 2 months. (b) Aspect at 22 months, note the regenerated nail bed. (c) Volar aspect of the direct flow island flap.
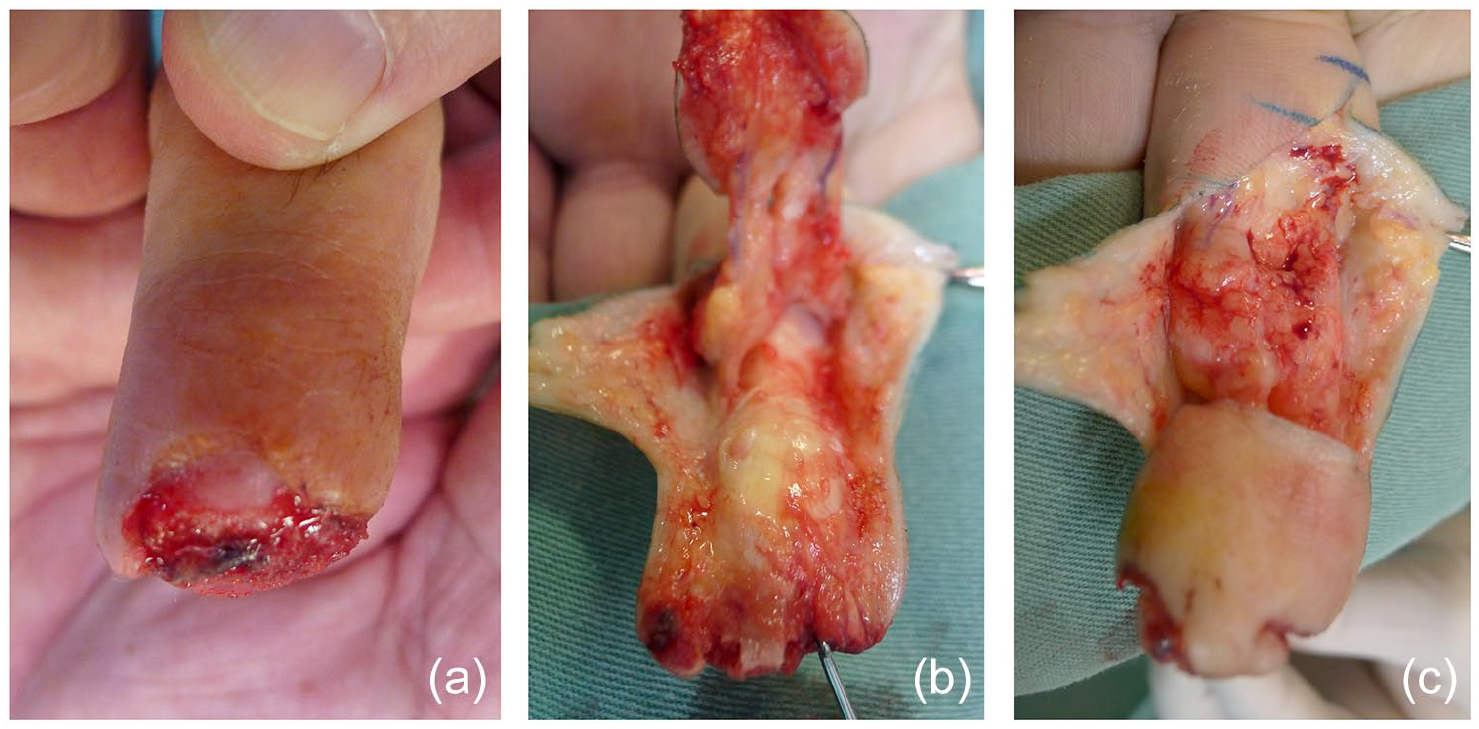
(a) Loss of distal substance from the pulp and nail bed with bone exposure Zook II. (b) Dissection of the direct flow island flap. (c) Placing the flap in the distal position.
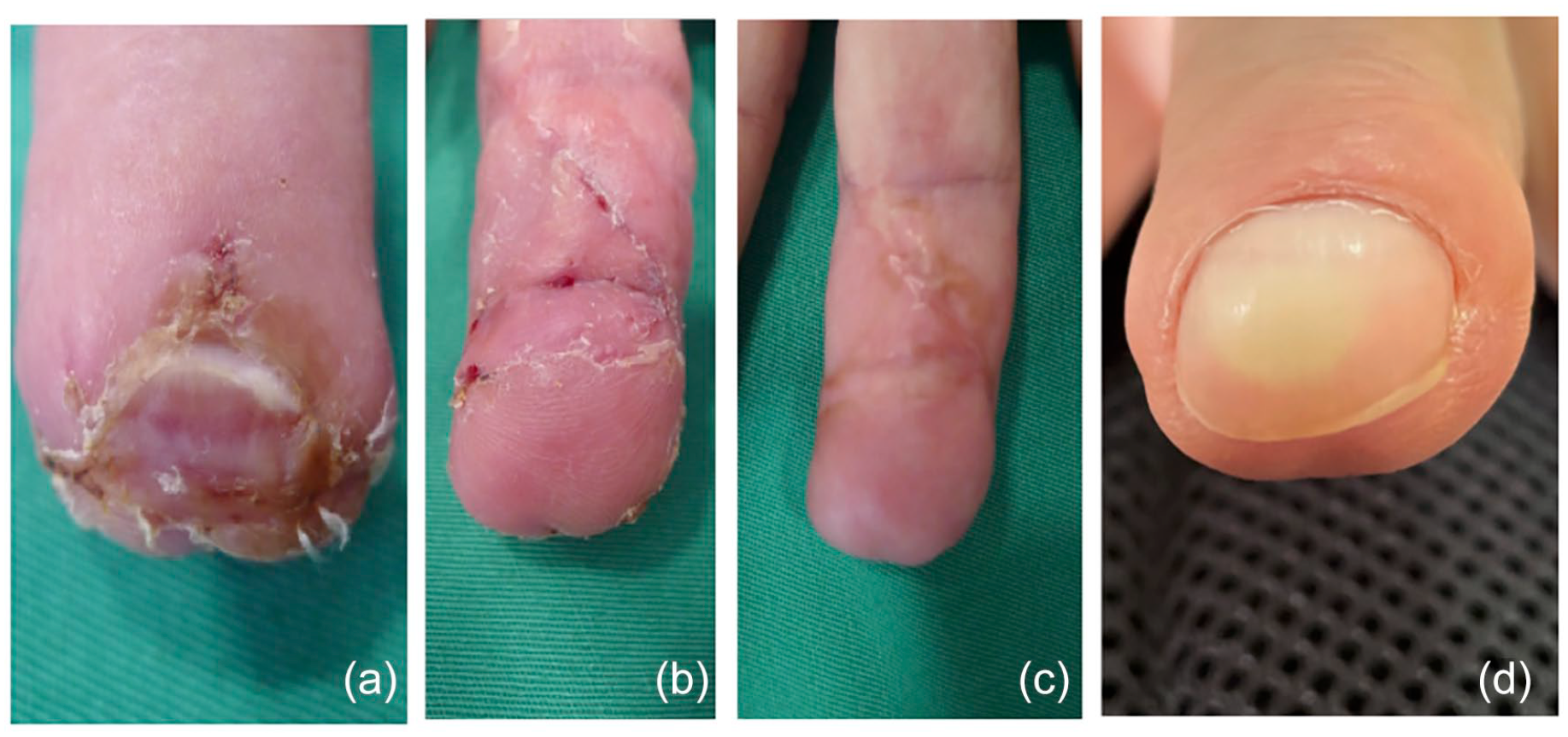
(a) Dorsal aspect at 3 weeks. (b) Volar aspect at 3 weeks. (c) Volar view at 18 months. (d) Dorsal view “nail complex” at 18 months.

(a) Index finger, dorsal aspect, nail bed necrosis. (b) Index finger, volar aspect, distal digital pulp necrosis. (c) Result, volar aspect. Direct flow island flap. (d) Result, dorsal aspect. Nail bed at 24 months.
Results
The outcomes were good to excellent in 41 operated patients (80.4%). Children had an excellent/good outcome rate of 85.2%, while in adults, the rate was 75% of cases (P = .485). Most patients (98%) did not develop necrosis. Only 1 child had necrosis in less than 50% of the Tranquilli-Leali flap, which was not found in adults (P = 1.0). Hook nail was absent in 84.3% of the patients, with only 14.8% of the children and 16.7% of the adults presenting this complication (P = 1.00). Active and passive joint mobility was unaffected in most cases, and 84.3% of the patients had 100% active and passive mobility in relation to the CL finger. Only 3 children (11.1%) had 75% of active and passive joint mobility compared with the CL finger, and the same was found in 5 adults (20.8%) (P = .451).
Thirty-nine patients (76.5%) underwent the direct flow island flap; of those, 19 (70.4%) were children. Eleven children (57.9%) and 11 adults (55%) had crush injuries, with no statistically significant difference. All the children and 90% of the adults had excellent/good outcomes with the direct flow island flap (P < .005). When analyzing the Zook type of each age group, it is possible to identify a higher prevalence of Zook type II, with 47.4% in children (P = .216) and 60.0% in adults (P = .008). In both age groups, all patients operated with this direct flow island flat did not present hook nail (P < .005).
The Tranquilli-Leali flap reconstruction was performed on 8 children and 4 adults. Five children (62.5%) and 2 adults (50%) suffered crush injuries, with no statistically significant difference. In children, Zook type II and III had a prevalence of 50% (P = .216), and, in adults, Zook type 3 was found in all patients (P = .008). Excellent and good results were found in 50% of children (P = .004) and in no adults (P = .001).
Comparing the age groups, regardless of the technique used, 23 children (85%) and 18 adults (75%) had excellent/good results. Only the Zook type showed a statistically significant difference. In adults, Zook type I or II had 77.8% of excellent/good results (P = .018), while in children, 69.5% (P = .531). Twenty-three children (100%) who presented excellent/good results did not present hook nail, while 4 children (100%) who presented regular/poor results presented hook nail (P < .01). Eighteen adults (100%) who presented excellent/good results did not present hook nail, while 4 adults (66.7%) who obtained regular/poor results presented hook nail (P < .01).
When analyzing the factors associated with the excellent/good results, the direct flow island flap technique presented a relative risk (RR) of 3.07 compared with the Tranquili-Leali technique (P = .004), regardless of the age group, the Zook type, or the type of trauma. Comparing age groups, children had a greater chance of having excellent/good results (RR: 1.27, P = .011). Comparing the Zook type, Zook II had an RR of 1.33 (95% confidence interval [CI], 0.98-1.82, P = .067) and Zook III had an RR of 1.20 (95% CI, 0.83-1.74, P = .332) when compared with Zook I (Supplemental material Tables 2–4).
Statistical Analysis
Quantitative variables were described using the mean and standard deviation and categorical variables by absolute and relative frequencies. To compare means, the Student t test was applied. When comparing proportions, Pearson χ2 or Fisher exact tests were used. To control confounding factors, the multivariate Poisson regression model was applied. Relative risk was calculated in conjunction with 95% CI. The level of significance adopted was 5% (P < .05) and the analyses were performed using the SPSS version 21.0 program.
Discussion
Fingertip injury is very common, often with nail bed injuries and shortening of the finger. However, there is still no consensus as to the optimal reconstructive techniques in terms of cosmesis and function. This may partly be due to the controversy that has surrounded the physiology of nail growth and regeneration. For many years, it was believed that the nail was produced by the germinal matrix alone. An article in 1991 attempted to put an end to the discussion, concluding that nail formation happens continuously throughout the nail bed, and not only in the germinal matrix. 9 These authors found that approximately one-fifth of the nail thickness from the lunula to the distal free edge of the nail was contributed by the nail bed. Nonetheless, formation of nail along the nail bed remains a subject of controversy.
Regarding surgical technique, there used to be reluctance toward free nail bed grafting, owing to an (now historical) article published in 1955 describing nail growth in less than half of the grafts, with only 20% yielding cosmetically acceptable results. 10
However, Endo et al, in 1997, reported complete and aesthetically pleasing nail growth after performing microsurgical transfer of a full-thickness nail bed graft from the great toe to the distal phalanx of a finger. These contributed to the idea that free full-thickness grafts of the nail bed may be the method of choice for reconstructing a completely missing nail. 11 Evidently, despite the very good outcomes with microsurgical transfer of the great toe, this requires a long operating time, microsurgical skills, and significant donor site morbidity.
One of the 2 techniques used in this study—first described in 1935 5 and subsequently reported in 1970 6 —consists of a triangular flap which is designed with the base at the edge of the amputation and the apex at the distal interphalangeal crease. 12 It is most indicated for distal oblique and transverse amputations.
The other technique used in our series, the direct flow island flap, is indicated for coverage of major pulp loss.7,8,13,14
We decided to separate adults from children because they are patients with different metabolic healing responses. In our pediatric patient group, the general outcome was good with either technique. Although tissue necrosis was only present in 1 case (<50%) that underwent the Tranquilli-Leali flap technique, the overall functional and cosmetic result was still adequate. Apart from this complication in 1 case, the best results were seen in patients with Zook types II to III who underwent the direct flow island flap technique.
It is significant to note, however, that no patient presented with a cosmetic or functional outcome considered to be fair or poor, regardless of injury classification or surgical technique applied.
Johnson et al demonstrated favorable results by using boneless perionychial grafts taken from the amputated fingertips supported by flaps used to reconstruct the finger pulp in 4 adults and 4 infants. There were no complications, and joint mobility was fully preserved in the pediatric cases. In that same group of patients, nail deformity was minimal in 1 of them and the other 3 had no deformities. The authors of that study recommend harvesting the perionychial tissue, performing nail bed repair and replacing it on its prior bed, as well as supporting it with a local flap to reconstruct the fingertip, particularly in children, when replantation/revascularization is not possible. 15
Hwang et al used nail bed flaps and grafting in the emergency department for distal injuries and found excellent and good results in 16 of the 20 operated cases. 4
Between 2000 and 2009, we observed that in 15 patients who underwent nail bed grafting in the emergency department, only 2 obtained good results, 5 regular, and 8 poor. Owing to these unsatisfactory results, we abandoned this technique in emergency situations. 16
Ogo also observed that the nail bed is capable of regeneration. The study consisted of 4 cases of posttraumatic nail deformities in which nail bed regeneration was observed in all patients who underwent a full-thickness skin graft of the nail bed. He noted that the best results were associated with an adequate nail matrix size, whereas nail matrices of inadequate size did not show good nail bed growth. 17
While surgeons often opt not to reconstruct zone 1 fingertip and nail bed trauma in adults due to the risk of a hook nail of parrot beak deformity, we believe the direct flow island flap is a good option because it provides a larger quantity of suitably sensitive tissue allowing for adequate regeneration of the nail bed in both children and adults. We believe it is this distal tissue supplementation that enables the regeneration of the nail bed. 18 That is, the reason why we assume the Tranquilli-Leali Atasoy does not allow the nail bed to regenerate when there is a loss of nail bed in the lesion is because the flap does not advance over the nail bed.
Although we have 51 patients in this series, it was possible to carry out several statistical analyses and draw conclusions that allow us to establish a course of action for a certain type of trauma and obtain a satisfactory standard result.
In our series, We have found reconstruction of the fingertip, potentially by offering support to the growing distal phalanx, as well as a possible intrinsically increased potential for nail bed regeneration in children and adults.
Conclusion
Nail bed injury continues to be a relatively underappreciated topic of hand surgery, as many patients who sustain trauma or other injuries to the nails do not seek out medical help, and there is currently no consensus as to the optimal treatment of such injuries. Regeneration of the nail bed occurs after reconstruction of the hyponiquium. A base is placed, which can be considered as a substrate (direct flow island flap or a Tranquilli-Leali “Atasoy” flap), so that the regeneration process can occur. Our study shows statistically that the direct flow island flap is superior in terms of outcome, regardless of age, sex, affected finger, dominant hand, type of trauma, and injury zone (Zook). And, that there is no need to perform nail bed grafting, considering that when there is tissue support provided by the direct flow island flap, the nail bed regenerates, regardless of the patient’s age.
Supplemental Material
sj-docx-1-han-10.1177_15589447211064359 – Supplemental material for Does the Nail Bed Regenerate?
Supplemental material, sj-docx-1-han-10.1177_15589447211064359 for Does the Nail Bed Regenerate? by Jefferson Braga Silva, Gabriela A. Magnus, Valentina Stanham, Cecília G. Wolff, Carolina S. Aranchipe and Carolina Cauduro in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.