
Abstract
Background:
Degenerative arthritis of the wrist is a common condition often treated with 4 corner arthrodesis (FCA) or a partial wrist fusion. A number of limited intercarpal arthrodeses have been proposed for treatment of this condition. One technique, described by Wang and Bednar in 2012, involves fusion of the lunatocapitate and triquetrohamate joints. This study presents midterm follow-up of outcomes following this 2 column arthrodesis.
Methods:
From 2000 to present, patients who underwent lunatocapitate and triquetrohamate arthrodesis were evaluated. The original cohort from the 2012 study was reviewed, as well as any additional patients who since underwent this procedure. Only patients who had greater than 5 years of follow-up data were included. Outcomes included demographics, wrist range of motion, grip strength, complications, and radiographic evidence of union.
Results:
Twenty-one cases were included in the final analysis. Mean follow-up was 8.75 years. Wrist extension and flexion were 58% and 90% of the unaffected side, respectively. Grip strength was 92% of the unaffected side. Osseous union was achieved in 95.2% of cases. Two cases underwent revision surgery, one for nonunion and one following a fall.
Conclusions:
Lunatocapitate and triquetrohamate arthrodesis offers a treatment for wrist arthritis that yields good clinical outcomes, low nonunion rates, and no conversions to total wrist arthrodesis, as shown by 5-year follow-up data. Limited intercarpal arthrodesis is an alternative to FCA, with the advantage of a smaller surgical footprint and simpler technique, while still providing excellent mid- to long-term outcomes.
Keywords
Introduction
Wrist arthritis is a degenerative condition commonly managed and treated by hand surgeons. Frequently, it is the result of scapholunate advanced collapse (SLAC) or scaphoid nonunion advanced collapse (SNAC). Whether the cause is from ligament attenuation, as in SLAC wrist, or secondary to a scaphoid fracture nonunion, as in SNAC wrist, both conditions can lead to a progressive and predictable pattern of wrist arthrosis, resulting in chronic wrist pain and stiffness. Watson previously described the pattern and progression of collapse in wrist arthritis.1,2 There are a variety of treatment options for wrist arthritis. Partial wrist fusions are one type of treatment for certain patterns of arthritis that preserve some degree of wrist motion. Four-corner arthrodesis (FCA) with scaphoid excision, as described by Watson et al 3 in the 1980s, has been a frequently used method for motion-preserving reconstruction of the wrist joint. These procedures are typically performed for more advanced stages of SLAC and SNAC wrists.
While results following FCA have shown preservation of grip strength and functionality, there has been concern over the nonunion rate and progression of degeneration necessitating conversion to total wrist arthrodesis following these procedures.4-7 Subsequently, a number of limited carpal arthrodeses have been proposed, with the central rationale suggesting that the fusion of fewer carpal bones leads to similar outcomes with a smaller surgical footprint and fewer complications.7-10 One such technique, as described by Wang and Bednar in 2012, involves scaphoidectomy and a 2 column fusion between the lunatocapitate and triquetrohamate articulations. 8 Headless compression screws are used to facilitate fusion between the capitate and lunate as well as the hamate and triquetrum, augmented with autologous bone graft taken from the excised scaphoid. Their initial results demonstrate similar range of motion, grip strength, and nonunion rates as compared to FCA. 8
To date, studies reporting long-term results on such procedures are sparse and remain limited. The purpose of this study is to review the outcomes of this 2 column arthrodesis of lunatocapitate and triquetrohamate for degenerative SLAC or SNAC arthritis, with long-term follow-up data of the original cohort. All additional and eligible patients treated by this technique were additionally reviewed.
Materials and Methods
This study was approved by our institutional review board and conducted according to its protocol and guidelines. A retrospective chart review was performed to identify patients who underwent scaphoid excision and 2 column fusion by one surgeon. From 2000 to present, Current Procedural Terminology (CPT) codes corresponding to scaphoid excision (25210 carpectomy) and intracarpal arthrodesis (25825 arthrodesis with autograft and/or 25820 intercarpal fusion wrist) were queried and a chart review performed to identify patients who were evaluated and treated with scaphoid excision and lunatocapitate and triquetrohamate arthrodesis. The original cohort of patients was identified and all additional patients identified by query and chart review through 2015, to allow for an adequate follow-up period, were included. Patients’ subsequent follow-up visits were reviewed and clinical and radiographic outcomes were collected from the patients’ most recent follow-up visit with the surgeon. Patients were excluded if they had less than 5 years of follow-up. Outcomes included measurements obtained from the surgeon using a goniometer and Jamar dynamometer and recorded in the chart for wrist range of motion (flexion, extension, radial deviation, and ulnar deviation), grip strength as recorded from Jamar level III testing, as well as complications as defined by unexpected outcomes recorded in clinic notes or return to the operating room for revision surgery. Radiographic analysis for osseous union and maintenance of carpal alignment, as well as evidence of hardware failure as documented in the surgeons’ notes was also recorded.
Surgical Technique
An incision is made in line with the third ray over the dorsal wrist and skin flaps are raised at the level of the extensor retinaculum. The third dorsal extensor compartment is entered and extensor pollicis longus is freed and retracted ulnarly. The second and fourth extensor compartments are elevated to facilitate exposure. A neurectomy of the posterior interosseous nerve is then performed. A ligament sparing capsulotomy is performed to expose the proximal row. The scaphoid is excised using rongeurs and osteotomes. The surfaces of the capitate, lunate, hamate, and triquetrum are denuded in the midcarpal joint with a rongeur and high-speed burr. The capitohamate and lunotriquetral surfaces are not disturbed. Capitolunate reduction is performed by translating the capitate volar and ulnar to restore sagittal alignment. Provisional fixation with a 1.6-mm Kirschner wire (K-wire) is placed under fluoroscopic guidance from capitate to lunate. The wrist is brought through a range of motion under fluoroscopy to ensure symmetric flexion and extension arcs. The first guidewire is placed from proximal dorsal lunate toward distal volar capitate, drilled, measured, and an antegrade headless compression screw is placed over the wire (Acutrak mini screw; Acumed, Hillsboro, Oregon). The provisional K-wire is replaced with a second guidewire and subsequent retrograde headless compression screw is placed from distal dorsal capitate to proximal volar lunate. To facilitate appropriate trajectory of the second screw, a trough is created in the dorsal base of the third metacarpal. A third guidewire is then placed from triquetrum to hamate and an antegrade headless compression screw is inserted. Cancellous graft from the excised scaphoid is packed into the arthrodeses sites. Fluoroscopy confirms appropriate alignment and fixation, and the wrist is ranged to confirm fixation and lack of impingement. The dorsal wrist capsule and extensor retinaculum is closed with non-absorbable suture beneath the extensor pollicis longus tendon. Skin is closed with nylon suture and a bulky dressing with a volar thumb spica splint is applied. Patients underwent suture removal at 2 weeks and short arm casting for 4 additional weeks followed by rigid orthosis and range of motion exercises with therapy at 6 weeks. Bracing is typically discontinued by 10 to 12 weeks postoperatively.
Results
There were 103 total procedures for scaphoid excision and intercarpal arthrodesis performed between May 2001 and December 2015. Eighty-two of these patients were excluded for follow-up less than 5 years from surgery, for a total of 21 cases included in final analysis. There were 2 patients who subsequently had scaphoid excision and intercarpal arthrodesis performed on the contralateral side during the study period, all patients were included in final analysis. Average patient age at time of surgery was 54 years old. There were 6 females and 15 males. There were 14 cases for which the work status was available; 7 (50%) were laborers, and 7 (50%) were non-laborers. Worker’s compensation status was available in 16 cases; 6 (38%) were worker’s compensation cases, and 10 (62%) were not worker’s compensation cases. Time to return to work was available in 9 cases; average time to return to work was 3.8 months, 2 cases had weight restrictions on their duty, and there were no patients who were unable to return to work at all. Demographics for the entire cohort can be found in Table 1.
Demographics.
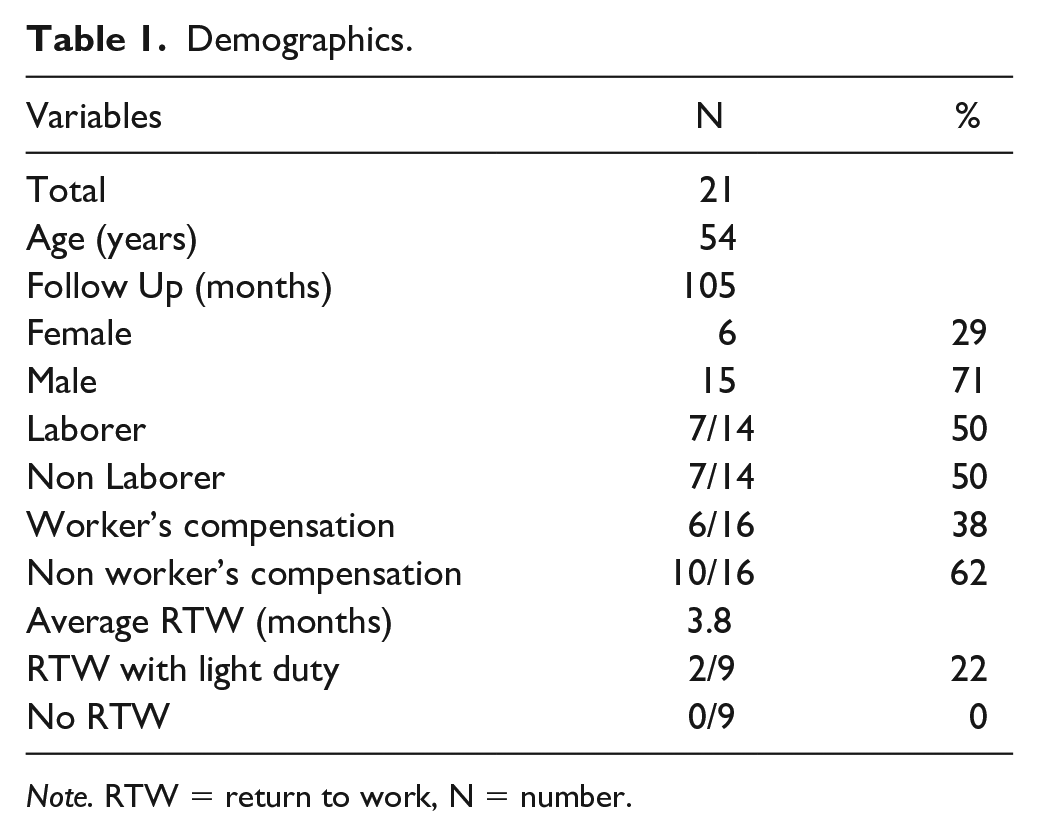
Note. RTW = return to work, N = number.
Follow-Up
The mean follow-up was 105 months (range 61 – 158 months).
Range of Motion
The mean wrist flexion-extension arc at final follow-up was 71% of the unaffected side (65 ± 7.6 vs. 95 ± 8.1 degrees, P = .0045). Mean wrist extension was 58% of the unaffected side (28 ± 2.5 vs. 46 ± 6.5 degrees, P = .0267). Mean wrist flexion was 90% of the unaffected side (36 ± 5.0 vs. 39 ± 6.5 degrees, P = .6344). All data outcomes as compared to contralateral side can be seen in Table 2.
Operative Versus Contralateral Side Outcomes.
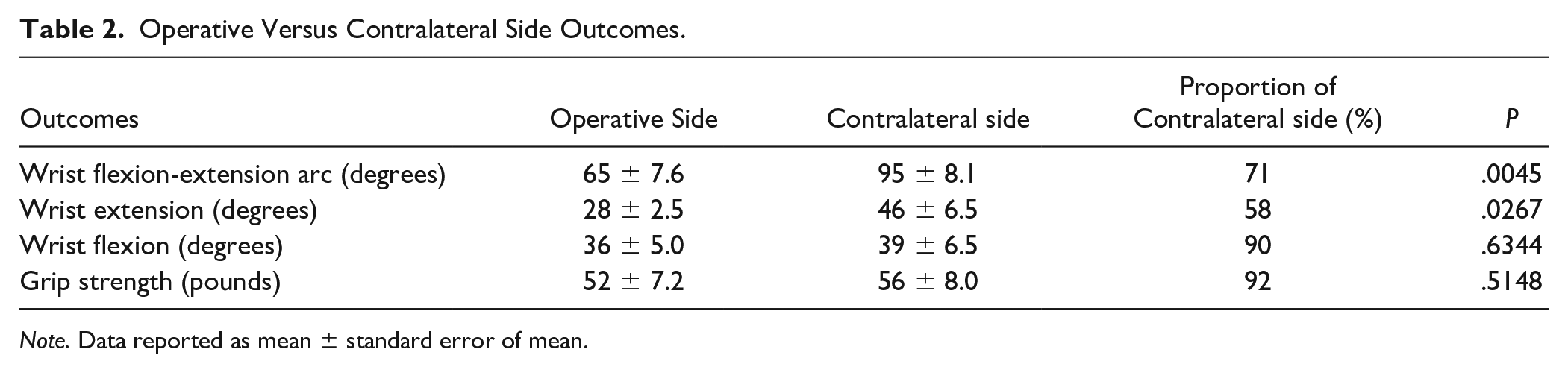
Note. Data reported as mean ± standard error of mean.
Grip Strength
At final follow-up, the mean grip strength was 52 ± 7.2 pounds, which was 92% of the unaffected side (56 ± 8.0, P = .5148) (Table 2).
Osseous Union
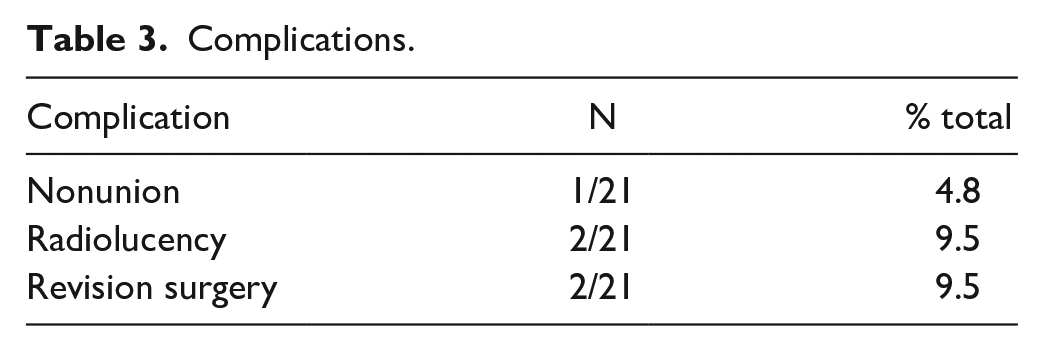
In the cohort, 20 out of 21 cases achieved osseus union, or 95.2% (Figures 1a and 1b). All patients who achieved clinical and radiographic union were evident by 10 to 12 weeks post operatively. Advanced imaging was not obtained unless there was concern for nonunion beyond the 10- to 12-week follow-up period. One case went on to nonunion (4.8%), requiring revision surgery (Table 3).

Anteroposterior and lateral radiographs of a patient (a) one year status post scaphoidectomy with lunatocapitate and triquetrohamate arthrodeses showing solid fusion mass and anatomic alignment of carpus and (b) 9 years status post arthrodesis with noted minimal progression of radiocarpal arthritis or secondary degenerative changes.
Complications.
Complications
There were 2 cases (9.5%) that had evidence of radiolucency around the hardware (Table 3). One involved the triquetrohamate screw, however there was noted to be fusion of the joint space and did not required revision surgery; additionally, there was no noted complications in this patient. The other case involved the lunatocapitate screw with nonunion of the fusion, necessitating revision surgery. Two of the 21 cases (9.5%) required revision surgery (Table 3). One case was for nonunion at the lunocapitate joint and underwent nonunion repair 25 months after the original surgery, which went on to fusion. The other revision case was for a fall and fracture through the lunatocapitate fusion mass, that occurred 5 years after primary surgery. This patient underwent repair of lunatocapitate fusion, which healed without complication.
Discussion
Limited intercarpal arthrodeses are emerging as an alternative to FCA for the treatment of wrist arthropathy. While the original technique of fusing the capitate, lunate, hamate, and triquetrum with excision of the scaphoid offers preserved range of motion, strength, and an acceptable union rate, the necessity of the fusion between all 4 carpal bones has been challenged.7-10 In their case series published in 2012, Wang and Bednar describe scaphoidectomy with lunatocapitate and triquetrohamate fusion as an alternative to FCA. Initial results were comparable to FCA in terms of wrist range of motion, grip strength, and nonunion. 8
The current study examines midterm (greater than 5-year) follow-up for scaphoidectomy with lunatocapitate and triquetrohamate arthrodeses in order to assess longer term outcomes and complication rates in these patients.
Wrist flexion-extension arc motion was 71% of the contralateral side postoperatively, with mean flexion-extension arc 65 degrees. This is comparable to mean values of postoperative flexion-extension arc of 62 degrees and 64 degrees following FCA in 2 systematic reviews.4,11 Additionally, a recent 10-year follow-up for FCA demonstrated a mean 68.8 degree arc. 6 Mean wrist extension in our cohort was 28 degrees and flexion was 36 degrees. This compares to range of motion reported in a systematic review of FCA by Saltzman et al, 4 which showed 39 and 32 degrees of postoperative extension and flexion, respectively. Furthermore, our results were similar to a systematic review by Mulford et al, 11 which showed extension and flexion to be 33 and 33 degrees following FCA.
Postoperative grip strength in this study was 92% in the operative side as normalized to the contralateral side. This was considerably better than results published by Saltzman et al 4 and Mulford et al, 11 which showed 75% and 74% grip strength postoperatively of the contralateral side.
In this study, 95.2% of cases achieved osseous union (4.8% nonunion rate). This was better than rates reported in the literature for FCA, at 6.9% and 5.5% nonunion rates.4,11 Of note, Mulford et al 11 stratified nonunion rate by FCA with wires or screws only (4.95%) versus with plate only (13.6%), which shows nonunion rate in our cohort to be better than the nonunion rate of FCA using wires or screws only, and considerably lower than FCA utilizing plating technique.
There were 2 cases that required revision surgery (9.5%) for nonunion and fracture through previous fusion mass. None (0%) of these cases went on to require wrist arthrodesis, however. Conversion to wrist arthrodesis following FCA is varied in the literature; Saltzman et al 4 reported a 10% conversion rate, while Mulford et al 11 reports 2.9%. One ten-year follow-up of FCA reports one out of 15 cases to have converted to wrist arthrodesis (6.7%). 6 Additionally, a large database study reported conversion rates to wrist arthrodesis from FCA to be 19.2%, and 4.9% of patients require repeat wrist arthrodesis procedures. 5 Complications following FCA include, in addition to nonunion, dorsal impingement (2.6%) and hardware problems necessitating removal (3.3%). 11 Our results demonstrated no complications related to hardware during the follow-up period.
There have been other limited intercarpal arthrodeses techniques described as an alternative to FCA, including variations of the bicolumnar arthrodesis, lunatocapitate arthrodesis with scaphoid excision, and capitolunate arthrodeses with or without triquetrum excision.7,9,10 Draeger et al 9 describe their technique of bicolumnar arthrodesis, which involves scaphoidectomy with antegrade headless screw fixation of the lunate-capitate and triquetrum-hamate-capitate joints. In a small series of 11 patients, they observed a mean 88 degrees of flexion-extension arc postoperatively (68% of the contralateral side), and postoperative grip strength was 97% of the contralateral side. 9 All of their cases achieved radiographic union between capitate-lunate and triquetrum-hamate joints. No cases required conversion to wrist arthrodesis, though one patient underwent subsequent capitolunate screw removal for proximal migration. 9 Abdelaziz et al 10 studied outcomes following scaphoid excision and lunatocapitate fusion with a headless retrograde screw and K-wire in a recent study. In a series of 15 patients, they found mean postoperative flexion-extension arc was 70.1 degrees and grip strength was 71.5% of the contralateral side. 10 There were 2 cases of nonunion (13.3%) requiring revision, which subsequently went on to union, and 3 cases of ulnar sided wrist pain presumably secondary to the authors not fusion or excising the triquetrum. 10 In a large systematic review of capitolunate arthrodeses, Dunn et al 7 report mean postoperative flexion-extension arc of 71.3 degrees, grip strength to improve by 34.2% from pre- to postoperatively, and a 96.3% union rate. Four of these patients (5%) underwent conversion to wrist arthrodesis, 6.25% required hardware removal, and 1.25% had revision surgery for bone grafting and arthrodesis. 7 In a recent study evaluating outcomes of bicolumnar versus 3 corner arthrodesis, Gauci et al 12 report bicolumnar arthrodeses result in greater longevity for wrists with type I lunates, but recommend against performing a bicolumnar fusion in patients with type II lunates. The specific indications for performing limited intercarpal arthrodeses have yet to be clearly defined and is an area for future study.
The outcomes following these limited intercarpal arthrodeses, in addition to our data, support these techniques as an alternative to FCA. The authors believe that the preservation of more native mechanics of the carpus with a bicolumnar fusion rather than a FCA lends to the favorable functional outcomes observed, like improved postoperative grip strength. This study supports that it may not be necessary to fuse additional joint spaces to obtain adequate fusion. A limited intercarpal arthrodesis achieves acceptable union rates, while the smaller surgical footprint may preserve more native biomechanics and inter-carpal relationships. With functional outcomes comparable to FCA and > 90% union rate, limited intercarpal arthrodeses offers an effective, simplified, and less extensive procedure for degenerative wrist arthritis than FCA.
There are limitations to this study, including the retrospective nature, which limited data collection including radial and ulnar wrist motion measurements and preoperative wrist range of motion and grip strength. This study also lacks patient-reported outcome scores, as they were not collected consistently at follow-up. This limited our data collection and analysis. Many patients were also lost to follow-up at this point, and thus we had to exclude those patients with limited follow-up. This study was not a direct comparison of this technique to FCA or other limited intercarpal arthrodeses procedures, so we cannot conclude if one technique is superior to the other for this condition. This leaves room for further, prospective studies comparing this technique to FCA or other intercarpal arthrodeses, and to include patient-reported outcome scores.
Our results support that this is an effective procedure for wrist arthritis that leads to comparable outcomes as FCA with low nonunion rates and no conversions to total wrist arthrodesis, as shown by greater than 5 year follow-up data. Limited intercarpal arthrodesis has been gaining more attention recently, and the literature shows similar outcomes as compared to FCA, but with the advantage of decreased surgical exposure, increased simplicity of the case, and possibly preservation of normal mechanics without the fusion of all 4 carpus. This opens the field up to future studies on this topic, as we offer a successful and promising alternative to the treatment of wrist arthritis.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this retrospective review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.