
Abstract
Keywords
Introduction
Carpal tunnel syndrome (CTS) is one of the most frequent compressive syndromes. It is defined by the compression and/or traction of the median nerve at the wrist level. 1 The estimated prevalence of CTS is between 4% and 5% of the population, especially between 40 and 60 years of age, 2 mainly in women (around 4 times more than men). 3
Among the treatments, median nerve decompression surgery is one of the most widely performed orthopedic procedures. 3 The surgery is aimed at decreasing intratunnel pressure and increasing carpal tunnel volume by sectioning the transverse carpal ligament (TCL). 4
Although quite safe, the treatment of CTS by sectioning the TCL is not exempt from complications. Some nerve branches may be damaged by the incision. 4
Even with the use of a minimally invasive technique, such as endoscopic, many patients report similar persistent pain, frequently leading them to the indiscriminate use of strong analgesic.5,6 These persistent pains may be caused by sectioning the TCL in a zone with numerous nerve endings.
Thus, the aim of this study is to identify and map the TCL nerve endings, serving as a guide for sectioning this structure in a zone with less nerve ending density.
Materials and Methods
The study was approved by the institutional research ethics committee (CAAE 37083120.3.0000.5054) and involved 10 hands/wrists obtained from fresh adult cadavers.
The inclusion criteria were cadavers whose ligament extraction was authorized by the family after reading and signing the informed consent form.
The exclusion criteria were signs of trauma and/or degenerative injury that could hinder TCL dissection, inflammatory disease, previous wrist infection, or surgery (determined by radiography and clinical history and confirmed during dissection). However, none of the cadavers initially selected were excluded according to the criteria established.
Dissection
A median incision was performed on the anterior surface of the wrist, with dieresis by planes, where the edges of the TCL were identified based primarily on the direction and thickness of its fibers. Insertions into the thenar or hypothenar muscles in the TCL were dissected and reflected far from the TCL.
Careful attention was used to identify and resect the consistent insertions of the TCL radially in the scaphoid and trapezium and ulnarly in the pisiform and hamate. The TCL was flipped from radial to ulnar and its edges identified with non-absorbable thread. Next, the carpal tunnel was inspected to ensure that the TCL was completely resected (Figure 1a).
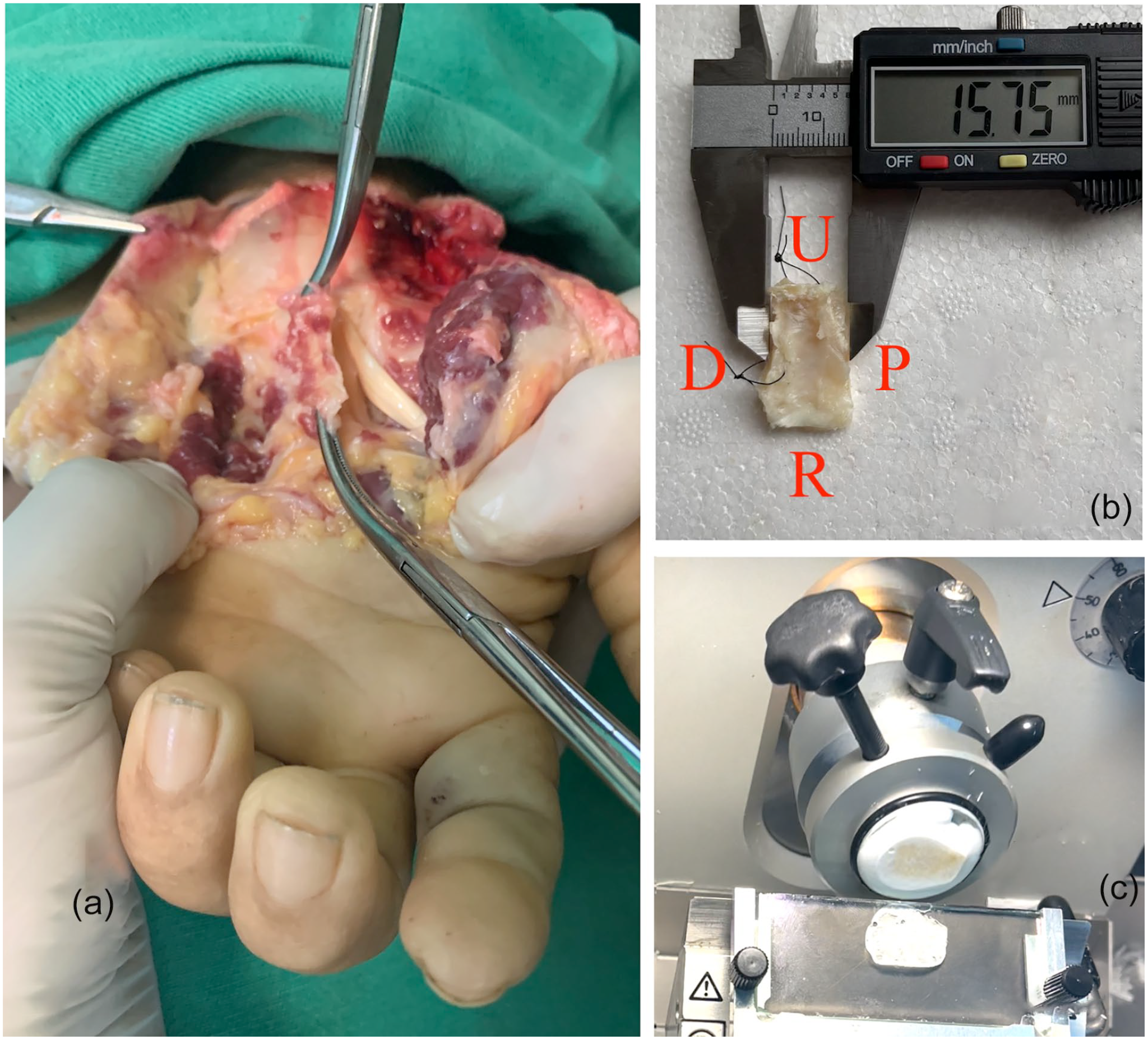
Transverse carpal ligament. (a) Dissection. (b) Measurement. (c) Cryostat sectioning.
With the TCLs resected, macroscopic measures of the ligament were taken, including length and width (Figure 1b). Each of the 10 TCLs was divided into 3 bands of equal width (three-thirds): radial, central, and ulnar.
The parts were immersed separately in a fixing solution of 4% paraformaldehyde in 0.1 M of phosphate buffer solution (PBS), pH: 7.4, at 4°C for 24 to 48 hours. The median nerve was also dissected to serve as stain control for the study.
Cryostat Section
After being fixed (24-48 hours), the ligaments were washed 4 times in 0.1-M PBS, pH: 7.4, at 4°C, followed by short washings and incubation in 0.1 M of PBS containing 20% sucrose buffer for cryoprotection. The tissues were prepared for sectioning in cryostat or stored at −70°C in 20% sucrose buffer for subsequent sectioning.
Each of the samples was placed on the support base for cryosectioning, aligned longitudinally in relation to the reference mark, and then fixed using Tissue-Tek O.C.T. compound solution (FR118 mL, Sakura-4583) as inclusion medium. The sections were cut using a Leica CM 1850 cryostat (Leica Microsystems, Nussloch, Germany), at a temperature between −18°C and −24°C, producing three 10-µm and three 50-µm sections for each ligament bands. All the sections were made in the longitudinal plane of the TCL bands. The sections calibrated into 10 µm were used for staining and the histological study with hematoxylin-eosin (HE). The 50-µm sections were arranged on the Immunoslide slides (Easypath) and reserved for immunofluorescence (Figure 1c).
Histology
The 10-µm sections were used to prepare the slides of each specimen of the study stained with Harris hematoxylin (Laborclin) and eosin yellowish (Inlab), for histological analysis, assessment of tissue integrity, and location of potential structures of interest, thereby serving as a reference for the study of immunofluorescence (Figure 2).
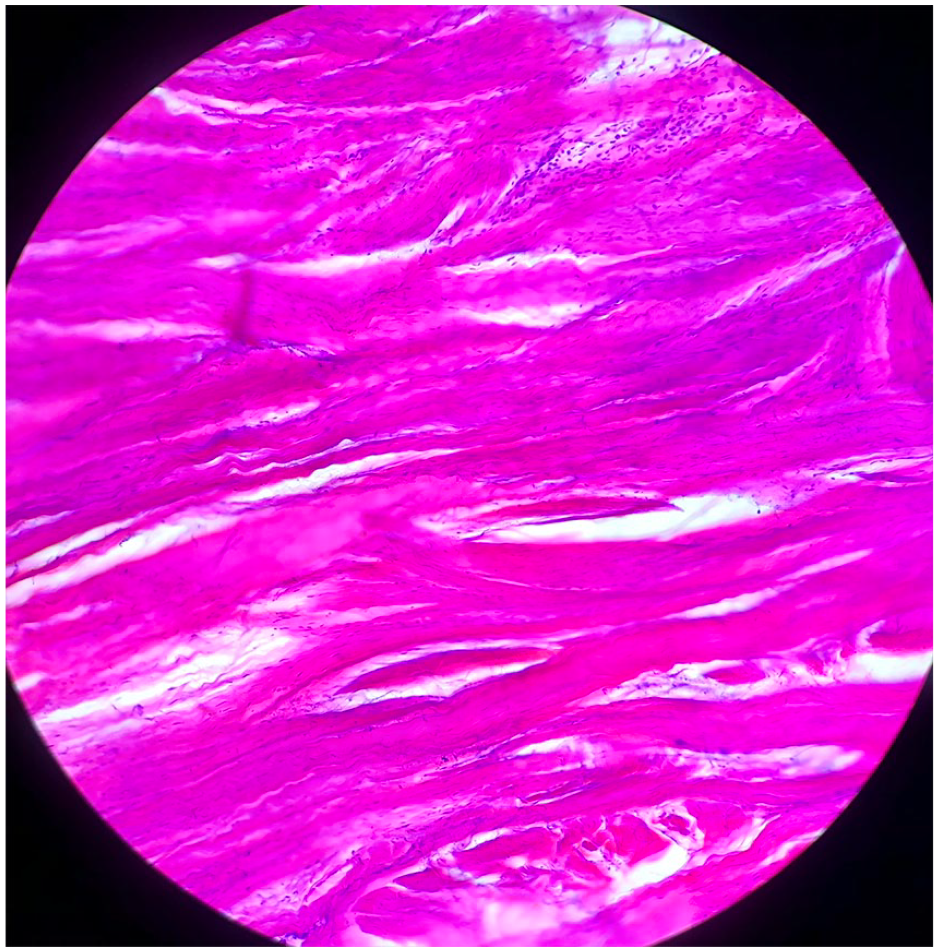
10-µm-thick longitudinal histological section of the transverse carpal ligament stained with hematoxylin-eosin.
Immunofluorescence
Slide preparation followed the method involving immunofluorescence with primary antibody protein gene product (PGP) 9.5 and secondary antibody Alexa Fluor 488, as proposed by Jew et al 7 and Ariel de Lima et al. 8
The slides were washed 4 times for 15 minutes each, with a cold PBS solution at 0.1 M containing 3% Triton X-100 (TX-100) (Inlab), followed by 2 hours of incubation at ambient temperature, with a blocking solution containing 4% normal goat serum (Jackson Immuno Research Inc), 0.25% bovine serum albumin serum (Inlab), 2% TX-100, and 0.1-M PBS.
The tissues were then washed 4 times for 15 minutes each, with 0.1-M PBS and incubated with primary antibody for 18 to 20 hours at 4°C. The primary antibody used was protein gene product (PGP) 9.5 (Sigma-Aldrich Ltda), diluted at a concentration of 1:400 in a solution containing 0.5% TX-100 in 0.1-M PBS.
After incubation with the primary antibody, the tissues were washed again 4 times for 15 minutes each, with a 0.1-M solution of PBS. Next, the tissues were incubated, protected from light, for 2 hours at ambient temperature with the secondary antibody, fluorescent marker Alexa Fluor 488 (Thermo Fisher Scientific Inc), diluted to a concentration of 1:100 in the same solutions used for the primary antibody. Next, the last 4 washings were performed protected from light: twice with 0.1-M PBS for 10 minutes, once with 0.05-M PBS for 10 minutes, and once with distilled water. Finally, the slides with the stained tissues were covered with coverslips, using Fluoromount Aqueous Mounting Medium, (Sigma-Aldrich Ltda), a liquid medium used to mount coverslips that prevents photobleaching. The slides were then stored in cases at −70°C.
Confocal Microscopy
The slides were examined under a confocal Laser Scanning Microscope (LSM)-710 (Carl Zeiss Inc, Germany), initially with epifluorescence at 10X magnification to assess tissue orientation and map the structures of interest. When identified, 20X and 40X lenses were used to observe the details of these structures. Next, the microscope was set to laser scanning mode, with standard configurations for parameters such as excitation wavelength (488 nm), pinhole size, and resolution. Stacks of optical sections were then obtained in the scanning mode, controlled by LSM software (Kontron KS400 Image Analyzer Workstation; Carl Zeiss Inc, Thornwood, New York). The functions of LSM software were used to analyze the images in 2D and 3D (after reconstruction). This analysis provided quantitative data such as length and diameter, and qualitative such as mechanoreceptor classification.
Morphometric Analysis
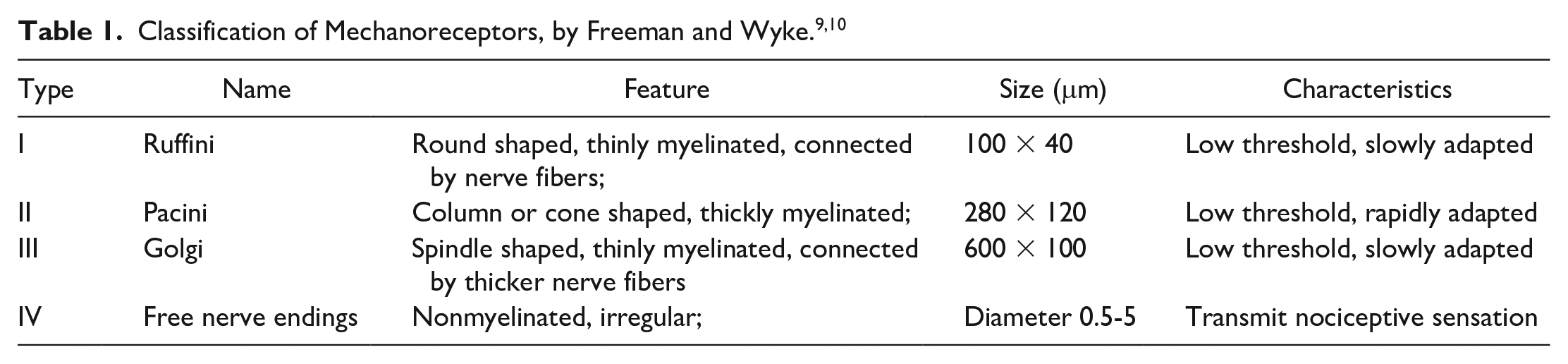
The nerve endings were classified according to Freeman and Wyke9,10 (Table 1). The TCL nerve fiber count was performed using the area fraction measurement function of ImageJ 1.52a.
Statistical Analysis
The quantitative variables were tabulated and analyzed in Statistical Package for the Social Sciences software (SPSS, v23), which provided measures of central tendency, percentile values, and dispersion.
Results
The average age of the cadavers was 47.4 ± 9.85 years (60% men and 40% women). In all the cases, the TCL exhibited consistent insertions in the scaphoid and trapezium radially and pisiform and hamate ulnarly. Morphologically, the TCL presents as an irregular parallelogram.
The relatively constant average width was 28.15 ± 1.18 mm. Average length in the longitudinal direction varied in the 3 bands studied: radial, central, and ulnar. The TCL was shorter in the central band, near the transition with the ulnar band (15.38 ± 0.58 mm), while radial and ulnar band lengths were 17.61 ± 0.65 and 16.16 ± 0.63 mm, respectively (Supplemental Table).
The histological sections in HE showed dense, well-organized collagen fibers, typical of a ligament structure (Figure 2). In all the specimens analyzed with immunofluorescence, type I mechanoreceptors (Ruffini) and free nerve endings (type IV) were identified (Figure 3 and Supplemental Video 1).
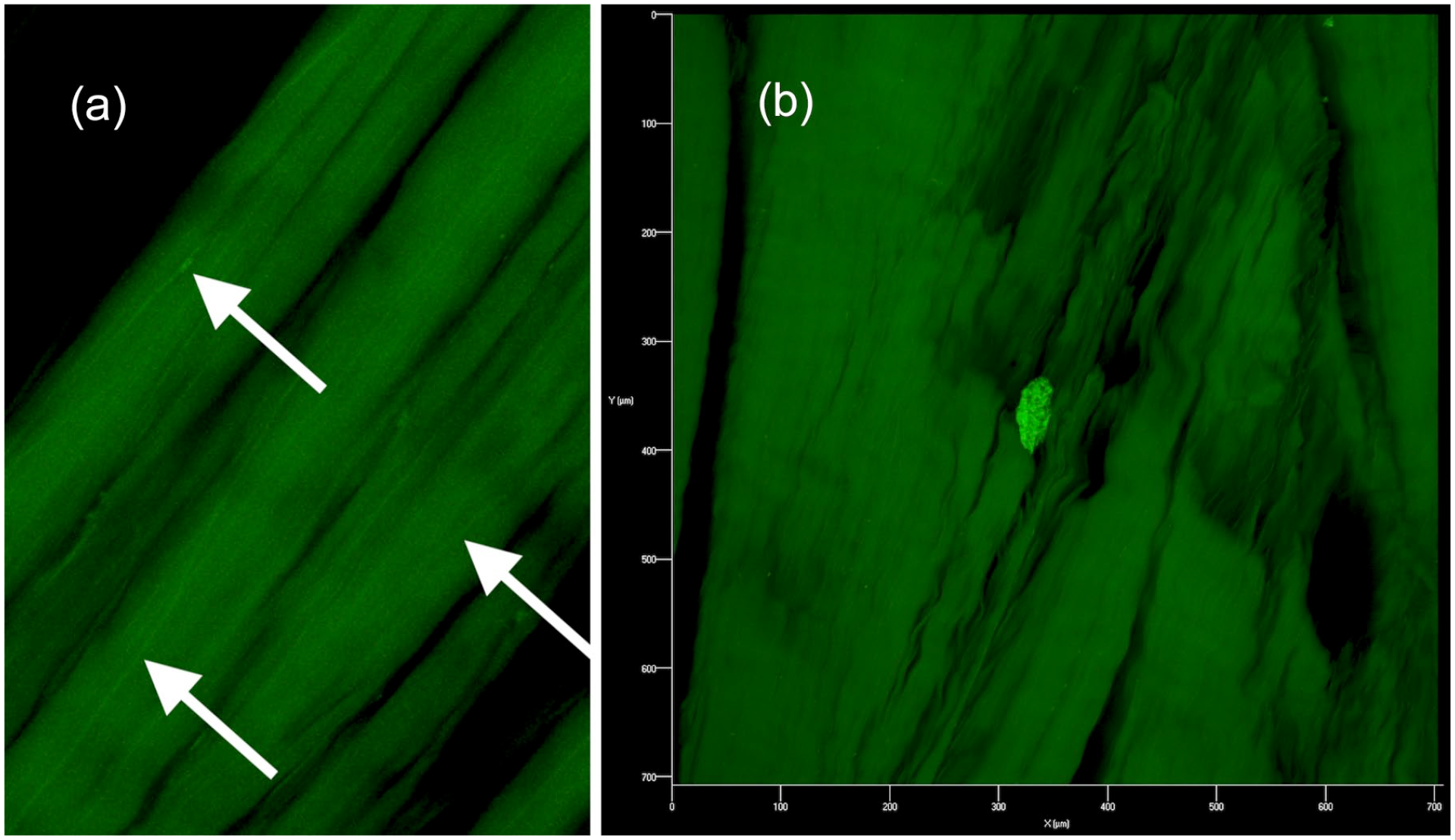
50-µm-thick longitudinal sections analyzed by confocal laser scanning microscopy. Immunofluorescence obtained with protein gene product 9.5 (PGP 9.5) marker as primary antibody and Alexa Fluor 488 as secondary antibody of the transverse carpal ligament. (a) White arrows indicate type IV (free nerve endings) mechanoreceptors, according to Freeman and Wyke.9,10 (b) Type I mechanoreceptors (Ruffini), according to Freeman and Wyke.9,10
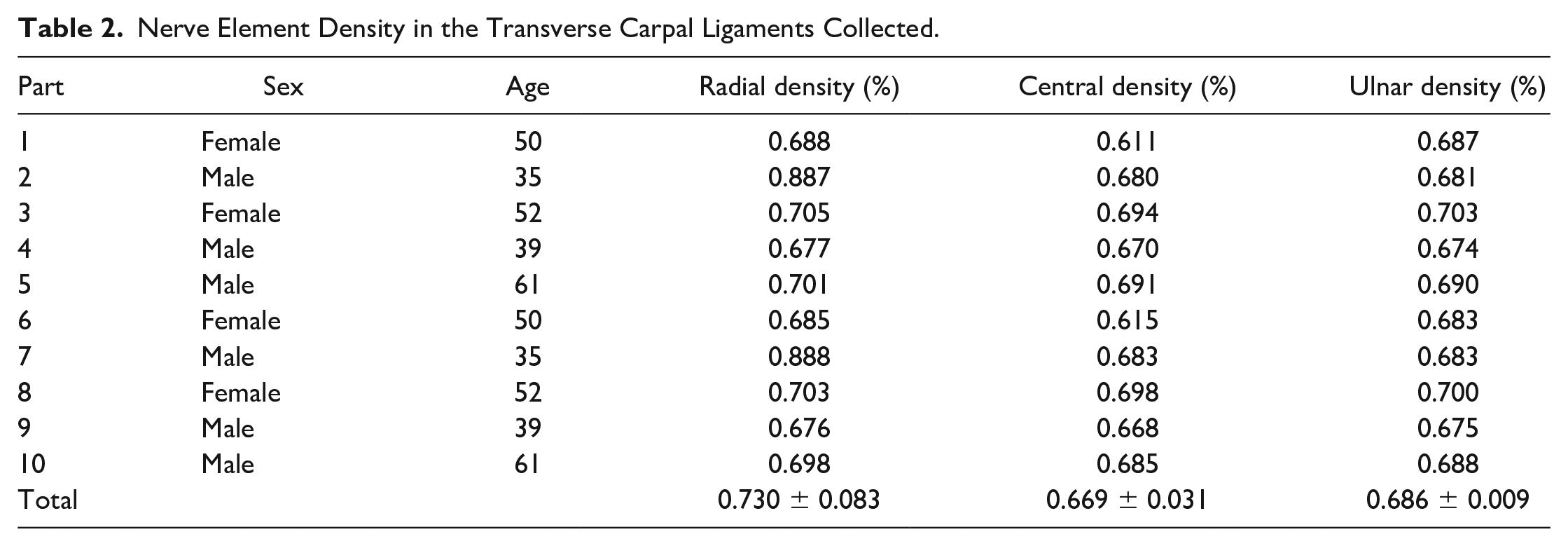
Neural elements, including free nerve endings and mechanoreceptors, occupy 0.695 ± 0.056% of the ligament area. When divided into bands (three-thirds), nerve element density was greater in the radial, followed by the ulnar and central, with 0.730 ± 0.083%, 0.686 ± 0.009%, and 0.669 ± 0.031%, respectively; Figure 4 and Table 2).
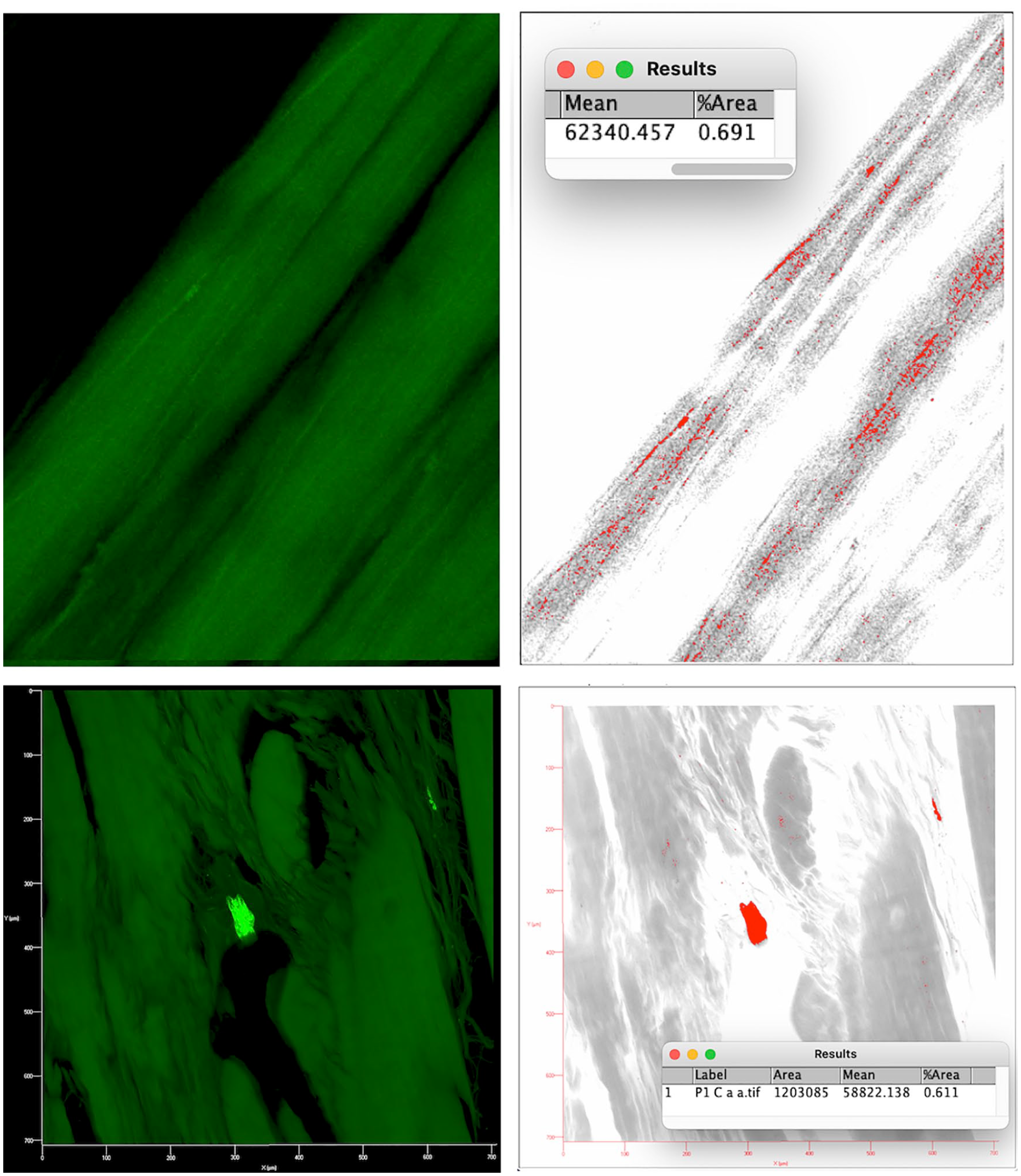
Nerve fiber count of the transverse carpal ligament using the area fraction measurement function of ImageJ 1.52a software.
Nerve Element Density in the Transverse Carpal Ligaments Collected.
The sections incubated without primary antibodies showed no immunoreactivity, confirming the specificity of the immunomarker.
Discussion
The main finding of this study was the mapping of nerve element density in the TCL, identifying the lowest density in the central portion. This mapping can be used to provide a possible route with fewer injured neural elements for TCL resection in CTS treatment. The presence of type I and IV mechanoreceptors was also found in the TCL.
Surgery to treat CTS has been performed for decades, generally involving TCL release to expand the volume of the carpal tunnel and decrease compression on the median nerve. Although it is a surgery performed frequently, only recently has the TCL been studied more rigorously, leading to better understanding of its anatomical complexity. 11
In some cases, TCL release surgery may fail, making it important to review this release for the treatment of persistent, recurring, or new symptoms. In a retrospective cohort study, Zieske et al 12 concluded that in revision surgeries, the symptoms were persistent in 43%, recurring in 20%, and new in 37%. In those with persistent or recurring symptoms, scarring between the median nerve and flexor retinaculum and incomplete TCL release were the most frequent findings. In patients with new symptoms, nerve damage was the most common, with nerve branches injured by the TCL incision standing out, resulting in painful neuromas.4,12,13
Theoretically, TCL sectioning in a zone with lower nerve ending density could decrease the incidence of complications from the treatment of CTS, avoid revision surgeries, and indiscriminate opioid use. 14 Mashoof et al 15 demonstrated the presence of neural elements in the TCL in 14 ligaments collected from fresh frozen cadavers. The tissues were stained with S-100 using the immunoperoxidase technique. The authors found an intraligamentous and extraligamentous neural network composed primarily of free nerve endings and Pacinian-like corpuscles. They also showed that neural innervation was present in the TCL, concluding that the nociceptive information transmitted by these neural elements may contribute to the pain associated with CTS.
In this study, mechanoreceptors were stained using immunofluorescence with primary antibody PGP 9.5. With the emergence of immunohistochemical and immunofluorescence techniques, the study of mechanoreceptors gained renewed interest16-18 after the first articles published by Freeman and Wyke.9,10 Many markers are used to study these nerve endings, such as antibodies for substance P, 19 P75, 20 calcitonin gene-related peptide, 21 S-100, 22 and neurofilament protein (NFP). 23 However, in addition to the technical peculiarities of each marker, several of them are not specific enough as neural markers and allow other tissues to be impregnated.7,24 As described by Jew et al 7 and Ariel de Lima et al, 8 PGP 9.5 (neural cytoplasmic protein, known as ubiquitin carboxyl-terminal hydrolase) has been successfully used in studies as a marker of nerves and nerve endings, a significant advantage of this protocol compared with others reported in the literature for nerve structures.
Divided into 3 bands (radial, central, and ulnar), the TCL exhibited the lowest neural element density in the central and highest in the radial. Corroborating this finding, Hagert and Mobargha, 20 in a review article, reported that mechanoreceptors in the wrist are found mainly near the ligament insertions because this provides the receptors with a fixed point from which they can feel changes in ligament tension. Manley et al 25 dissected cadavers and found strong TCL insertions in the scaphoid and trapezium radially and in the pisiform and hamate ulnarly.
Pacek et al, 26 using a silicone mold technique and digitization, studied TCL morphology in cadavers, constructing a 3D model of this ligament. The Pacek et al 26 divided the TCL longitudinally into 3 segments: radial, central, and ulnar and reported respective lengths of 16.5 ± 2.0, 14.4 ± 1.9, and 15.1 ± 2.6 mm, respectively. This study also demonstrated that the cross-section of the radial and ulnar segments was larger than that of its central counterpart. Pacek et al 26 found that the TCL was thicker distally in the central and ulnar segments and thicker proximally in the radial segment. That is, according to these authors, the thinnest zone of the TCL is an oblique line that longitudinally, from distal to proximal, is slightly inclined from radial to ulnar. Similarly to that described by Pacek et al, 26 this study divided the TCL into 3 longitudinal segments and also found that the central segment was shorter than the radial and ulnar segments.
Samarakoon et al 27 aimed to demonstrate a safety zone to decompress the carpal tunnel and recommended an incision in the TCL along the plane of the radial side of the ring finger. According to these authors, this could minimize inadvertent damage to the palmar branches and thenar of the median nerve, as well as the superficial palmar arch. Carmo 28 described a minimally invasive TCL release technique, reporting that the most indicated site for this release is the closest possible to the axis of the third webspace and not more than 10 mm distal to Kaplan line. According to Kim et al, 29 the reference for releasing is a line traced from the ulnar side to the middle finger. In view of the findings, we do not consider that an attempt to avoid the areas of the TCL with a high density of free nerve endings is justified if this increases the risk of inadvertent injury to nerve branches or the superficial palmar arch. However, if there is a safe area (with low nerve density and that does not increase the risk of inadvertent injury), it is better to use that safe area as a section area, hence another reason for a good mapping of nerve endings in the TCL.
As discussed above, the TCL is shorter longitudinally in the central third, near the transition with the ulnar third, has a smaller cross-section in the central band, and is thinner proximally and ulnarly. In this study, the findings suggest lower nerve element density in the central and ulnar thirds. Thus, it can be inferred that the central third region is the least prone to neural element injury during TCL release for the treatment of CTS, near the transition with the ulnar third, with the release from distal to proximal, and a slight inclination from radial to ulnar (Figure 5).
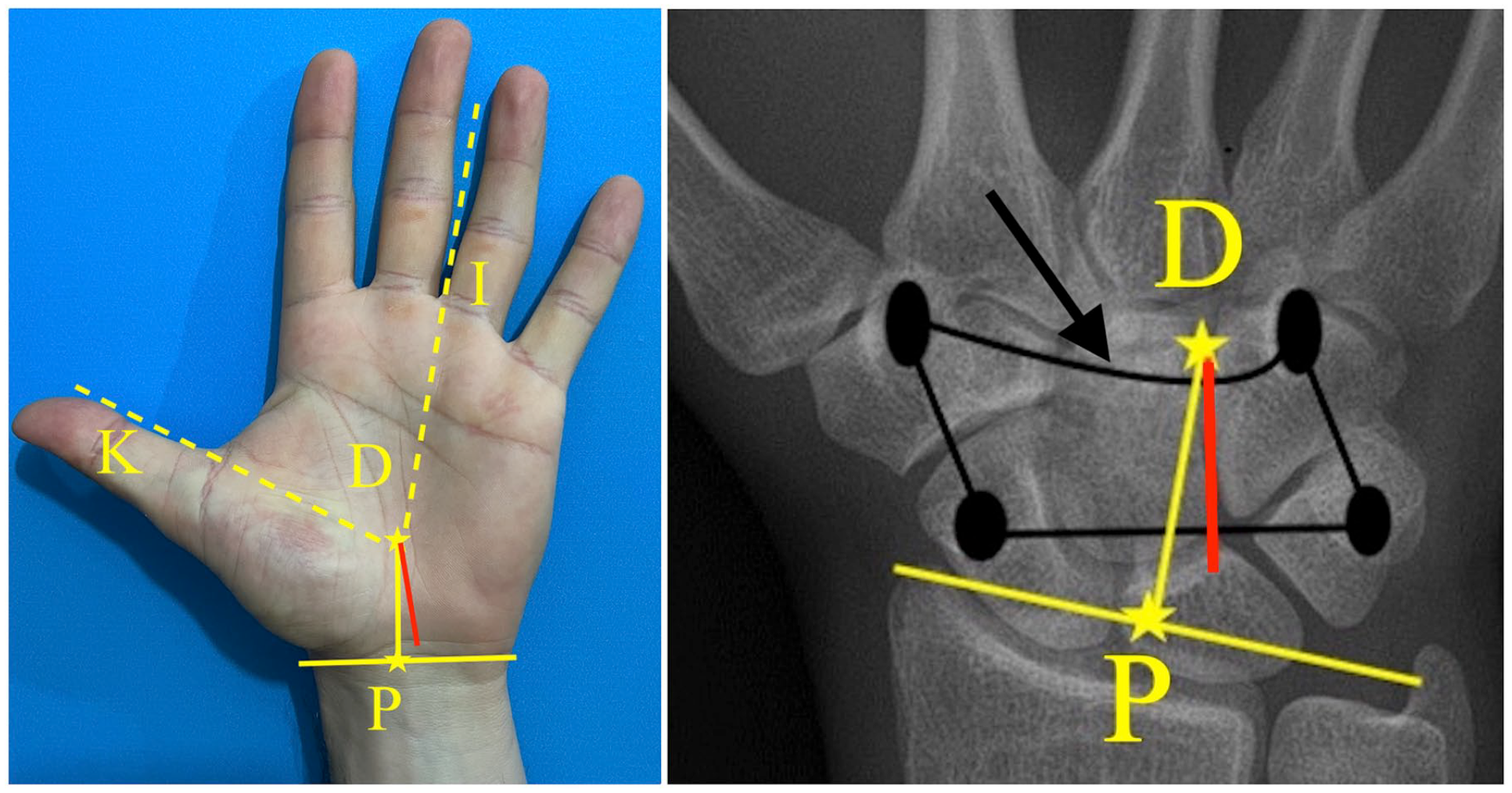
Topographic references for TCL release for the treatment of carpal tunnel syndrome with possibly less potential of compromising the nerve endings (red line).
Topographically, the proximal limit for release is the distal wrist crease. The distal limit is the intersection of Kaplan cardinal line and the axis of the third webspace. This distal limit aims to protect the superficial palmar arch, located 2 to 26 mm from the distal limit of the TCL. Kaplan cardinal line is an imaginary transverse line, starting at the deepest point of the first commissure, moving to the ulnar side of the hand, parallel to the proximal palmar crease 30 (Figure 5).
Limitations
The main limitation of this study was the number of ligaments studied. The COVID-19 pandemic and local laws hindered access to a large number of fresh cadavers, such that we only managed to obtain 5 specimens (10 wrists). However, based on similar studies in the literature, we believe that the sample used was sufficient to validate the conclusions. Regarding measurement failures, the correlation of TCL size with a measure of cadaveric limb size was not performed. Because the study was funded by the researchers themselves, another limiting factor was the cost of reagents, primarily PGP 9.5 and Alexa Fluor 488. Another limitation was the use of the Freeman and Wyke9,10 classification. Because this classification is old, it does not consider modern neuromarkers. In this study, type I (Ruffini) and IV (free nerve endings) mechanoreceptors were found in the substance of the TCL. Using staining for S-100, Mashoof et al 15 found no Ruffini endings. However, Hagert and Mobargha 20 reported that Ruffini endings are among the most prevalent mechanoreceptors in the wrist ligaments, constantly signaling the static articular positions of this joint. Finally, the lack of similar studies, especially on the staining technique and TCL innervation, made it difficult to interpret the results and select the ideal protocol.
Conclusion
The present findings suggest that the region with the least potential for neural element injury during TCL release is the central third near the transition with the ulnar third. When performed distally to proximally with a slight inclination from the radial to the ulnar, this release compromises the lowest nerve element density. Topographically, the proximal limit of the release is the distal wrist crease, while the distal limit is the intersection of Kaplan cardinal line and the axis of the third webspace (Figure 5).
Supplemental Material
sj-docx-1-han-10.1177_15589447211066974 – Supplemental material for Analysis of Mechanoreceptors and Free Nerve Endings of the Transverse Carpal Ligament
Supplemental material, sj-docx-1-han-10.1177_15589447211066974 for Analysis of Mechanoreceptors and Free Nerve Endings of the Transverse Carpal Ligament by Lana L. de Lima, Diego Ariel de Lima, Thiago H. B. Freire, Francisco A. A. Almeida, José A. D. Leite and Maria L. C. Cavalcante in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447211066974 – Supplemental material for Analysis of Mechanoreceptors and Free Nerve Endings of the Transverse Carpal Ligament
Supplemental material, sj-docx-2-han-10.1177_15589447211066974 for Analysis of Mechanoreceptors and Free Nerve Endings of the Transverse Carpal Ligament by Lana L. de Lima, Diego Ariel de Lima, Thiago H. B. Freire, Francisco A. A. Almeida, José A. D. Leite and Maria L. C. Cavalcante in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board (CAAE 37083120.3.0000.5054).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.