
Abstract
Background:
The purpose of this study was to determine the occurrence of patients undergoing primary trigger finger release (TFR) that underwent ulnar superficialis slip resection (USSR) for decompression and to determine which digit was most commonly affected.
Methods:
A retrospective chart review was conducted of all cases of open TFR performed by a single surgeon. The following data were obtained: age, sex, laterality, affected digit, and consideration for USSR. All patients failed nonoperative treatment of at least 1 steroid injection. The occurrence of patients who underwent TFR and USSR and which digit(s) most commonly underwent USSR were determined. The average patient age that underwent USSR, frequency by sex, and relative occurrence of USSR in each digit were computed. Statistical calculations were conducted using χ2 analysis (P < .05).
Results:
A total of 911 primary open TFRs were performed in 631 patients over a 16-year period. A total of 20 TFRs in 20 patients underwent USSR (2.2%). The long finger was the most commonly affected digit (40%) that required simple decompression. Within all USSR cases, the long finger was the most commonly affected digit. The index finger was the second most affected (30%), and there were no cases in the small finger.
Conclusions:
This study determined the occurrence of primary TFR cases that underwent USSR, with the long finger being the most commonly affected digit. Surgeons may consider this additional procedure to perform a larger decompression than simple A1 pulley release alone.
Keywords
Introduction
Stenosing tenosynovitis, or trigger finger, is a common disease process. The incidence of trigger finger in the general population ranges from 2% to 3% and affects women up to 6 times more frequently than men.1,2 The incidence increases in patients with rheumatoid arthritis and diabetes ranging from 10% to 42%.3-6 Initial treatment consists of splinting and/or corticosteroid injections at the level of the A1 pulley. After failure of nonoperative management, open trigger finger release (TFR) is usually recommended and is considered by most surgeons to be a minor procedure with a small but variable complication rate. Surgery typically involves complete release of A1 and palmar pulleys while avoiding injury to the critical A2 pulley. One known complication is persistent or recurrent triggering, which is thought to be higher among patients with rheumatoid arthritis and diabetes.2,7 It is unclear why these patients tend to have higher recurrence rates. Recurrent or persistent triggering may be due to several etiologies, including incomplete surgical release or masses within the retinacular system. Triggering may also lead to the development of a stiff proximal interphalangeal (PIP) joint with a flexion contracture.7,8 Triggering has also been proposed to develop secondary to chronic repetitive friction with progressive formation of an intratendinous nodule within the flexor digitorum profundus (FDP) tendon, although this hypothesis remains unproven in the literature. 9 In such cases, tendon debridement and/or partial excision can be considered during the index procedure as, in the author’s experience, it can consistently resolve intraoperative and potentially postoperative triggering after simple A1 release.
Occasionally, triggering may persist after simple A1 pulley release as enlarged flexor tendons continue to catch underneath the A2 pulley and/or at Camper’s chiasm. These patients have a size mismatch between the digital flexor tendons and the overlying pulley. In this instance, resection of the ulnar slip of the flexor digitorum superficialis (FDS) may be used to allow for smooth and unrestricted excursion of the tendons underneath the A2 pulley. Le Viet et al 10 described ulnar slip of the superficialis resection (USSR) to be successful in reducing tendon “bulk” with no objective superficialis weakness postoperatively. The radial slip was preserved to prevent ulnar deviation of the flexor mechanism and the potential development of a swan neck deformity. These patients were found to have a fixed flexion deformity of the PIP joint due to a chronic trigger finger. Other indications for USSR, not included in our sample population, may include lack of full extension after A1 release, painful passive extension, a history of failed open TFR if simple complete A1 pulley release does not improve the finger’s motion, or if persistent triggering is apparent intraoperatively. This surgical technique creates a larger decompression within the flexor tendon sheath without meaningfully sacrificing the function of the FDS tendon. 11
Although USSR has been described as a useful procedure in patients with diabetes and rheumatoid arthritis, the reported occurrence of patients who undergo this additional intervention at the time of primary TFR is lacking. The purpose of this study was to investigate the occurrence of patients who underwent resection of the ulnar slip of the FDS during primary open TFR and to determine which digits were most commonly affected.
Methods
A retrospective chart review was conducted for all cases of open TFR performed by a single surgeon from January 2003 to January 2019. All patients had failed an initial course of nonoperative management of at least 1 steroid injection and/or splinting. Patients with congenital trigger fingers (age <18 years), trigger thumbs, triggering due to partial tendon lacerations, prior trigger finger surgery in that digit, or incomplete data were excluded from the study. No patients were found to have a PIP contracture preoperatively. A heightened awareness for USSR was identified preoperatively on select patients. These patients had typical triggering underneath the A1 pulley and additionally appeared to trigger or “double click” under the A2 pulley (Supplemental Video 1). These patients were counseled about the possible need for excision of the ulnar slip of the FDS tendon. Fortunately, many of the patients who had this finding preoperatively responded successfully with a simple A1 pulley release.
The operative note was used to gather information on the specific procedures performed. The following data were obtained: patient age at index procedure, sex, laterality, affected digit(s), and the need for USSR. Approval for this project was obtained from the institutional review board of our institution.
Surgical Technique
For all TFR patients, a local or regional anesthetic was administered. Most typically, this involved a digital block placed just proximal to the distal palmar crease using 2% plain lidocaine. In select patients where more than 3 TFRs were being performed simultaneously or the TFR was combined with other more proximal procedures, a wrist block was used often with ultrasound guidance (median and/or ulnar nerve block at the distal wrist using 2% plain lidocaine). In this way, the patient was still able to perform active range of motion to confirm a complete decompression. A nonsterile tourniquet was applied proximally, and the affected extremity was prepped and draped in a standard surgical fashion. Longitudinal incisions were used directly over the A1 pulley unless an USSR was thought to be useful as determined by preoperative physical examination. In these instances, an angled incision was thereby used more easily, allowing distal extension of the incision if necessary.
The flexor sheath was exposed being careful to protect the neurovascular bundles on either side of the often fibrotic flexor sheath. The A1 pulley and palmar aponeurosis were released in their entirety being careful to not injure the critical A2 pulley. A flexor tenosynovectomy was performed if tenosynovitis was present. Once the aforementioned releases were performed, patients were asked to actively flex and extend the digit from full extension to full flexion while wide awake. Care was taken to note the size of the superficialis and profundus tendons. If triggering or locking was still present, we elected to proceed with an USSR.
The metacarpophalangeal (MCP) and PIP joints were maximally flexed, and the FDS tendon was withdrawn through the wound by placing traction on it proximally with the aid of a Ragnell retractor. The ulnar slip of the FDS was sharply incised as distally as possible, typically at the distal level of Camper’s chiasm (Figure 1). Next, using a tongue depressor and #10 scalpel, the slip was then incised proximally in a beveled fashion to allow for smooth, unimpeded excursion (Figure 2). Patients were then retested to ensure frictionless excursion of the flexor tendons. If there was persistent catching or triggering, the incision was extended. If an angled incision was made initially, this was simply extended in a Bruner fashion. If a standard longitudinal incision was initially made, a separate angled incision was made distally that was centered over the PIP flexion crease. The subcutaneous tissues were divided, and care was taken to identify and protect both neurovascular bundles. A window between the A2 and A4 pulley was made, and the flexor tendons were reevaluated. The very distal ulnar slip was then resected and the patient was retested. The skin was closed with 5-0 nylon, and a sterile bandage was applied trying to allow for as much unimpeded motion as possible and yet still cover the surgical site.
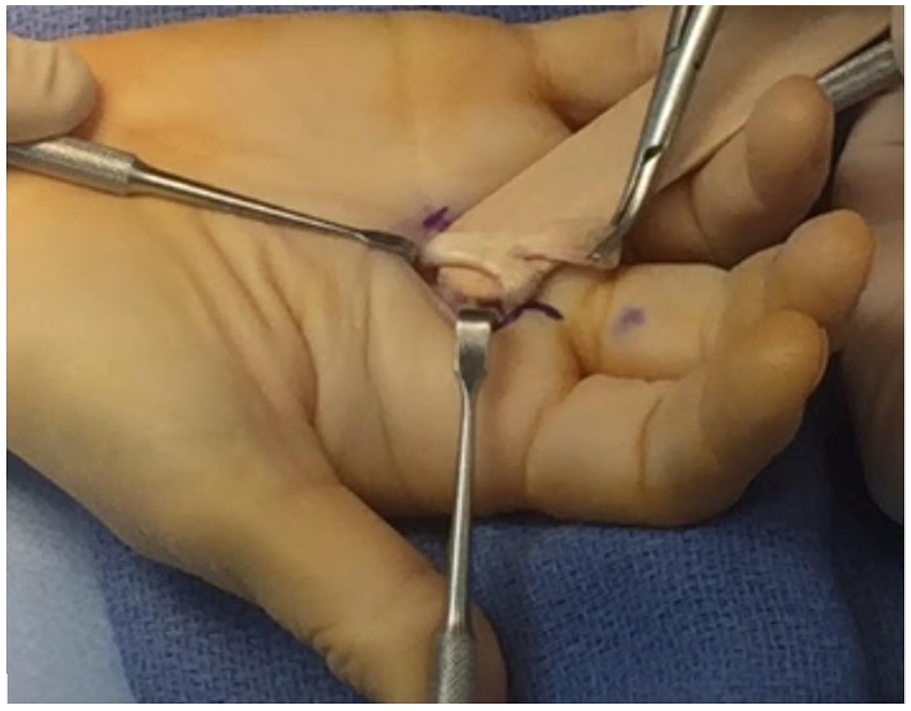
Intraoperative photograph of the ulnar slip of the flexor digitorum superficialis demonstrating that flexion of the metacarpophalangeal and proximal interphalangeal joints allows for the distal aspect of the ulnar slip to be reached without extending the incision too distally.
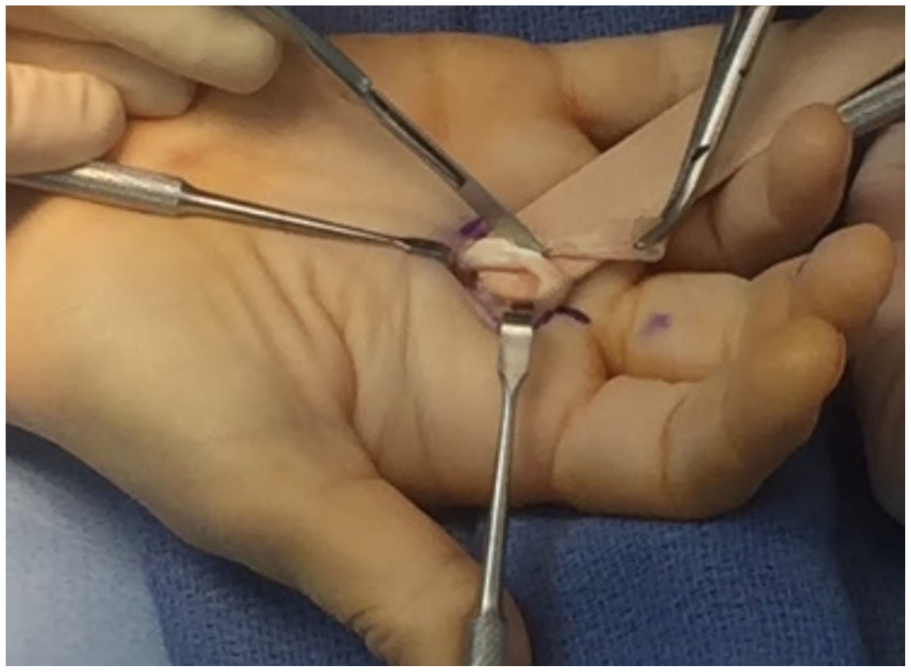
Intraoperative photograph demonstrating excision of the degenerative ulnar slip of the flexor digitorum superficialis.
The overall occurrence of patients with trigger finger that underwent primary TFR and USSR in this adult population was determined as well as which digit was most commonly affected. The average age of patients who underwent USSR, the frequency by sex, and the relative occurrence of USSR in each digit were also computed.
Statistical methods
Statistical calculations were conducted using χ2 analysis. A significance level of .05 was used. A χ2 test of independence was performed to determine which digit most frequently underwent USSR.
Results
A total of 911 primary open TFRs were performed in 631 patients over a 16-year period (Figure 3). Patients requiring simple decompression consisted of 348 women (55%) and 283 men (45%). The average age of patients requiring simple decompression was 60 ± 12 years, compared with an average age of 64 ± 7 years for patients who underwent USSR (Table 1). The long finger was the most commonly affected digit that underwent simple TFR (40%) (P < .05). When stratified by sex, the average age of patients who underwent USSR was 62 ± 9 years for men and 64 ± 5 years for women. None of these patients required revision TFR or USSR for recurrent triggering or flexion contractures.
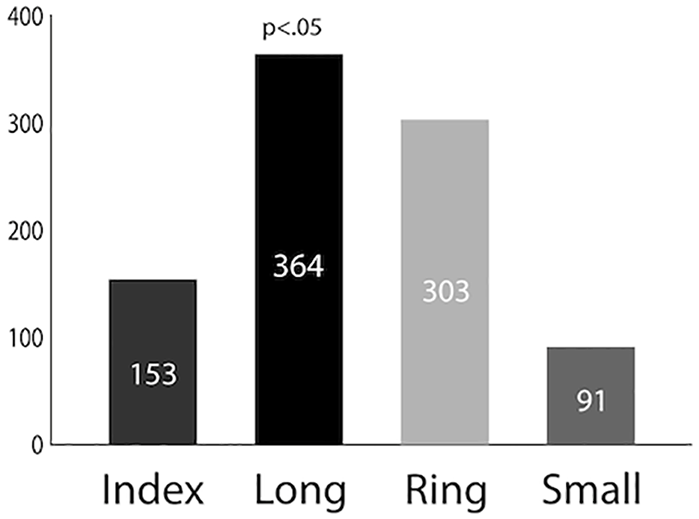
The frequency of trigger finger release cases in each digit.
The Distribution of Cases by Surgical Intervention, Age, and Sex.
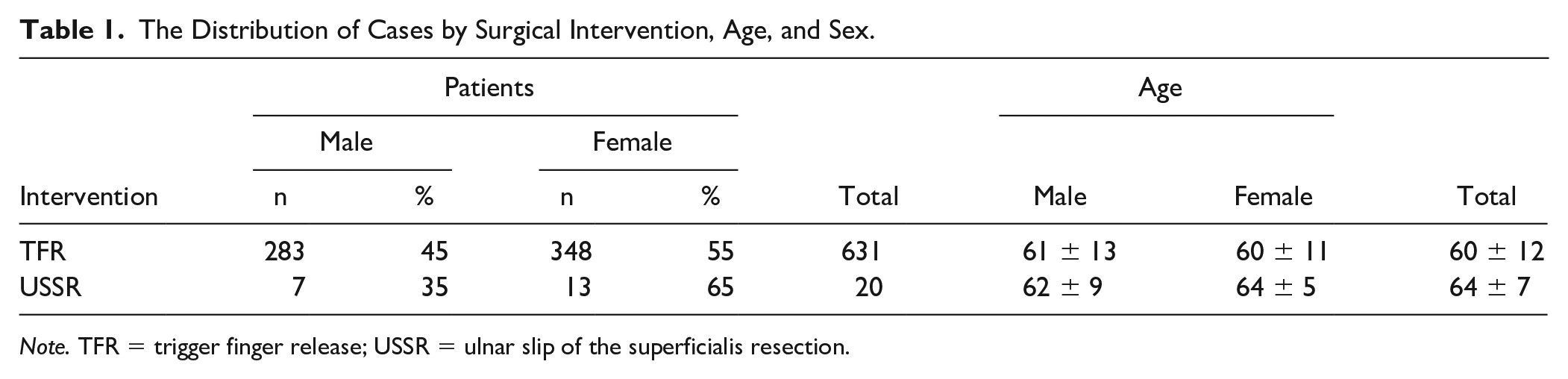
Note. TFR = trigger finger release; USSR = ulnar slip of the superficialis resection.
A total of 20 TFRs in 20 patients underwent USSR, accounting for 2.20% of all trigger finger cases (Table 2). Of the total USSR cases, 65% (n = 13) were performed in female patients and 35% (n = 7) in male patients (P < .05). The long finger was the most commonly affected digit that underwent USSR and comprised 55% (n = 11) of the total USSR cases (Figure 4). The long finger was significantly more likely to undergo USSR when compared with the other digits (P < .05). The index finger was the second most affected digit (30%), and the ring finger accounted for the final 15% of USSR cases. No TFR cases in the small finger underwent USSR.
The Distribution of Trigger Finger Release and Ulnar Slip of the Superficialis Resection Cases per Digit.
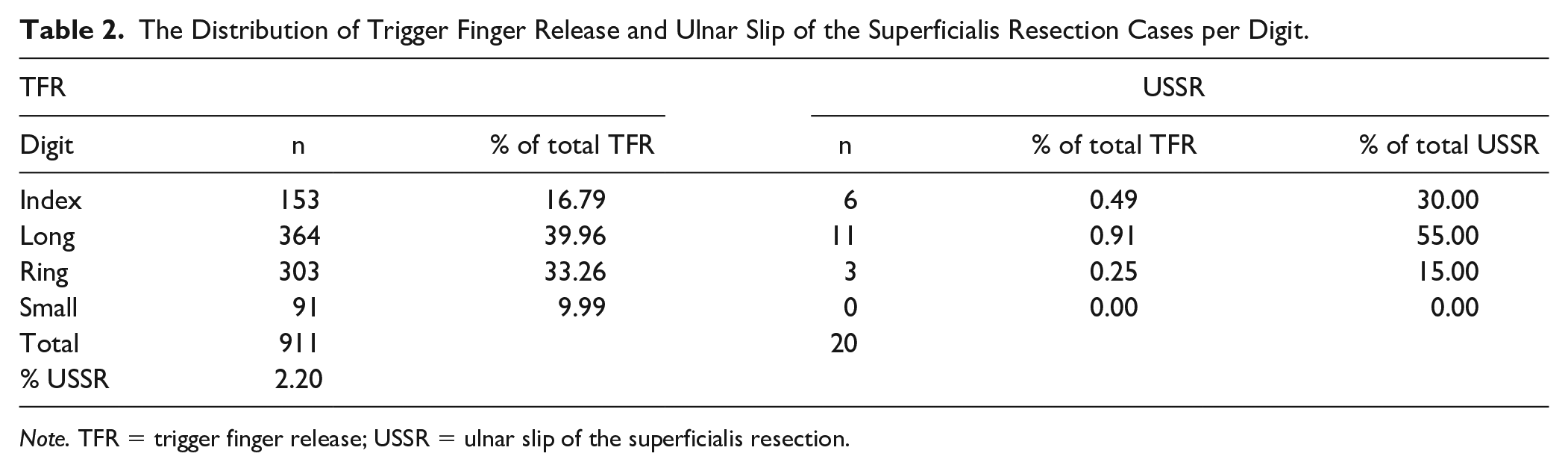
Note. TFR = trigger finger release; USSR = ulnar slip of the superficialis resection.
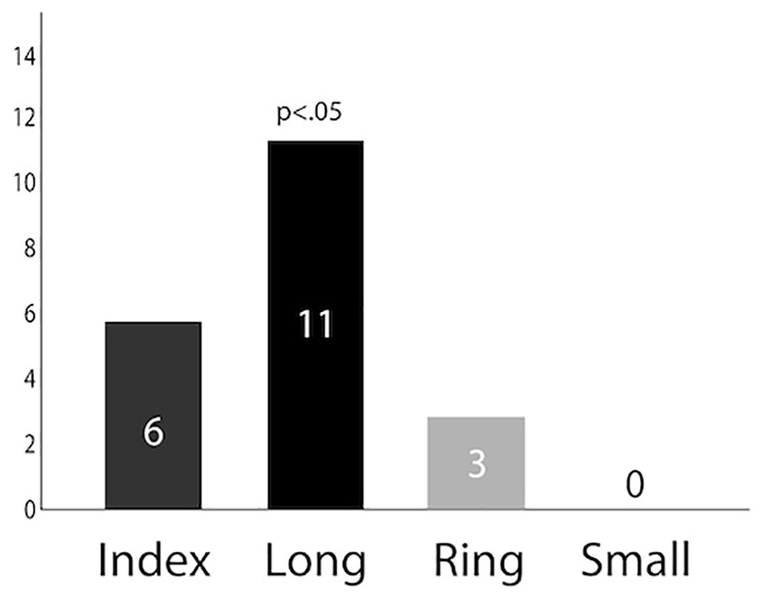
The frequency of trigger finger release cases that underwent additional ulnar slip of the superficialis resection in each digit.
Discussion
The excision of the ulnar slip of the FDS tendon in the setting of persistent or recurrent triggering after A1 release has been a suggested form of treatment in the more complex trigger finger patient undergoing primary TFR.7,8,10,11 However, there is a paucity of literature on the occurrence of USSR in these patients and which fingers are more commonly affected. Our study demonstrated that the long finger was the most common digit that underwent USSR. It is unclear why the long finger was the most common. One reason for this may be that patients with long finger triggering often have a delayed presentation when compared with other fingers. In the author’s experience, delayed presentation of trigger finger can lead to the development of significant tendon thickening, which is often seen intraoperatively. 12 A simple, complete A1 pulley release may not be enough to resolve the patient’s symptoms, as demonstrated with persistent triggering intraoperatively upon active finger flexion. Similarly, Favre and Kinnen 8 examined patients with long-standing trigger finger or previously failed A1 pulley release with an associated positional contracture of the PIP joint with the middle finger as the most commonly affected digit (67%). After TFR, all patients continued to lack full extension in the affected joint, but regained motion after subsequent excision of the ulnar slip of the FDS tendon. Although PIP joint contracture was not one of the indications examined in our sample population, this study demonstrates another potential indication for USSR in the complex trigger finger.
In addition, there were no incidences of USSR in the small finger. The lack of USSR cases in the small finger was an unexpected finding. This may be explained by the often found small and sometimes incompetent FDS slips seen when performing standard TFRs. In fact, up to 21% of patients can have an incompetent or absent FDS to the small finger. 13 No intratendinous nodules or other anatomical variants were noted. An intratendinous nodule would create a mass effect similar to the pathology encounter in a trigger finger in the pediatric population. 14
Numerous techniques have been described to perform excision of the ulnar slip of the FDS. Le Viet et al 10 initially described a technique of distal sectioning with proximal retrieval followed by resection of the ulnar slip. The extensive approach allows for complete visualization of the FDS from proximal to distal. Marcus et al 7 describe a 2-incision technique starting with an oblique incision distal to the transverse palmar crease to release the A1 pulley and a second V-shaped incision over the proximal phalanx and the flexor sheath and tendon distal to the A2 pulley. In a series of rheumatic patients, Ween et al 2 describe 2 discontinuous, extensile incisions over the middle to proximal phalanges and at the mid palm. One of the disadvantages of these techniques is that the larger incisions extend from the proximal palmar crease into the digit, which carry a higher risk of postoperative scarring and loss of motion as unimpeded postoperative range of motion becomes difficult. Extensive releases also potentially increase the risk of injury to the critical A2 pulley. 8 In our series of USSR patients, we routinely were able to decompress the flexor sheath and perform an USSR through a palmar incision alone. We have found that with hyperflexion of the MCP and PIP joints, the distal aspect of the ulnar slip can be reached, a modification which allowed for a substantially smaller incision for USSR than what has been previously described.
Limitations
There are several limitations to the study. Although we had an adequate sample size of patients who underwent primary TFR, our subset of patients who underwent USSR was relatively small. Therefore, we were unable to perform a substantial statistical analysis other than a χ2 analysis to determine relative occurrences in each digit. Second, we did not stratify our patients according to the comorbidities. While the incidence of USSR is higher in patients with diabetes and rheumatoid arthritis, we did not separate the TFR and USSR groups based on these systemic disorders. The study may be susceptible to confounding bias if the USSR group was more likely to have a systemic disorder compared with the TFR group. It is also possible that the patients who underwent simple TFR later required USSR at another institution, a finding which would increase the occurrence of USSR. However, none of our patients who underwent simple TFR returned for revision TFR or later USSR at our institution. Conversely, it is possible that patients who underwent TFR and USSR could have experienced eventual resolution of triggering in the postoperative period even if primary USSR was not performed, which would artificially increase the occurrence of USSR. While this may be a possibility, we elected for further decompression because continued triggering was identified intraoperatively even after simple TFR. Finally, we do not have range of motion comparisons between the typical TFR and USSR groups nor do we have long-term data for comparison (Supplemental Video 2). Despite these limitations, our study presents a large cohort of patients with trigger finger with a subset that also underwent USSR.
This study determined the occurrence of primary open TFRs that underwent additional excision of the ulnar slip of the FDS tendon. In our series, 2.2% of cases of primary TFR underwent ulnar slip of the superficialis resection, with the long finger being the most commonly affected digit (>50%). Surgeons should be aware of this finding and have the option of performing an USSR in their armamentarium. This can potentially minimize postoperative complications such as persistent triggering, stiffness, and pain, although further research is required to confirm this notion. Because the long finger was found to be the most commonly affected digit, surgeons should have a heightened awareness of this and can consider performing long finger TFR under wide-awake anesthesia when possible. This may help resolve any persistent triggering intraoperatively after complete release of the A1 pulley. Further studies are needed to assess the anatomical differences and variations of both slips of the FDS tendon of each digit and the cross-sectional size needed to create triggering at Camper’s chiasm or underneath the A2 pulley. Long-term follow-up data are also needed to compare the final range of motion, outcome, and strength of traditional TFR patients with USSR patients.
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval for this study was waived by Northwell Health Institutional Review Board because of the retrospective and patient deidentified collection of surgical records.
Statement of Informed Consent
Informed consent was not sought for this study because of the retrospective and patient deidentified collection of surgical records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.