
Abstract
Background:
Fellowship directors (FDs) influence the future of trainees in the field of hand surgery. Currently, there are no studies that analyze the demographic background, institutional training, and academic experience of hand surgery FDs. This study aims to serve as a framework to understand the landscape of current leadership positions in hand surgery education and to identify opportunities to improve FD diversity.
Methods:
The American Society for Surgery of the Hand Fellowship Directory was reviewed to include all hand surgery fellowships in the United States. Collected demographic information regarding FDs included age, sex, ethnicity, residency/fellowship training, residency/fellowship graduation year, year hired by current institution, time since training completion until FD appointment, length in FD role, and H-index.
Results:
Of the 90 FDs included, 86.7% were men and 71.4% self-reported as Caucasian. The average H-index was 13.98 and significantly correlated with age and duration as FD; 71.1% of FDs were trained in orthopedic surgery. The most attended residency program was the University of Pennsylvania; Mayo Clinic and Harvard University were the most represented fellowship programs.
Conclusion:
This review reveals specific trends in demographic backgrounds, institutional training, and academic experiences among current FDs in hand surgery. Our observations, such as racial/ethnic and sex disparities, may offer opportunities to improve the representation of the communities these physicians serve. In addition, the trends described in this study provide objective data among current hand surgery FDs and could serve as a guide for individuals who desire academic leadership roles.
Keywords
Introduction
Leaders in medicine exhibit unique characteristics that qualify them to serve in institutional roles that impact their respective fields. These individuals have acquired leadership skills through academic training, societal and community involvement, and extensive practical experience.
Within the field of hand surgery, one such leadership position is the role of fellowship director (FD). Fellowship directors significantly influence the future of developing surgeons. An evaluation of these individuals’ careers can reveal shared features of their training backgrounds that may have aided them in their pursuits of professional accomplishments. Identifying demographic and training backgrounds provides valuable information that may have previously gone unnoticed. Some studies have previously analyzed demographic trends of residency program directors and department chairs in other medical fields.1-4 Closer to the specialty of hand surgery, recent studies assessed these trends for orthopedic FDs.5-9
The purpose of our study was to provide a snapshot into the current landscape of leadership in hand surgery by reviewing the demographic and institutional training backgrounds, as well as academic productivity of the current hand surgery FDs in the United States. Overall, this study aims to serve as a framework for those aspiring to achieve such leadership positions in hand surgery and identify opportunities to improve the position, particularly regarding diversifying leaders’ racial, sex, training, and research backgrounds.
Methods and Materials
Data Collection
The American Society for Surgery of the Hand (ASSH) Hand Fellowship Directory for 2019 to 2020 was reviewed to incorporate all hand surgery fellowships in the United States. All programs included in the study were classified as either orthopedic surgery or plastic surgery hand fellowship programs. This study was performed in 2020.
For each program, all listed FDs were included. The demographic and educational background data for each FD were gathered via author review of current curriculum vitae (CVs) forwarded directly by FDs or their department coordinators. Any information that was unavailable on CV review was gathered from institutional biographies, Scopus, Web of Science, and e-mailed questionnaires sent to fellowship administrators. To ensure the collection of as many data points as possible, fellowship program coordinators, department offices, and FD were directly contacted via phone if there was no response via e-mail. The demographic information of interest for each FD included age, sex, race/ethnicity, former residency and fellowship training locations, the years of residency and fellowship graduations, year hired by current institution, time since residency and fellowship completion until FD appointment, length in FD role, and each individual’s H-index.
To obtain the individual H-index for each FD, the Scopus database (Elsevier BV, Waltham, Massachusetts) was queried to access their research specific information. This database has a search engine feature that operates through an extensive repository of peer-reviewed scientific literature with a citation tracking component. Scopus was employed to retrieve the H-index for every FD in the study.
Pearson correlation coefficients were determined via Statistical Analytics System (SAS 9.4) software. Data were interpreted according to Mukaka’s 10 guide for correlation coefficients. Values under 0.3, 0.3 to 0.5, 0.5 to 0.7, 0.7 to 0.9, and greater than 0.90 are indicative of negligible, low, moderate, high, and very high positive correlation, respectively.
Results
Of the 90 hand surgery fellowship programs listed in the ASSH database, 72 of them were designated as orthopedic surgery programs, while only 18 were considered plastic surgery programs. Designation of program specialty type was determined by authors using program descriptions available directly on the ASSH database, in addition to program-specific Web sites when appropriate. Demographic information including age, sex, and race/ethnicity was obtained for the 90 FDs (Table 1). Of the 90 FDs, 86.7% (n = 90) of the leadership was men. In addition, 62% (n = 56) of the FDs responded to the racial/ethnicity classification question. Of those who responded, 71.4% identified as Caucasian (n = 40), 21.4% identified as Asian or Asian-American (n = 12), 3.6% identified as Hispanic/Latino (n = 2), and 3.6% identified as Middle Eastern (n = 2). The mean age of current FDs was 55.2 years old (±9.9 years).
Demographics.
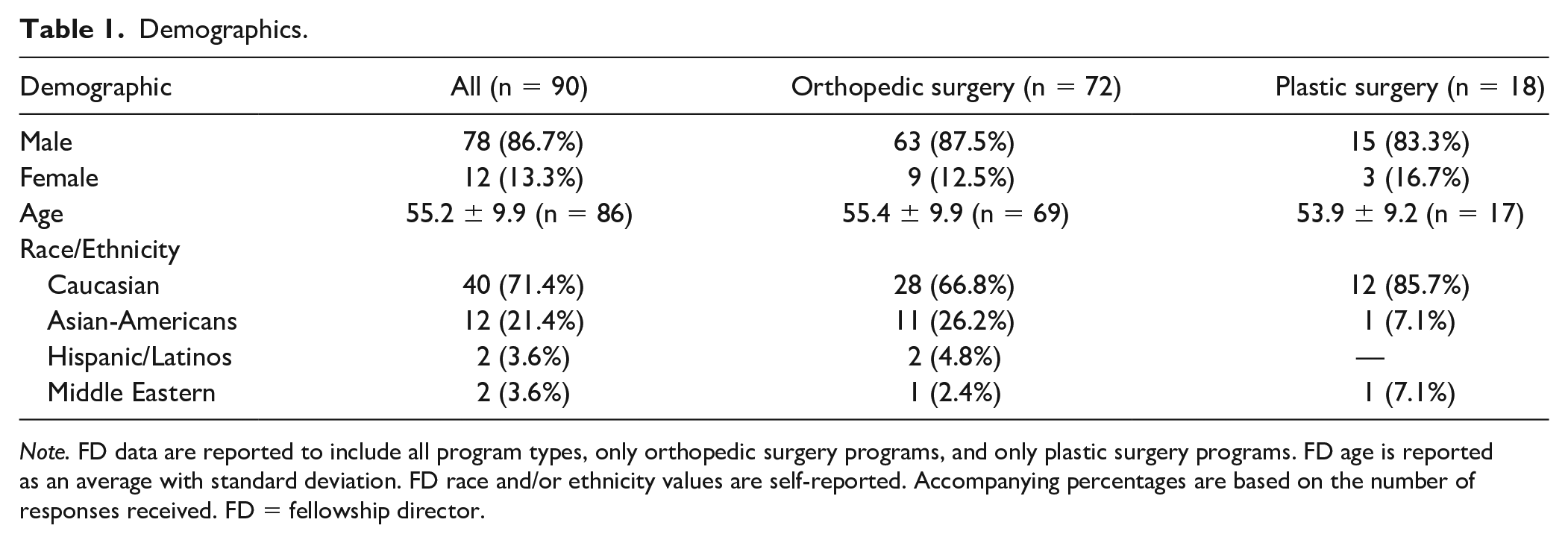
Note. FD data are reported to include all program types, only orthopedic surgery programs, and only plastic surgery programs. FD age is reported as an average with standard deviation. FD race and/or ethnicity values are self-reported. Accompanying percentages are based on the number of responses received. FD = fellowship director.
Detailed educational, employment, and leadership progressions of hand surgery FDs are presented in Table 2, including mean calendar years for completion of residency and fellowship training, mean duration from fellowship graduation until FD appointment, mean duration of employment for an FD at his/her current institution, mean duration that an FD has held his/her current position, and the average time from initial hire until FD appointment. Of note, the mean duration from fellowship graduation until FD appointment was 11.3 years (±8 years). Specifically, the mean duration of employment for an FD at his/her current institution was 17.1 years (±9.6 years) and the mean duration that an FD has held his/her current position was 11.0 years (±9.8 years). Table 2 also describes the percentages of FDs currently working at the same institution where they completed residency training, completed fellowship training, or completed both residency and fellowship training were included.
Education and Employment Progression.
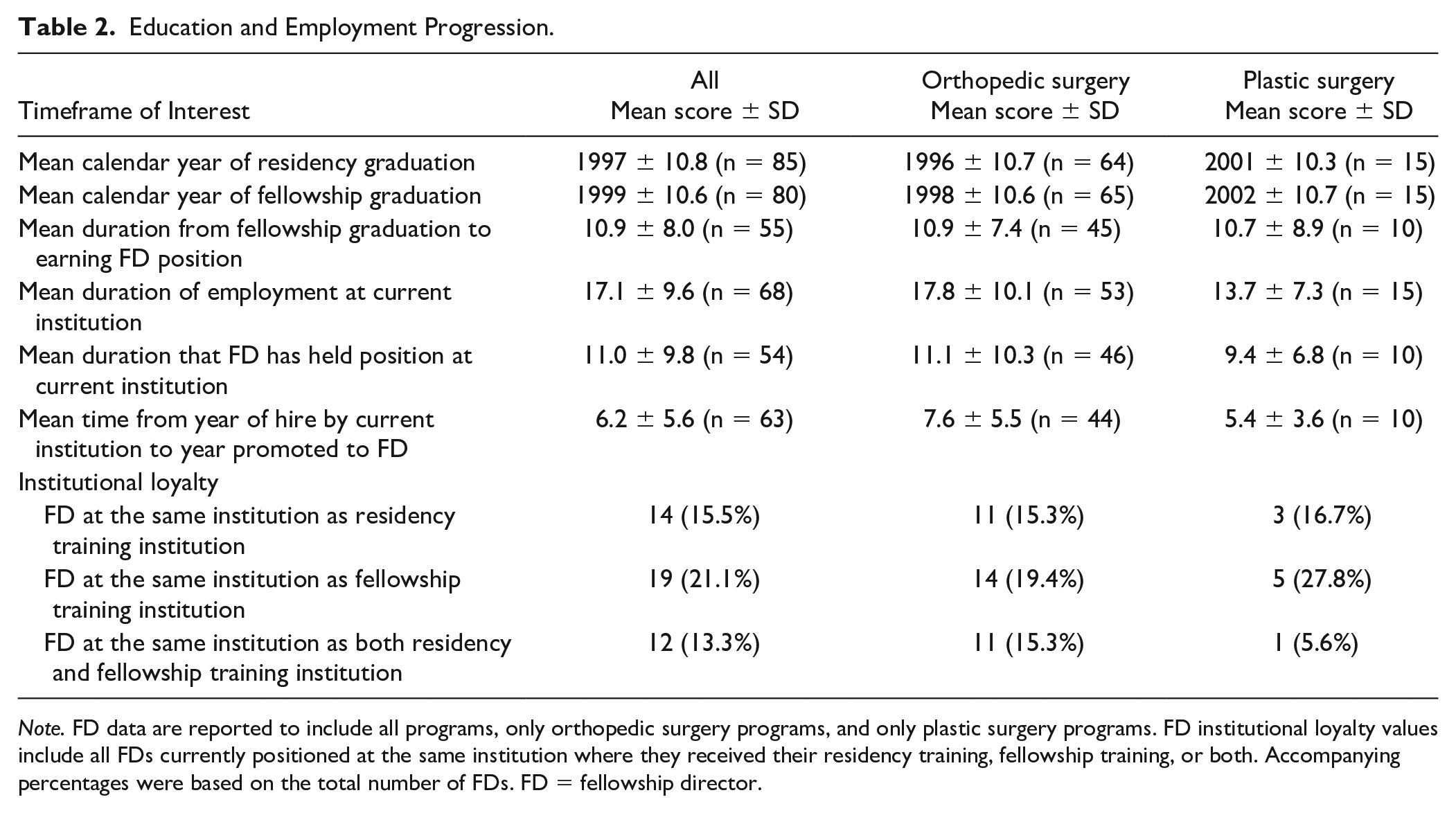
Note. FD data are reported to include all programs, only orthopedic surgery programs, and only plastic surgery programs. FD institutional loyalty values include all FDs currently positioned at the same institution where they received their residency training, fellowship training, or both. Accompanying percentages were based on the total number of FDs. FD = fellowship director.
Route of surgical specialty residency training showed that FDs were trained in orthopedic surgery, plastic surgery, both general surgery and orthopedic surgery, both general surgery and plastic surgery, or general surgery. This information is reported in Table 3. Research productivity, which was measured in the form of Scopus H-indices, and the correlations with years as FD and age are included in Table 3.
Training Backgrounds and Research Productivity.
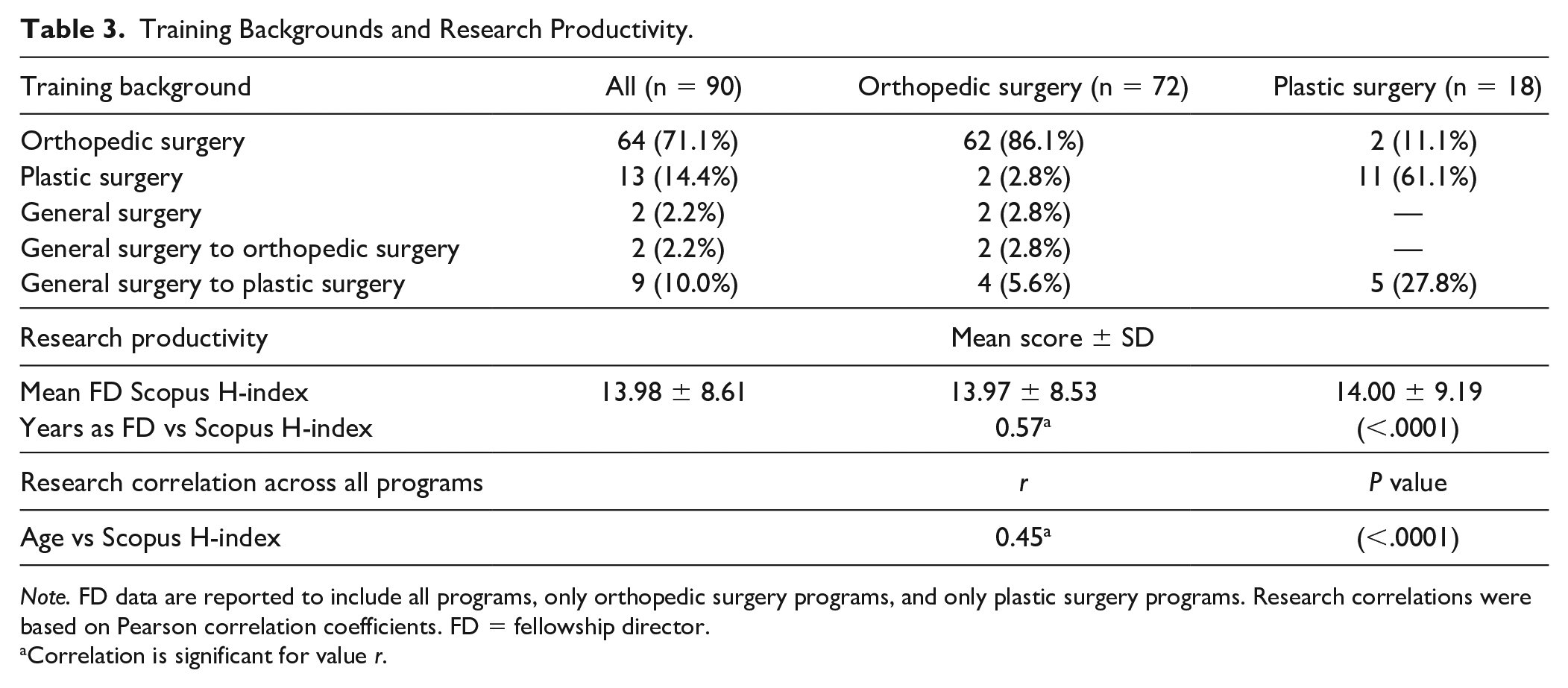
Note. FD data are reported to include all programs, only orthopedic surgery programs, and only plastic surgery programs. Research correlations were based on Pearson correlation coefficients. FD = fellowship director.
Correlation is significant for value r.
Figures 1 and 2 represent the most attended residency and fellowship training programs, respectively. Institutions with residency programs at which at least 3 FDs trained are included in Figure 1. Institution with fellowship programs at which at least 5 FDs trained are included in Figure 2. Orthopedic, plastic, and general surgery training programs were grouped together by institution. Notably, 20 FDs (22.2%) completed 2 fellowships. The most common additional fellowship training FDs received were in sports medicine, shoulder and elbow, and microsurgery. When completed consecutively and immediately after residency, the last fellowship training completed was consider as that individual’s year of completion of fellow training.
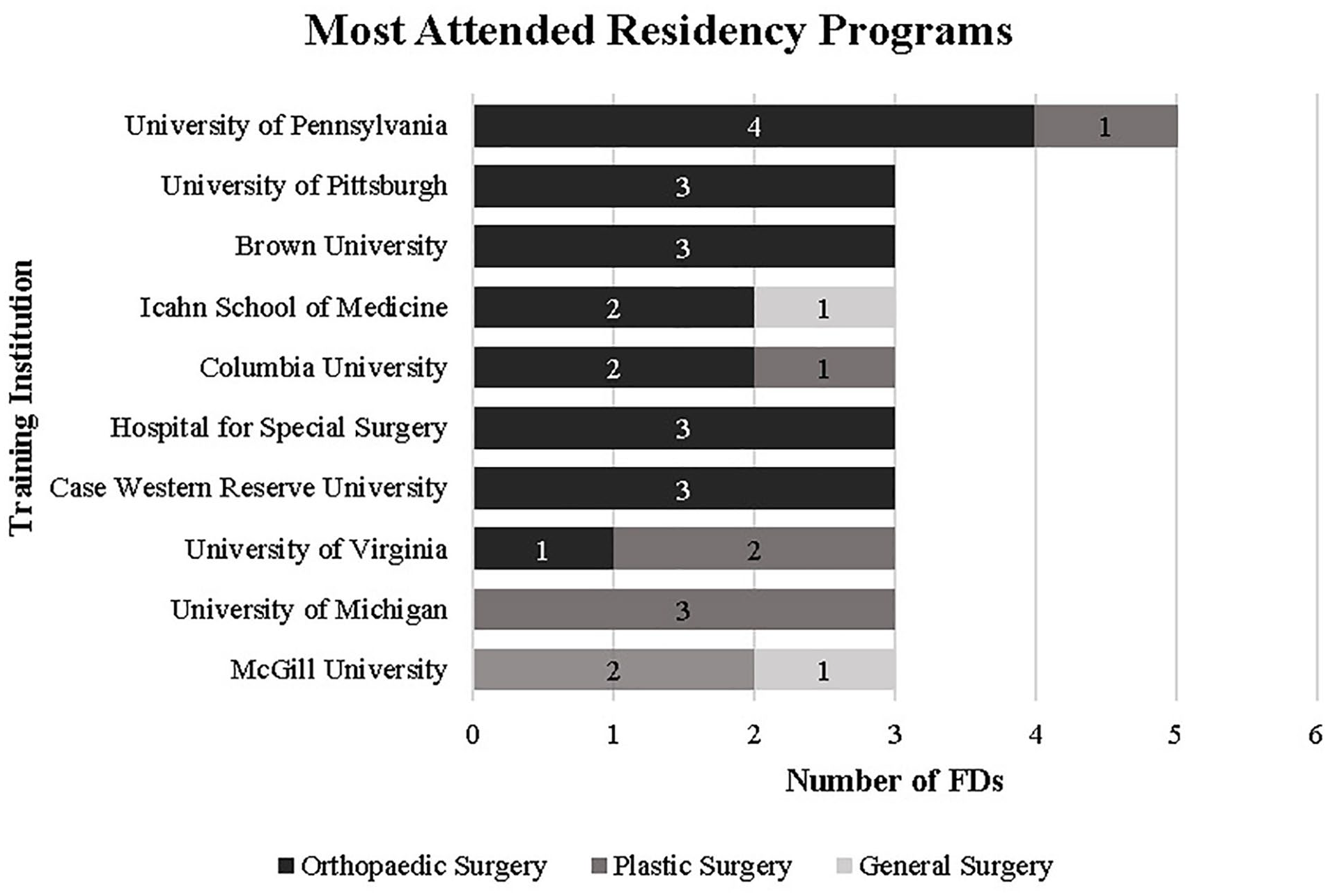
A summary of the most attended residency training programs among current hand FDs. Residency programs at which at least 3 FDs trained were included.
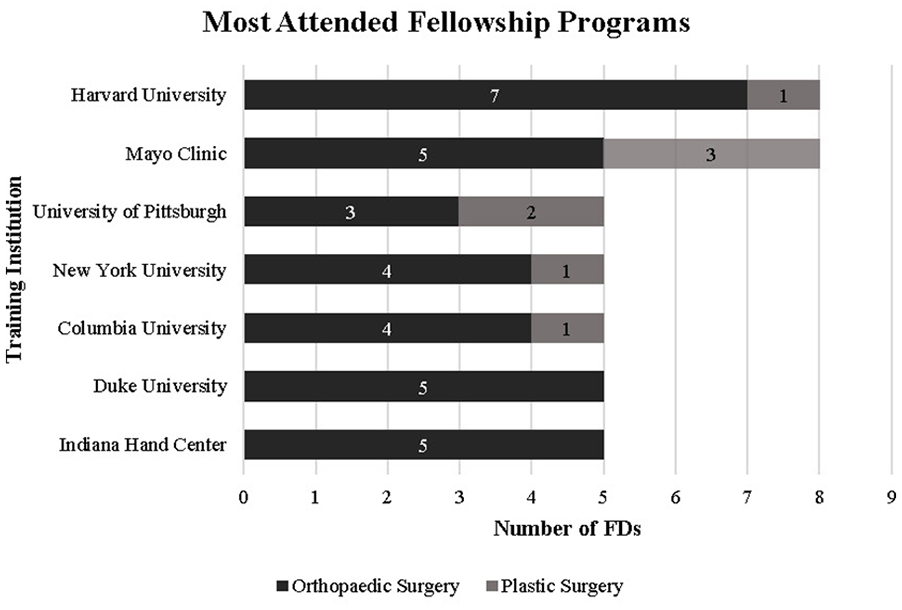
A summary of the most attended fellowship training programs among current hand FDs. Fellowship programs at which at least 5 FDs trained were included.
Figure 3 illustrates the distribution the Scopus H-indices for FDs in the form of ranges. At the time this study was completed, the most proficient FD in research had a Scopus H-index value of 40. By comparison, the 10th most proficient FD in research had a Scopus H-index value of 23.
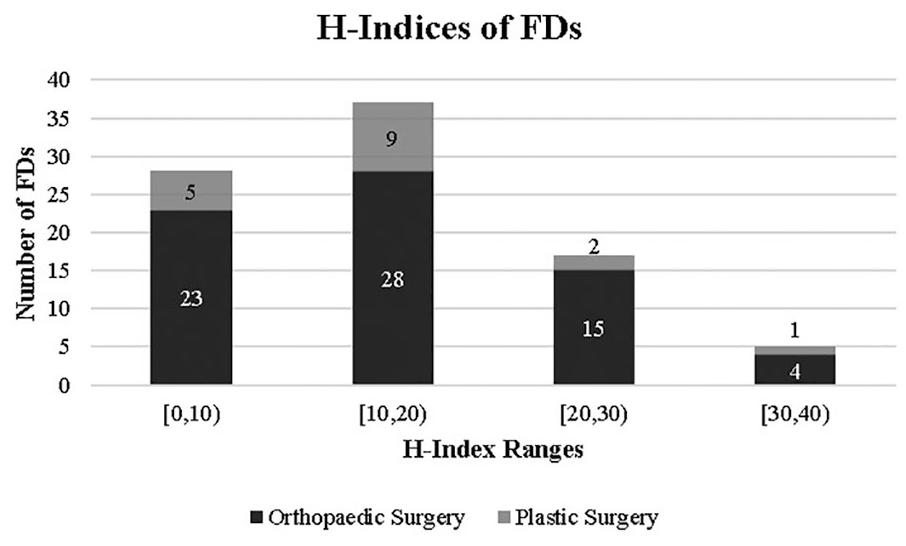
A representation of the Scopus H-indices of all hand FDs.
Discussion
Our investigation critically evaluates the demographic, training backgrounds, academic productivity and detailed educational, employment, and leadership progression of FDs in hand surgery within the United States. The ASSH outlines the various routes to become a hand surgeon through training in orthopedic, plastic, or general surgery, before completing a hand fellowship. 11 Our study shows that hand surgeons with backgrounds in orthopedic surgery, as opposed to plastic (24.4%) or general surgery (2.2%), hold most FD positions (73.3%). Within orthopedic surgery hand fellowship programs, 8.3% of FDs were trained in plastic surgery. Conversely, 11.1% of plastic surgery hand fellowship FDs were trained in orthopedic surgery. This may demonstrate that many hand surgery programs are multidisciplinary and involve both orthopedic and plastic surgeons. Our study found that 8 institutions had separate hand fellowships in both their orthopedic surgery and plastics surgery departments. Hand surgery fellowship programs may have a preference or even restrict applicants to those of the same discipline, either orthopedic or plastic surgery. Understanding what opportunities are available for aspiring hand surgeons may explain this multidisciplinary approach. Applicants should consider the predominance of orthopedic surgeons in the field of hand surgery and opportunities for roles of leadership when choosing a training program.
Recent studies in spine and adult reconstruction orthopedic surgery used similar approaches to observe trends among FDs.8,9 Comparing these specialties with hand surgery can inform paths to leadership positions. Hand FDs took on average 11.3 years from fellowship graduation to FD appointment. This time period was found to be longer for hand FDs than for orthopedic spine (8.6) and adult reconstruction FDs (9.6).8,9 Professional development and, subsequently, promotion in academic medicine involves demonstrated teaching ability, service work, and research productivity. It is possible that the opportunities within hand surgery to complete promotion activities may be limited due to the specialized training and focus of the field. The average Scopus H-index of 13.98 among hand surgery FDs was lower than H-indices for spine and adult reconstruction FDs.8,9 However, within hand surgery, the average H-index was nearly identical when compared between FDs trained in orthopedic and plastic surgery. Previous literature describes the use of H-index as an adjunct for assessment of research productivity and demonstrates a strong correlation between H-index and academic rank in hand surgery. 12 The number of journals for hand surgery and variability of publication opportunities specific to the field may be lower than those available to orthopedic spine and adult reconstruction. Therefore, while it may be interesting to compare H-index between specialties, its use should be considered only as a verifiable metric of research productivity between individuals within the same specialty.
Additional factors to consider when evaluating the progression of hand surgery FDs include the influences of institutional residency and fellowship programs. Prior studies suggest that successful fellowship match is correlated with professional connections at the residency and fellowship levels.13,14 In the field of hand surgery, 50% of all FDs hold positions at the same institution where they either completed their residency training, fellowship training, or both, emphasizing the impact that training programs can have on individuals’ career paths. Once hired by their current institution, hand surgeons tended to remain at that institution for an extended period (17.1 years, ±9.6 years). Also, certain institutions produce large percentages of current hand FDs. The 10 most attended residency programs among current FDs were responsible for producing 32 of the 90 FDs, nearly 36% of the population. The 7 most attended fellowship programs account for 46% of current hand FDs. These trends were similarly observed in other orthopedic specialties,8,9 and these trends may influence the cohort of applicants with academic career aspirations to pursue specific programs. The determination of FD trajectory reveals elements of both institutional loyalty and the positioning of training programs dictate the selection of future leaders.
This study also highlights the demographic backgrounds of current hand surgery FDs. The average age of 55.2 years among hand FDs is older than that of orthopedic spine and adult reconstruction FDs (51.4-52.9, respectively). This slight difference in age may reflect the amount of additional training the average hand surgeon completes, taking into consideration years to complete plastic or general surgery residencies. Approximately one-third of hand surgery FDs (28.9%) completed multiple fellowships adding to this age difference. Our review also shows that leadership at hand surgery fellowships is male dominated (86.7%, n = 78); the number of female hand FDs (13.3%, n = 12) is low. Further analysis shows that the number of female FDs between orthopedic (n = 9, 12.5%) and plastic (n = 3, 16.7%) surgery hand fellowships was similar. A review of the Accreditation Council for Graduate Medical Education Databook for 2019 to 2020 revealed that orthopedic surgery hand fellows (men: 74% and women: 26%) and plastic surgery hand fellows (men: 65.2% and women: 34.8%) have a sex distribution that more closely resembles that of the US population (men: 49.2% and women: 50.8%). 15
However, despite these low numbers, the percentage of women in FD positions was found to be higher in hand surgery (13%) than in orthopedic spine (4%) and adult reconstruction (0%).8,9 Many orthopedic surgery residency programs report some of the lowest proportions of women when compared with other fields of medicine.16,17 Collectively, these reports demonstrate shortcomings in sex equality. Another study reports that male hand surgeons had a higher mean H-index than female surgeons. 12 However, after adjustment for effects of other research degrees, affiliations, and training backgrounds, those authors concluded that sex was not significantly associated with academic rank (P = .91). 12 Although academic hand surgery has experienced a rise in female fellows, an inverse relationship has been observed in academic progression as fewer women hold positions in leadership. 18 Future work is required to continue to foster a place for women in leadership positions in hand surgery. 17
The collective of current hand FDs also demonstrates the need for improved racial and ethnic diversity; 71.4% percent of FDs identified as Caucasian, 21.4% as Asian-Americans, 3.6% as Hispanic/Latinos, and 3.6% as Middle Eastern. Many studies have identified the underrepresentation of minorities within the field of orthopedics and have observed regressions in minority representation in residencies.19-23 One study states that increased diversity in orthopedic surgery will improve patient care through better communication, cultural competency, and improved access. 23 At the time of this study, no hand surgery FD identified as African American in response to the inquiry regarding race/ethnicity. Efforts are being made to address the need for a more increase diverse field through pipeline programs, conscientious mentoring, and targeted participation in medical schools. 23 Hand surgery may benefit from implementing similar strategies.
Diversity among leaders may enhance the training experience for the next generation of FDs and enable progress and innovation in the field through different perspectives and shared strategic planning. The paucity of women and minorities holding leadership positions in hand surgery education demonstrates the need to continue to pursue diversification of our field. These deficits may also inspire future surgeons to contribute to make changes in the field. Our community of hand surgeons should continue to pursue efforts to foster diversity in leadership positions, and by doing so, will continue to build professional development frameworks for the future leaders of hand surgery.
We must acknowledge some critical limitations of our investigation. First, our data collection relies on the use of self-reported CVs. When possible, missing data were obtained using online databases, e-mails, or phone calls. Additional responses from hand surgeons could have provided value to our metrics. For example, only 62% of respondents self-selected race or ethnicity categories (n = 56). Second, the study design analyzes data at a single point in time. Our study used the ASSH hand fellowship directory to incorporate the hand fellowship programs included in this study and relied on the specialty designation provided through that database to classify programs as orthopedic or plastic surgery programs. We understand that many factors influence how institutions operate and the division between orthopedic and plastic surgery can be complex. Further research could report on variations over time through sequential comparisons and conduct program evaluations around concentrated efforts to adapt the field of hand surgery. While this study focused on the FD role, additional review of other leadership positions within the field of hand surgery may provide a more comprehensive analysis of the specialty. Finally, our results focused on obtaining objective data for analysis. No assessment or evaluation of subjective factors that can impact an individual’s appointment and/or pursuit of academic leadership positions was included in this study.
Conclusion
The trends observed in this study provide objective data to describe current hand surgery FDs. Our results showed that hand surgery FDs are frequently distinguished by their level of academic productivity and training background. In addition, it appears that specific training programs prepare more individuals for future FD positions. Our results also showed racial/ethnic and sex disparities exist among hand surgery FDs. By continuing to focus on diversifying these distinguished leadership positions, future FDs will enhance the training experiences for the next generation of hand surgeons and promote innovation in the field by bringing different perspectives to strategic planning. Moreover, these efforts toward promoting diversity and providing minorities with opportunities to take on leadership roles will lead to a better representation of the communities these hand surgeons serve. Ultimately, this discussion may serve as a guide for our community of hand surgeons to evaluate the field’s advancement of leadership positions and for individuals who desire these academic leadership roles.
Footnotes
Authors’ Note
The authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Author Contributions
All authors significantly contributed to the document and have reviewed the final article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
No human and/or animal subjects were used in this study.
Statement of Informed Consent
This study did not require the use of informed consent. There are no relevant disclosures, copyrighted materials, or signed patient consent forms associated with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.