
Abstract
Background:
Carpal tunnel release (CTR) is one of the most commonly performed procedures in hand surgery. Complications from surgery are a rare but significant patient dissatisfier. The purpose of this study was to determine whether insurance status is independently associated with complications after CTR.
Methods:
We retrospectively identified all patients undergoing CTR between 2008 and 2018 using the Indiana Network for Patient Care, a state-wide health information exchange, and built a database that included patient demographics and comorbidities. Patients were followed for 90 days to determine whether a postoperative complication occurred. To minimize dropout, only patients with 1 year of encounters after surgery were included.
Results:
Of the 26 151 patients who met inclusion criteria, 2662 (10.2%) had Medicare, 7027 (26.9%) had Medicaid, and 16 462 (62.9%) had commercial insurance. Compared with Medicare, Medicaid status (P < .001) and commercial insurance status (P < .001) were independently associated with postoperative CTR complications. The overall complication rate was 2.23%, with infection, wound breakdown, and complex regional pain syndrome being the most common complications. Younger age, alcohol use, diabetes mellitus, hypertension, and depression were also independently associated with complications.
Conclusions:
The incidence of complications after CTR is low. Insurance status, patient demographics, and medical comorbidities, however, should be evaluated preoperatively to appropriately risk stratify patients. Furthermore, surgeons can use these data to initiate preventive measures such as working to manage current comorbidities and lifestyle choices, and to optimize insurance coverage.
Keywords
Introduction
Carpal tunnel syndrome (CTS) affects 2.7% to 5.8% of the overall adult population1,2 and as much as 7.8% of working adults in the United States.3,4 The incidence of CTS in the United States has risen over time from 258 cases per 100 000 person-years between 1981 and 1985 to 424 cases per 100 000 person-years between 2001 and 2005. 5 Correspondingly, there was a 33% increase in the number of carpal tunnel release (CTR) procedures performed from 1996 to 2006. 6 As a result, CTS has been called the most expensive upper extremity musculoskeletal disorder, costing approximately $2 billion in direct costs per year.3,7
Carpal tunnel release is a low-risk outpatient procedure that can be performed by either open or endoscopic techniques with comparable improvement of symptoms, return to functional status, time to return to work, and overall complication rates.8-10 Intraoperative complication rates for CTR are rare, whereas postoperative complications, such as complex regional pain syndrome (CRPS), infection, and wound dehiscence, may occur. 11 Despite the low complication rate, affected patients may suffer from loss of work time and/or employment and a decreased quality of life. 12 As such, an evaluation of factors associated with CTR complications is warranted to optimize patient outcomes.
Health insurance status is one socioeconomic variable included in studies assessing surgical outcomes, including after hand and upper extremity surgery. For example, in a study by Devana et al 13 evaluating complications after endoscopic or open CTR, they reported differential rates of median nerve injury in patients with different insurance types. Given the potential impact on outcomes and as a tool for surgical risk stratification, we sought to better understand the relationship between insurance type and postoperative complications following CTR. We hypothesize that insurance status impacts the incidence of CTR postoperative complications.
Materials and Methods
Data Collection
We used the Indiana Network for Patient Care (INPC) to build a comprehensive database with unique and deidentified patients, 18 years of age and older, who underwent surgical treatment for CTS via open or endoscopic CTR between 2008 and 2018. The INPC is a health information exchange that links health care data from disparate sources in real time through a global patient index. Sources cover the continuum of inpatient and outpatient health care for more than 14 million patients; therefore, it includes the vast majority of patients, encounters, and health care data in the state of Indiana and surrounding catchment areas. Data inputs are both codified and free text data from sources such as electronic medical records, insurance claims, operative records, public health databases, pharmacies, picture archiving and communication system, and a variety of other sources.14-17 Therefore, data are directly input by providers at the point of care and validated through insurance claims and other mechanisms. For research purposes, the Regenstrief Institute provides access to the proprietary system and quality assurance of the data through a team of data analysts.
We used the INPC to identify all patients who underwent isolated CTR as defined by Current Procedural Terminology (CPT) codes and the International Classification of Diseases (ICD) 9th or 10th Edition codes: CPT 29848 or 64721, ICD-9 04.43, and ICD-10 01N50ZZ, 01N53ZZ, or 01N54ZZ. Among those who underwent CTR, only those with follow-up in an INPC participating institution within 1 year of the procedure and documented insurance status at the time of the procedure were included, which helped to minimize patient dropout. For patients who had more than 1 CTR, we studied only the first procedure. Patients with a diagnosis of 1 or more of the following complications, based on ICD-9 or ICD-10, within 90 days of surgery were identified: hand infection, neurovascular injury, retained foreign body, wound breakdown, and CRPS (Supplemental Table 1). The recurrence of CTS was not included. Comorbidities previously reported as risk factors for postoperative CTR complications were also identified and recorded. Only comorbidities active within the year before surgery were included in the study. Patients were divided into 3 discrete cohorts: Medicare insurance, Medicaid insurance, and commercial insurance. Patient data were stored using Indiana University cloud computing and analyzed using Stata/MP 16.1 (StataCorp LLC, College Station, Texas) in compliance with the Health Insurance Portability and Accountability Act of 1996.
Statistical Analysis
We performed univariate analysis to analyze the population sample, followed by χ2 and Fisher exact tests to examine the bivariate relationships between variables. We then used backward stepwise multivariable logistic regression analysis to examine the relationship between patient variables and CTR complications. In the stepwise backward-selection estimation method, we used a P value of .25 as the threshold for removal from the final model. Factors included in the stepwise regression model comprised age, sex, alcohol use, diabetes mellitus (DM), hyperlipidemia, hypertension, arthritis, peripheral vascular disease, congestive heart failure, coronary artery disease, chronic kidney disease, depression, and coronary artery disease. Body mass index (BMI) data were reported in only 37.1% of patients, so was excluded from the multivariable analysis. Robust variance method was used to report standard errors and P values to account for uncertainty in estimates due to model misspecification, if any.18-21 Adjusted odds ratios and 95% confidence intervals were calculated for each factor, with P < .05 considered statistically significant. Multicollinearity in the linear regression model was quantified via variance inflation factor (VIF), which indicates the strength of the collinearity and whether the degree of variances for each predictor in the multivariable model is inflated due to this collinearity. In general, a VIF >10 is considered to have a detrimental effect on the relationship between the predictors and the outcome.22,23
Results
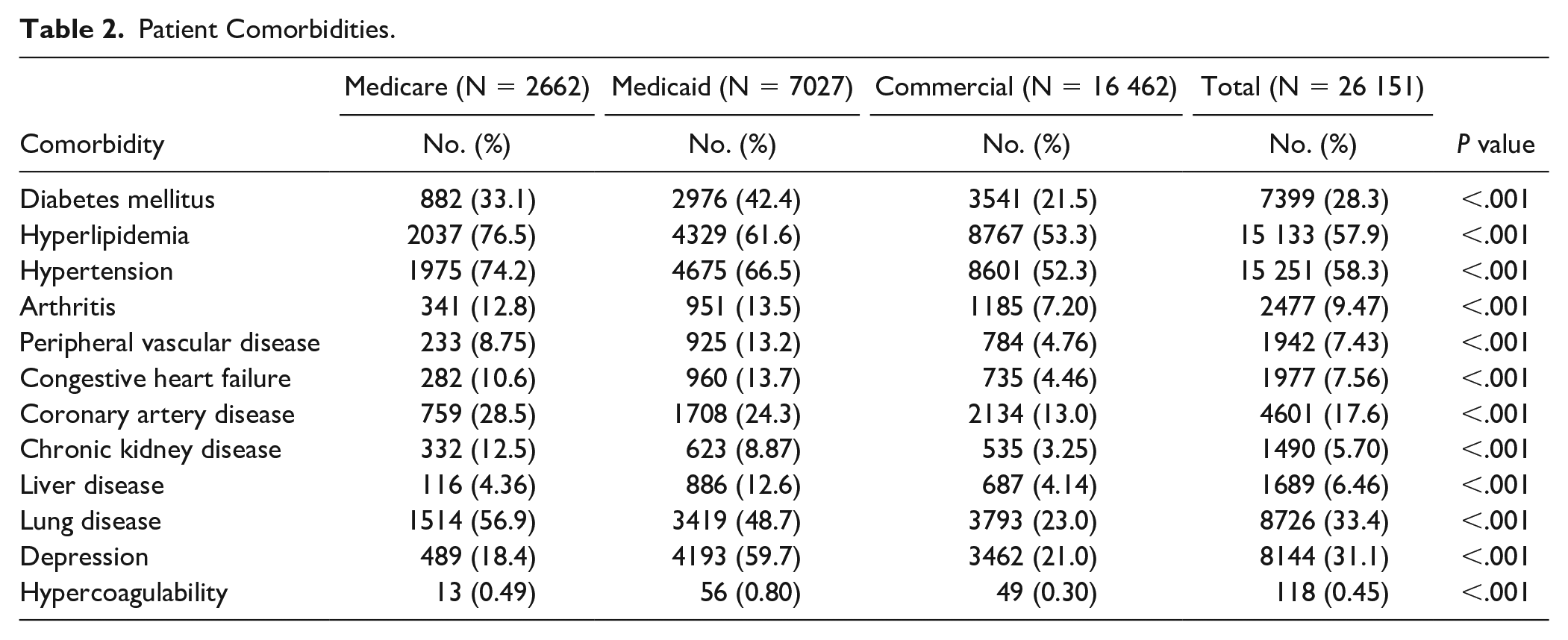
Overall, 26 151 patients met inclusion criteria: 2662 (10.2%) had Medicare, 7027 (26.9%) had Medicaid, and 16 462 (62.9%) had commercial insurance. Patient demographics varied across insurance cohorts. The average BMI was 32.4 ± 7.7 kg/m2, and the Medicare cohort was the oldest (74.7 ± 7.0 years). The Medicaid cohort had the highest proportion of women (76.4%) and alcohol use (11.6%) (Table 1). The Medicaid cohort had the highest proportion of several comorbidities (Table 2). There was a statistically significant difference in comorbidities between insurance groups (P < .001) (Table 2).
Patient Demographics.
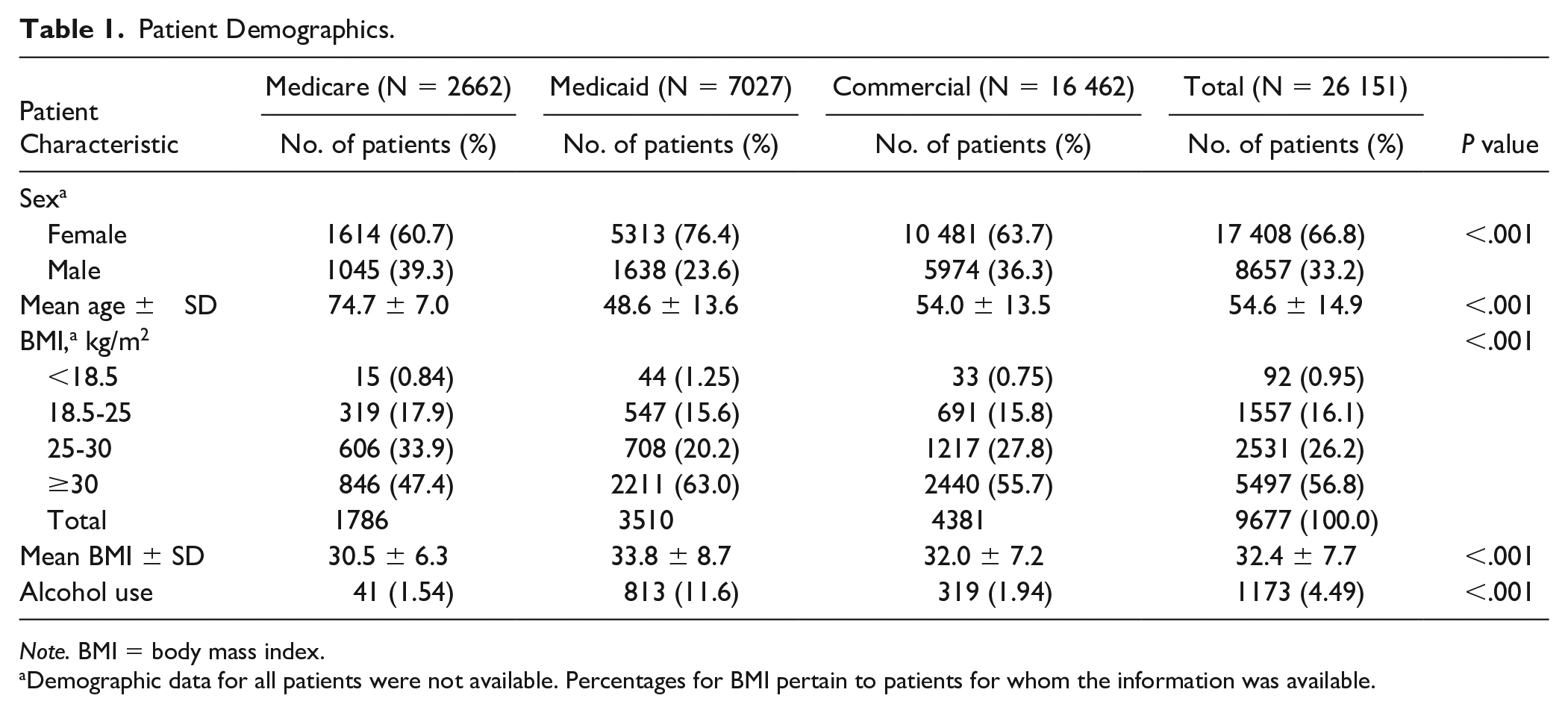
Note. BMI = body mass index.
Demographic data for all patients were not available. Percentages for BMI pertain to patients for whom the information was available.
Patient Comorbidities.
Postoperatively, 11 (0.4%) Medicare patients, 303 (4.3%) Medicaid patients, and 268 (1.6%) commercial insurance patients had at least 1 complication (P < .001). The most common complications were infection (1.65%), wound breakdown (0.43%), and CRPS (0.21%). Cohort differences for each complication were statistically significant (P ≤ .001) (Table 3). There were 248 (3.35%) patients with DM and 334 (1.78%) non-DM patients who developed a complication (P < .001). For patients with DM, infection (2.53%) and wound breakdown (0.68%) were the most common complications (Table 4).
Complications After Carpal Tunnel Release.
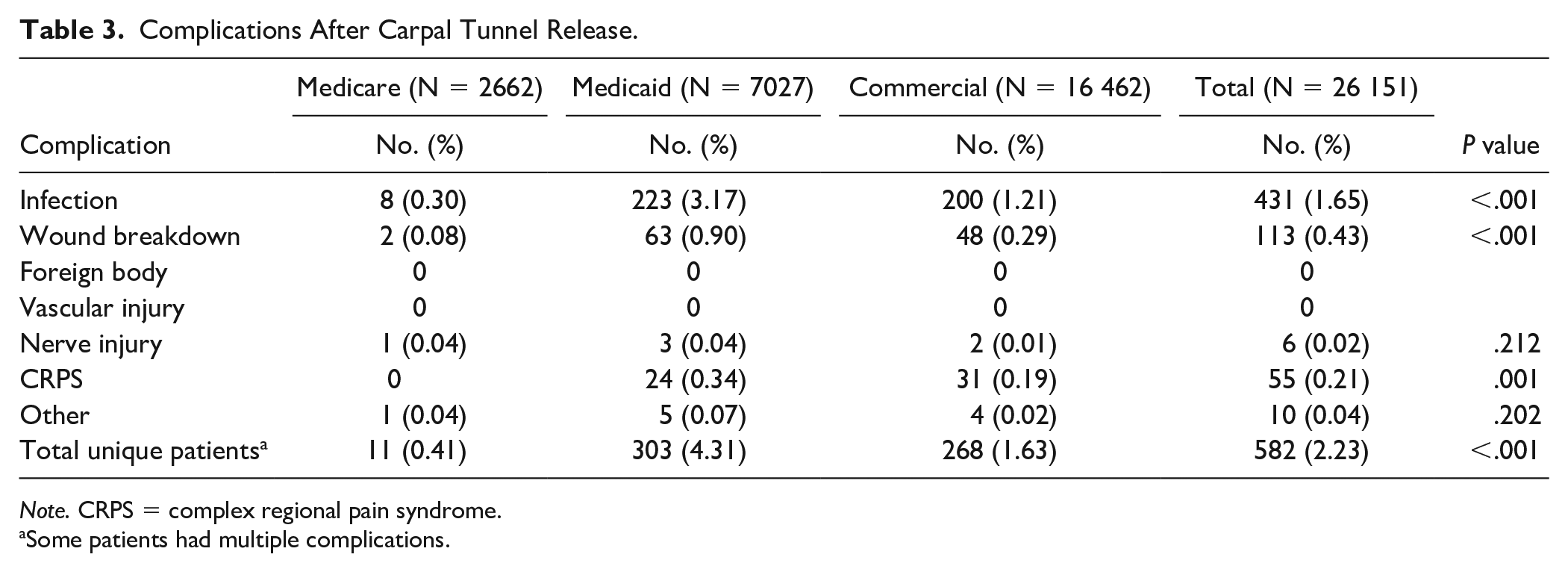
Note. CRPS = complex regional pain syndrome.
Some patients had multiple complications.
Complications After Carpal Tunnel Release in Patients With Diabetes Mellitus.
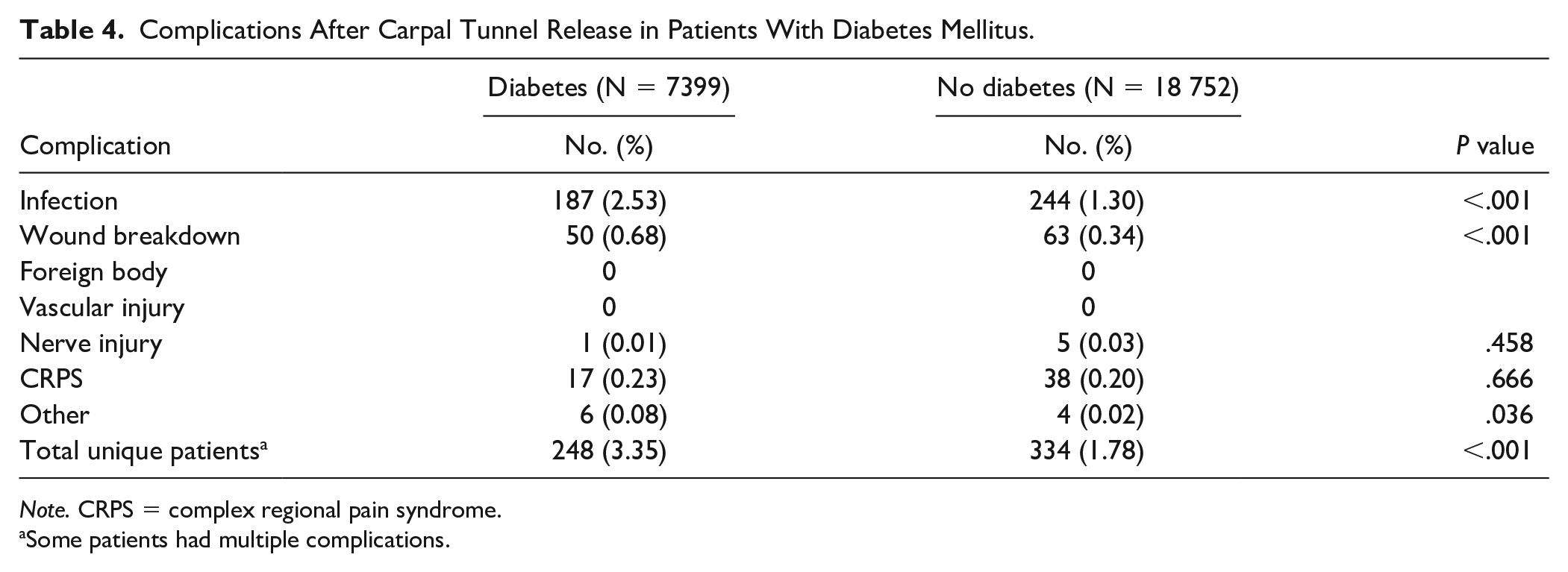
Note. CRPS = complex regional pain syndrome.
Some patients had multiple complications.
In multivariable analysis, those with Medicaid (P < .001) and commercial insurance (P < .001) were more likely than Medicare patients to sustain a postoperative CTR complication. There was no significant association between sex and postoperative complications. Younger age (P < .001) and alcohol use (P = .008) were associated with increased odds for complications. Diabetes mellitus (P < .001), hypertension (P = .018), and depression (P < .001) were the only comorbidities independently associated with an increased odds for postoperative complications (Table 5).
Multivariable Logistic Regression for Any Complication After Carpal Tunnel Release.
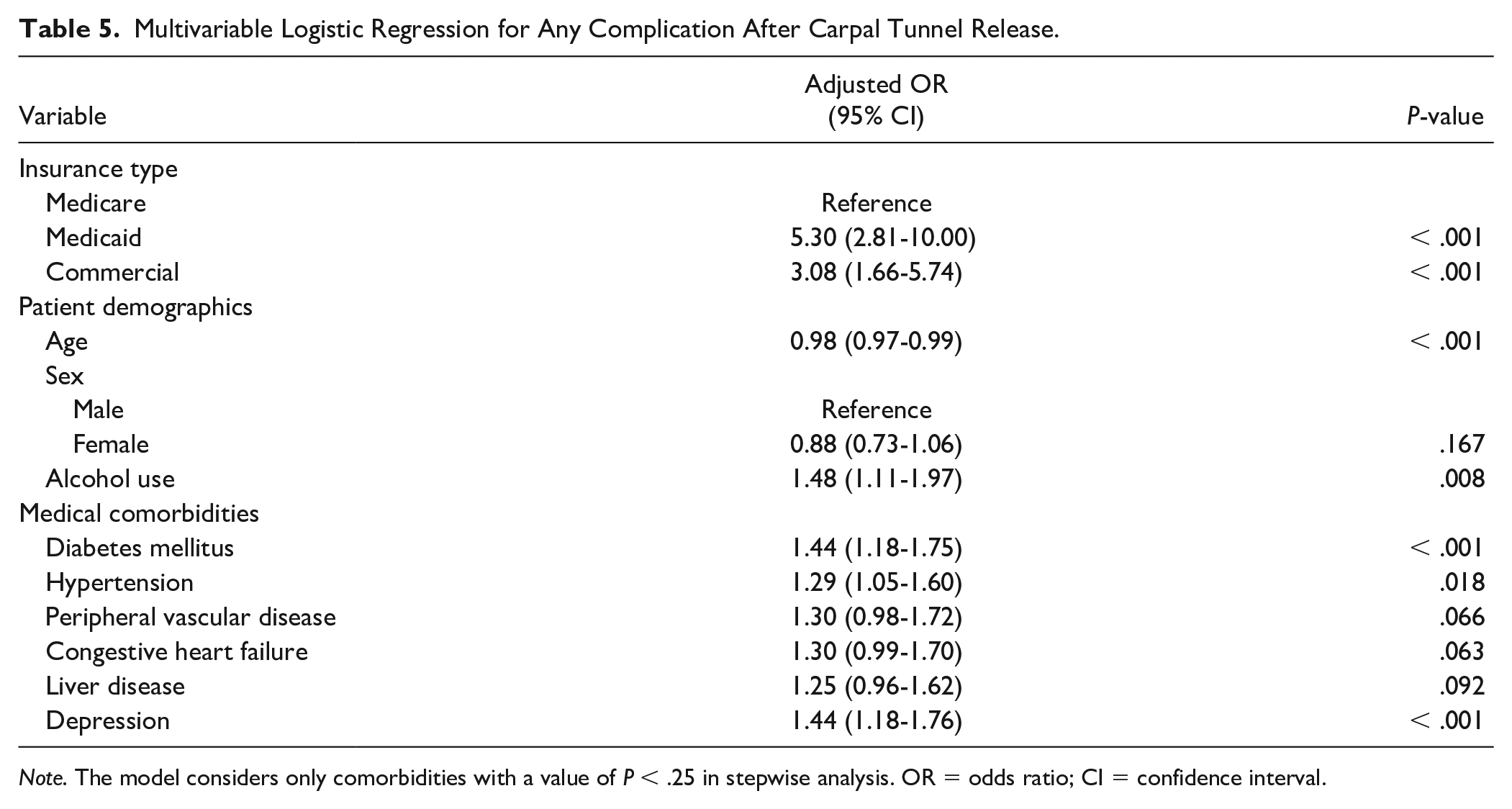
Note. The model considers only comorbidities with a value of P < .25 in stepwise analysis. OR = odds ratio; CI = confidence interval.
Discussion
In this study, we found that insurance status independently conferred an increased odds for complications after CTR. Our findings are consistent with other studies showing that Medicaid patients have higher rates of postoperative complications.24-26 In those studies, the phenomenon was partly attributed to potential biases related to insurance status. 25 Compared with commercial insurance, Medicaid typically reimburses less, and a smaller cohort of physicians accept it for coverage. 27 As such, insurance status alone can have implications for surgeon access (eg, a smaller pool of qualified providers) and can lead to delays before treatment.
It is also possible that insurance status may be, in some cases, a relative proxy for patient-related lifestyle choices. In our study, the Medicaid cohort had the highest proportion of patients with most of the assessed comorbidities and had a higher average BMI and rate of alcohol consumption. The higher rate of comorbidities may be related to decreased health literacy, language barriers, and nutritional deficiencies that can predispose to poorer health outcomes. Insurance status may also be indirectly related to postoperative adherence to recommendations. Patients with less generous insurance coverage may be unable to afford a prescribed antibiotic or undergo a full course of occupational therapy. These physician- and patient-related considerations may partially explain the increased incidence of infection and wound breakdown in the Medicaid cohort and how insurance status may be independently associated with an increased odds for complications after CTR.
The overall rate of complications in this study was relatively low (2.23%) and was similar to previous estimates of 2.5% after CTR. 28 Although 1.65% of all patients in our study developed an infection, only 0.30% of Medicare patients developed a post-CTR surgical site infection. This rate was similar to a study in 454 987 Medicare patients that showed a postoperative infection rate of 0.32%. 29 The incidence of infection was nearly double in patients with DM. This finding may support the use of perioperative antibiotic prophylaxis in this cohort. Previous studies have reported post-CTR CRPS rates of between 2% and 8%,12,30-32 which is significantly higher than our finding of 0.21%; it is important to note that, however, some of the randomized controlled studies used comparatively smaller sample sizes of often less than 200 patients. Wound breakdown/dehiscence rates in our study (0.43%) were similar to previous estimates in the literature of 0.2%. 28 Finally, neurovascular injury rates in our study (0.02%) were similar to those reported in the literature (0.10%-0.30%). 12
There are multiple relevant limitations to this study. Race data were not recorded for many patients. It has been documented in vascular surgery that nonwhite Hispanic and black patients are more likely to have adverse outcomes and more likely to be enrolled in Medicaid than white non-Hispanics. 24 All data were derived from an administrative database, so there are additional concerns for nonreporting bias and inaccurate data abstraction, which can confound results. Also, all data in this study came from a single state, which may limit generalization across the United States. We attempted to address selection bias by only using patients with documented postoperative follow-up. There was no concern for collinearity in this study as the VIF never exceeded 10 in any of the variables studied. Despite these limitations, our findings remain clinically relevant, and surgeons can use these data for considerations in CTR to optimize health care outcomes.
Conclusions
Complications after CTR are rare, yet insurance status, patient age, alcohol use, DM, hypertension, and depression are independently associated with postoperative complications. Surgeons can use these findings to appropriately stratify patients preoperatively and to initiate preventive measures such as working to manage current comorbidities and lifestyle choices, and to optimize insurance coverage.
Supplemental Material
sj-pdf-1-han-10.1177_1558944721990818 – Supplemental material for The Association of Insurance Status and Complications After Carpal Tunnel Release
Supplemental material, sj-pdf-1-han-10.1177_1558944721990818 for The Association of Insurance Status and Complications After Carpal Tunnel Release by Phoebus Sun Cao, Scott N. Loewenstein, Lava R. Timsina and Joshua M. Adkinson in HAND
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Benjamin Lancaster for his assistance in preparing this manuscript.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.