
Abstract
Background:
Prior studies suggest steroid injections may affect infection rates following thumb carpometacarpal joint (CMCJ) arthroplasty. However, it is unclear whether injections prior to CMCJ arthroplasty affect functional outcomes, primarily Quick Disabilities of the Arm, Shoulder, and Hand (qDASH).
Methods:
We retrospectively identified patients who underwent thumb CMCJ arthroplasty from 2015 to 2019. Patients who had qDASH scores reported preoperatively, and at 5 and 11 months postoperatively were included. Charts were reviewed for the presence or absence of prior corticosteroid injection to the CMCJ and complications. Delta qDASH was calculated by subtracting the patients’ postoperative qDASH scores from the preoperative qDASH scores.
Results:
In all, 350 CMCJ arthroplasty patients were identified, 177 who had received at least 1 steroid injection and 173 who were steroid-naïve. No significant differences existed in delta qDASH scores postoperatively between the injection and naïve groups at 5 months (28.5 vs 28.6) or 11 months (31.2 vs 31.9). Whereas there were no significant differences in rates of major complications between the 2 groups, minor complications were higher in the injection group (16.4% vs 9.2%). Patients who received more than 3 injections did not have worse 5-month or 11-month delta qDASH scores or complication rates than those with fewer than 3.
Conclusions:
Preoperative CMCJ steroid injection status does not affect major complication rates or functional outcomes following CMCJ arthroplasty. However, injections increase the rate of minor complications. The qDASH and complication rates following CMCJ arthroplasty are not affected by receiving greater than 3 injections preoperatively.
Keywords
Introduction
Osteoarthritis (OA) of the thumb carpometacarpal (CMC) joint (CMCJ) space is exceedingly common, especially in certain demographics. 1 The prevalence of symptomatic first CMCJ OA among men and women above the age of 70 is estimated to be 13% and 26%, respectively.2,3 The natural history of this disease involves progressive joint space destruction that for many patients leads to disabling pain, stiffness, and an inability to perform essential functions, such as pinch and grasp. 4 Due to its prevalence and the functional limitations it can impose, it is crucial to have a clear understanding of the value of nonoperative and operative options. It is equally imperative to comprehend how preoperative interventions may affect a future operative intervention.
To date, there is no consensus nonoperative algorithm to manage symptomatic thumb CMC OA. Initial treatment options include hand therapy, nonsteroid anti-inflammatory medication, steroid and/or hyaluronate intra-articular injections, as well as orthoses.5-7 Of these modalities, intra-articular steroid injection has emerged as one of the mainstays of conservative management. Prior studies have demonstrated largely heterogeneous results surrounding the efficacy and duration of steroid injections for the treatment of thumb CMC OA. Patients typically experience 1 to 6 months of pain relief following a cortisone injection.8-10 There is growing concern, however, that they may affect future surgical intervention, with data suggesting that prior steroid injections may increase the rate of complications following surgical intervention.11-13 Giladi et al 13 found that patients who had a steroid injection into the thumb CMC joint prior to surgery had a 20% increased risk of postoperative complications when compared with steroid-naïve patients.
As steroid injections are commonly used prior to CMC arthroplasty, their effect on post-surgical outcomes warrants assessment. To our knowledge, there is no existing literature evaluating the effects of prior steroid injections on functional outcomes following CMC arthroplasty. The primary aim of this study was to determine if the use of corticosteroid injections to the thumb CMC prior to surgery affects functional outcomes by measurement of Quick Disabilities of the Arm, Shoulder, and Hand (qDASH) scores postoperatively. A second objective was to perform a more granular examination of the effect of preoperative thumb CMC steroid injection on the rate of postoperative complications. We hypothesize that patients who receive any number of corticosteroid injection prior to thumb CMCJ arthroplasty will have similar qDASH scores and complication rates when compared with steroid-naïve patients who undergo thumb CMC arthroplasty.
Methods
Institutional review board approval was obtained prior to the start of this investigation. Using our center’s surgical registry, we retrospectively identified the medical records from 2015 to 2019 of patients aged 18 years and older who underwent an arthroplasty of the thumb CMC joint by searching all cases coded with Current Procedural Terminology code 25447 at our university. We reviewed patient demographics, type of arthroplasty performed, the presence or absence of prior corticosteroid injection to the CMCJ, minor and major complications, and qDASH scores at the preoperative, and 5- and 11-month postoperative visits. Major complications included infections requiring intravenous antibiotics, complications requiring repeat hospitalization or surgery, or a diagnosis of complex regional pain syndrome. Minor complications included infections requiring oral antibiotics or postoperative symptoms lasting longer than 6 months, which were considered to be persistent symptoms for the purposes of this study.
The procedures were performed by a group of 18 fellowship trained orthopedic hand surgeons at a single university. The indication for thumb CMC arthroplasty was symptoms refractory to conservative treatment measures and was also based on the shared decision making between each patient and their individual surgeon. The type, quantity, and frequency of injections prior to surgery; type of CMC arthroplasty performed; and postoperative care were all administered at the discretion of the treating surgeon. Patients were excluded from our study if prior injection status could not be determined or if preoperative, 5-month, or 11-month qDASH scores were not recorded. Complications were excluded if the treating surgeon indicated in the chart that they were unlikely to be a result of the surgical intervention.
An a priori power analysis determined that at least 226 patients (113 in each group) would be needed to detect a 10.8 difference in qDASH between the 2 groups, assuming a power of 0.8 and an α of 0.05. Changes in qDASH scores (delta qDASH) were calculated by subtracting patients’ postoperative qDASH scores from their preoperative qDASH score. A positive delta qDASH score represented an interval improvement in function, whereas a negative delta qDASH score represented an interval worsening of function. For comparative analysis, the patient cohort was stratified into a group that received any number of steroid injections prior to surgical intervention (injection group) and a group that received no steroid injections prior to surgical intervention (no-injection group). To identify whether greater than 3 injections affected outcomes or complication rates, a subgroup analysis was performed in which the injection group was stratified into a group that received more than 3 injections (heavily injected subgroup) and a group that received 1 to 3 injections (sparsely injected subgroup). Continuous variables were represented as mean ± SD for parametric data and as median and range for nonparametric data, and all categorical variables were represented as count and percent of group. Statistical analysis was performed using t tests for continuous variables and χ2 tests for categorical variables. To determine whether time from the last steroid injection to surgical intervention affected outcomes, logistic and linear regressions were performed with the dependent variables of complications and qDASH scores, respectively, and days from injection to surgery as the independent variable for both tests. A P value < .05 was considered to be statistically significant for all analyses performed.
Results
A total of 1646 thumbs underwent CMC arthroplasty during the study period. We excluded 1232 thumbs due to missing qDASH documentation and 64 thumbs due to insufficient preoperative corticosteroid injection data. This left a total of 350 patients for final analysis, including 177 in the injection group and 173 in the no-injection group. There were no significant differences in baseline demographics between the 2 groups (Table 1).
Baseline Patient Demographics.
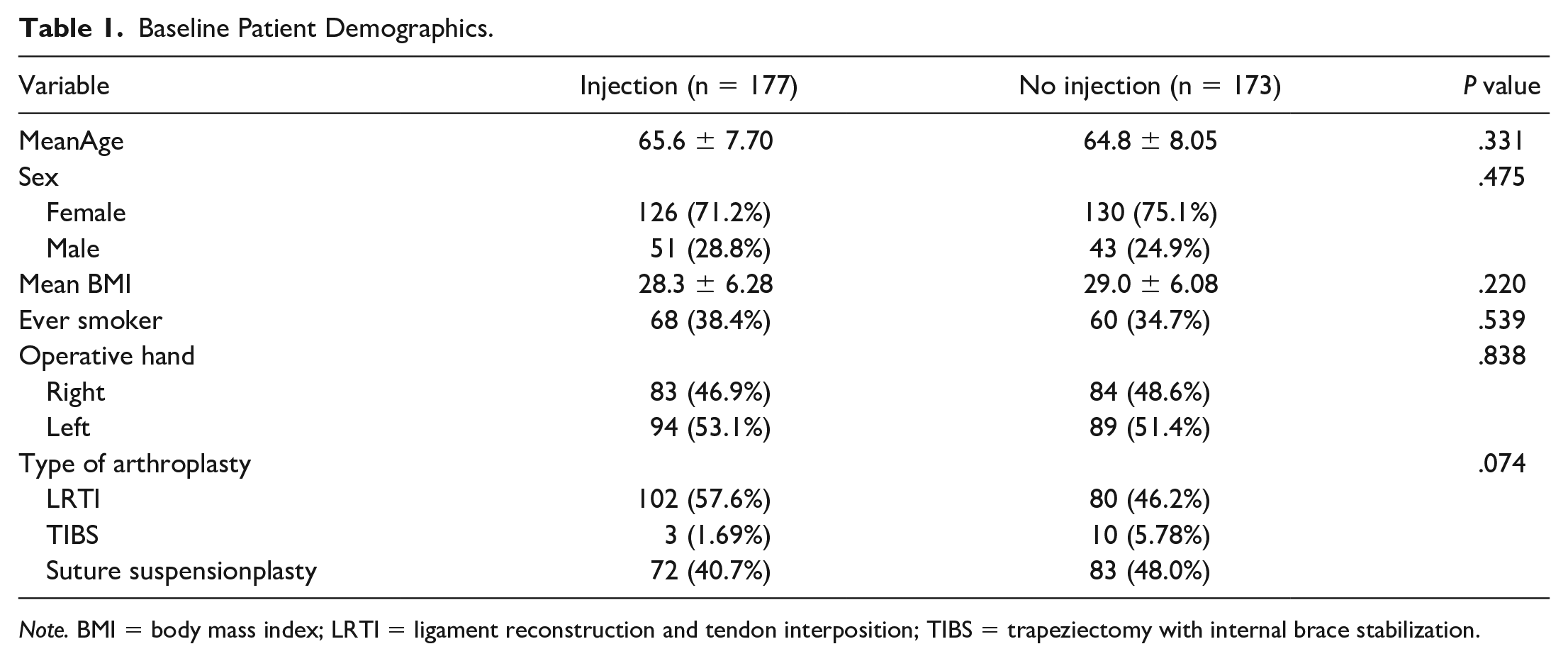
Note. BMI = body mass index; LRTI = ligament reconstruction and tendon interposition; TIBS = trapeziectomy with internal brace stabilization.
On average, patients in the injection group received between 2 and 3 (2.7 ± 1.6) injections prior to surgical intervention. The median time from corticosteroid injection to surgical intervention was 146.0 days (range, 24-892 days). There were no significant differences between the 2 groups for delta qDASH scores at either 5 or 11 months (P = .967, .809). The rate of major complications between the injection group (1.7%) and the no-injection group (1.2%) was not significantly different (P = .672). Major complications in the injection group (n = 3) included 2 revision surgeries and 1 case of hematoma requiring evacuation. In the no-injection group, major complications (n = 2) included 2 revision surgeries. The patients who experienced major complications had similar preoperative DASH scores to those without major complications (48.6 vs 50.1); however, on average, they experienced a smaller decrease in qDASH scores at both 5 months (10.0 vs 28.8 qDASH decrease) and 11 months (31.6 vs 45.6 qDASH decrease) postoperatively. The injection group had a significantly higher rate of minor complications (16.4%) compared with the no-injection (9.2%) group (P = .046). Minor complications in the injection group (n = 29) consisted of 19 cases of persistent pain, 3 cases of infections treated with oral antibiotics, 3 cases of persistent swelling/soreness, 2 cases of persistent paresthesias, and 2 cases of triggering. The 3 cases of infections included 2 cases of cellulitis over the surgical area and 1 case which was an overlying abscess. The latest injections for these 3 patients occurred at 44, 61, and 134 days prior to their surgical intervention, respectively. Two of the infections occurred in a patient undergoing ligament reconstruction and tendon interposition (LRTI), and 1 occurred in a patient undergoing suture suspensionplasty. Minor complications in the no-injection group (n = 16) consisted of 9 cases of persistent pain, 3 cases of triggering, 2 cases of paresthesias, and 2 cases of swelling/soreness. Although patients with minor complications had similar preoperative qDASH scores to those without (52.1 vs 49.8), they experience smaller decreases in qDASH scores at both 5 months (22.6 vs 37.4 qDASH decrease) and 11 months (28.5 vs 41.8 qDASH decrease) postoperatively. Table 2 summarizes these results.
Comparison of Outcomes and Complications After Arthroplasty Between the Injection and No-Injection Groups.
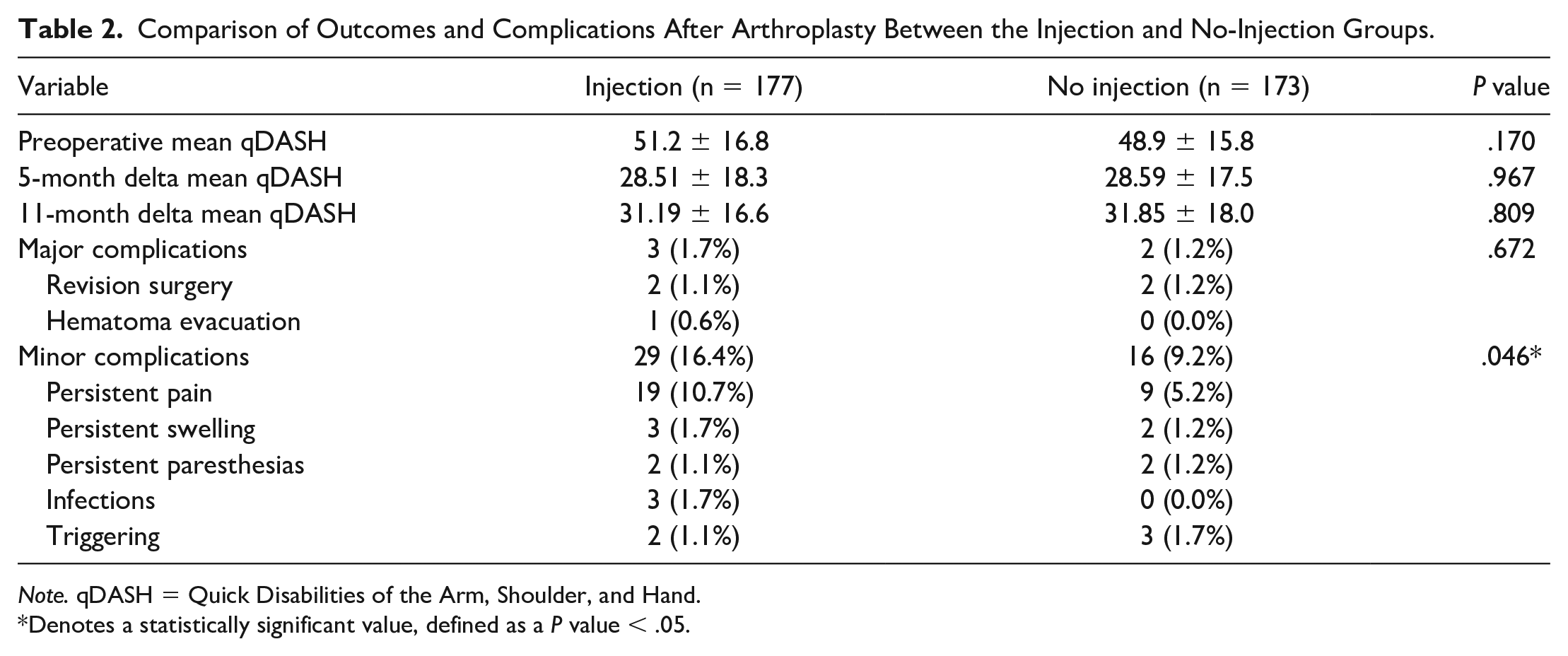
Note. qDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
Denotes a statistically significant value, defined as a P value < .05.
Regarding the injection subgroups, on average, patients in the heavily injected subgroup received between 4 and 5 (4.86 ± 1.20) injections, and those in the sparsely injected subgroup underwent between 1 and 2 (1.87 ± 0.85) injections. There were no significant differences between the 2 groups in qDASH scores or complication rates (Table 3).
Comparison of Outcomes and Complications After Arthroplasty Based on Number of Injections Received.
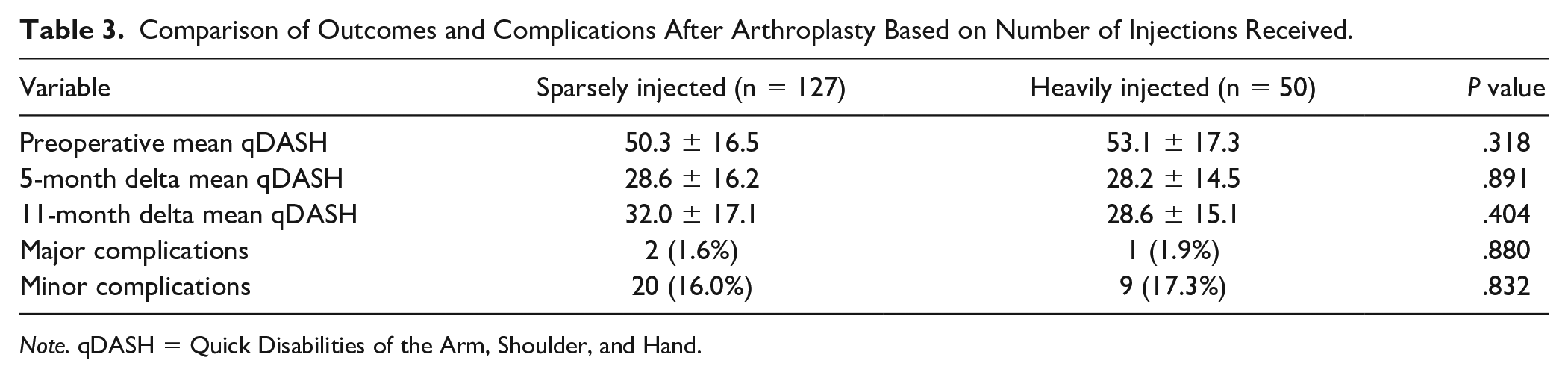
Note. qDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
The median time from corticosteroid injection to surgical intervention was 144.0 days (range, 44-613 days) for patients who developed any postoperative complication. For patients who did not develop a postoperative complication, the median time from corticosteroid injection to surgical intervention was 152.5 days (range, 24-892 days). The whole study cohort was analyzed using logistic and linear regression models to determine if days from injection to surgical intervention affected rates of complications or postoperative qDASH scores. Time from injection to surgery was not a significant predictor of either major or minor complications (P = .921, .190). In addition, it was not found to be a significant predictor of delta qDASH scores at 5 or 11 months (P = .115, .098).
Discussion
Corticosteroid injections are commonly used in the conservative management of CMC arthritis for short-term pain relief and improvement of thumb functionality.7,8,10 Our study supports that neither corticosteroid injections nor number of injections prior to surgery affects postoperative hand functionality. Our observed delta qDASH scores were similar to qDASH scores reported in previous studies.14-16 These findings stand in opposition to the commonly held belief that a maximum of 3 injections should be offered prior to surgery to avoid negative surgical outcomes and complications. These results suggest that patients who are either poor candidates or are hesitant to commit to surgery may be suited to receive greater than 3 steroid injections to alleviate their pain. In addition, prior studies have found corticosteroid injections delay or even completely prevent the need for surgical intervention.8,17,18 Gershkovich et al 19 found that only 13% of patients treated with steroid injections went on to need operative treatment within the 2-year follow-up period. This is important to highlight, as surgical intervention is not without consequence. Although the specific rate depends on the definitions and period chosen, complication rates for CMC arthroplasty can vary from 1.3% to 20%.13,20,21 When taken in conjunction with our study findings, this suggests that surgeons can safely use corticosteroid injections in the treatment of CMC arthritis without affecting operative outcomes if future surgical treatment is warranted.
In our study, we did not find a difference in major complications between the 2 groups. With our definition of a major complication, rates were low in both groups. In contrast, minor complications were higher in the injection group than in the no-injection group, similar to the findings of Giladi et al. 13 However, their study also found a stepwise increase in the rate of complications for every additional preoperative steroid injection which we were unable to replicate. The reasons for this discrepancy may be due to the reliance on a database in their study. The most notable weakness mentioned in their study was the coarseness of the search parameters in identifying complications. By using a broad set of International Classification of Diseases, Ninth Revision (ICD-9) codes ranging from 998.83—“Non-healing surgical wound”—to 682.8—“Cellulitis and abscess of other site”—the results were open to confounding. It is possible that Giladi et al overestimated complication rates by unknowingly including some conditions that were loosely or simply not related to the surgical intervention. In contrast, our study used a detailed chart review and included only conditions the treating surgeon deemed could reasonably be a result of the surgical intervention. Our study also evaluated complications with a minimum follow-up of 11 months, compared with the 2-month follow-up captured by their study. With a longer follow-up period, we saw no additional risk of major complications in the injection group, suggesting that physicians may use steroid injections to avoid more invasive measures until a joint decision is made between the physician and patient to proceed with surgical intervention.
Although we found no differences in major complication rates between the 2 groups, our study found a significantly higher rate of minor complications in the injection group compared with the no-injection group. The higher rate of minor complications may be related to the effect of steroids on inhibiting all phases of the wound-healing process. Corticosteroids are known to be associated with dehiscence of surgical incisions and increase the time of open-wound healing. They antagonize various growth factors and cytokines, thus interfering with inflammation, fibroblast proliferation, collagen synthesis and degradation, deposition of connective tissue ground substances, angiogenesis, wound contraction, and re-epithelialization.22,23 It is possible that the higher reported minor complication rate in the injection group, such as swelling, is due to the effects of steroid on inflammatory response and wound healing. However, it is important to note that these minor complications did not warrant any further treatment. Even patients experiencing these complications reported greater functionality following surgical intervention as indicated by lower postoperative qDASH scores. The benefits of steroid injection in delaying or avoiding surgery likely outweigh the risk of increased rate of minor complications if surgery is indicated at a later point.
Surgeons are often hesitant to perform surgery in patients who received a recent corticosteroid injection. Prior research in joint arthroplasty and trigger finger have supported this belief, finding that injections within 3 months of surgical intervention are associated with higher rates of complications.24-27 In contrast, our study found that there was no association between the timing of injection and complication rates or functional outcomes. Those studies found that infections specifically were the complications associated with recent corticosteroid injections. Our study cohort only had 3 cases of infection, so we were unlikely to have adequate power to determine the relationship between infection and injection timing. When all complications are considered, recent literature does not point to a strong association between recent injection and complication rates.28,29 There is a need for a larger cohort study to better examine the relationship between injection timing and complication rates when performing CMC arthroplasty.
We are aware of a few key limitations with our study. Due to its retrospective design, the treatment algorithm for the patient cohort was not standardized and was left at the treating surgeon’s discretion. This leaves the possibility for unidentified confounders, such as postoperative care protocols, to affect the results of the study. However, we believe these effects are minimal as most baseline demographics were similar between the 2 studied groups. This variance in protocol likely represents that which is seen in general clinical practice. Steroid injection technique and the amount or type of steroid injected were not standardized or studied. Therefore, we could not account for the influence of a possible dose-dependent or technique-dependent effect on the results of our study. Furthermore, patient injection status was based on our institution’s records for the patients. We could not account for the number of injections received at an outside institution. Finally, some patients in the no-injection group may have received a prior injection at a different institution but failed to mention this to their treating surgeon. We attempted to minimize this by excluding all patients for whom injection status was not clearly noted in the charts.
In conclusion, preoperative thumb CMC steroid injection status does not affect functional outcomes following arthroplasty as measured by change in qDASH score at 5 or 11 months. Whereas the risk of minor complications was affected by preoperative thumb CMC steroid injection status, the rate of major complications was not. However, there remains a paucity of research on this topic, and it warrants future investigation with strong prospective studies. While we continue to recommend the use of steroid injections for conservative treatment of thumb CMC arthritis, physicians should evaluate the risks and benefits for each individual patient.
Footnotes
Authors’ Note
This work was performed at Rothman Orthopaedic Institute, Philadelphia, Pennsylvania, USA.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
All patient information has been de-identified, and informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.