
Abstract
We report a case of an 11-year-old girl with bilateral severe Madelung deformity who underwent radial osteotomy with callus distraction. The distal radial articulation was corrected at surgery, and a unilateral fixator was subsequently used for callus distraction. No postoperative complication was noted. The patient did not need any additional surgeries for correction of the deformity. Forty-three months after surgery, the patient had a nearly full range of motion without any pain. Forearm deformity was not noticeable, except for surgical scar on both wrists.
Keywords
Introduction
Madelung deformity is characterized by an abnormal growth at the distal radial physis. It causes abnormal declination of the volar and ulnar sides of the distal radius and dorsal dislocation of the ulnar head. The symptoms of Madelung deformity usually begin in late adolescence, and the degree of deformity and associated symptoms vary across patients. Consequently, various surgical interventions, such as corrective osteotomy, Vickers ligament release, and ulnar shortening, have been attempted.1-9 However, all these procedures can only reduce the severity of the deformity and pain without preventing the development of physeal disorders. Herein, we report a case of an adolescent patient with severe forearm deformity in whom we performed callus distraction with corrective osteotomy.
Case Report
Clinical Presentations and Findings
An 11-year-old girl was referred to our clinic due to restricted motion of both wrists. She had noticed a deformity in both forearms at the age of 6 years. She had no significant family or medical history. Her height was 138 cm (the average height of an 11-year-old Japanese girl is 148 cm), and she presented with a sword bayonet-like deformity without any wrist pain. Wrist extension and forearm pronation were restricted. The wrist extension was 30° on the right and 35° on the left, flexion was 105° to 100°, the forearm pronation was 55° on the right and 60° on the left, and supination was 85° to 80°.
A plain radiograph revealed shortening of the radius with abnormal joint inclination and relative protrusion of the distal ulna (Figure 1). The radial head was atrophic and had no radiocapitellar contact in the right elbow, and the left radiocapitellar joint was wide on a lateral radiograph. The radiographic parameters are listed in Table 1. The radial inclination was 43° on the right and 42° on the left.
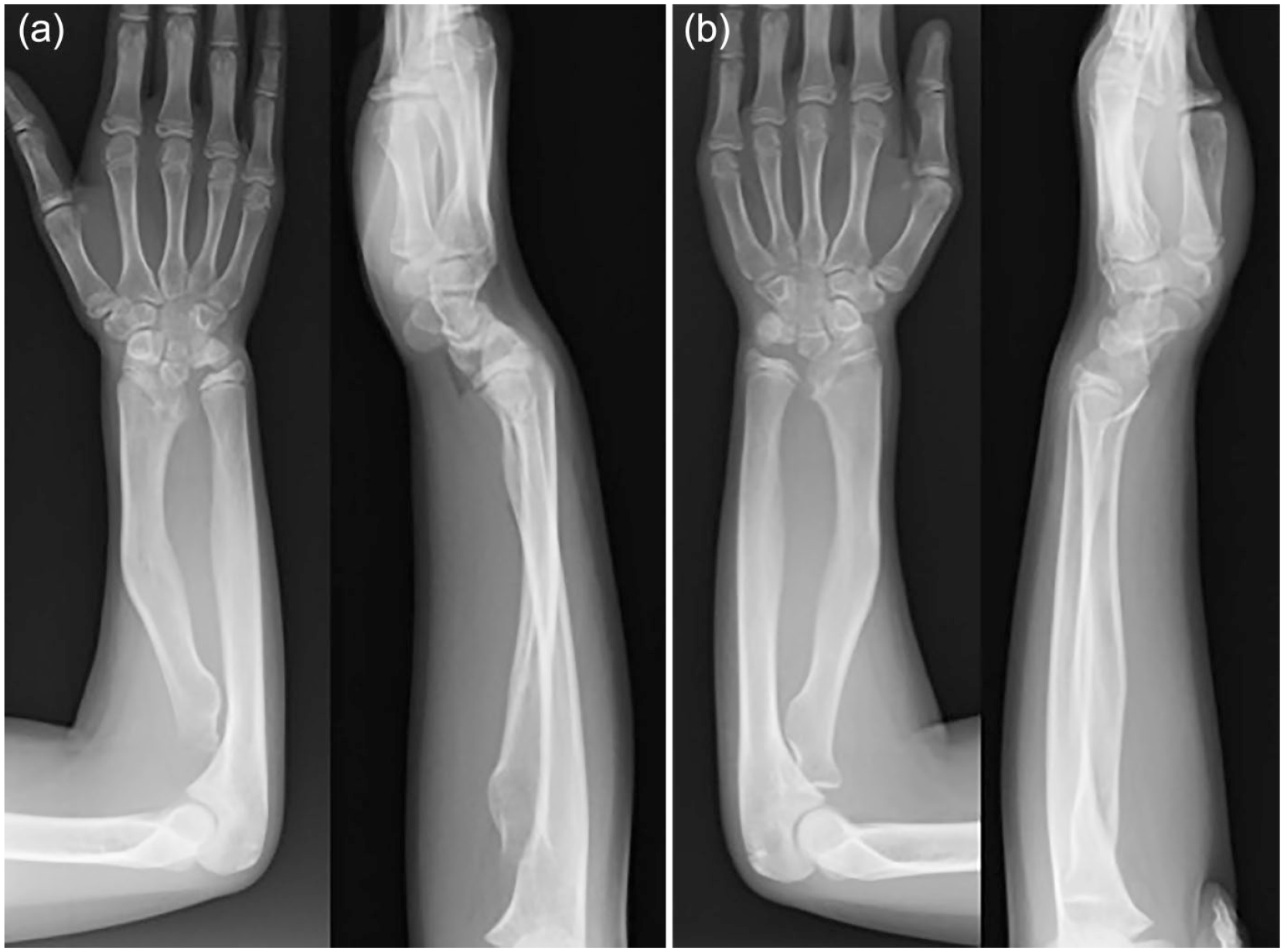
Preoperative radiography performed at 10 years of age revealed severe shortening of the radius and deformity of the distal radius.
Radiographic Parameters.
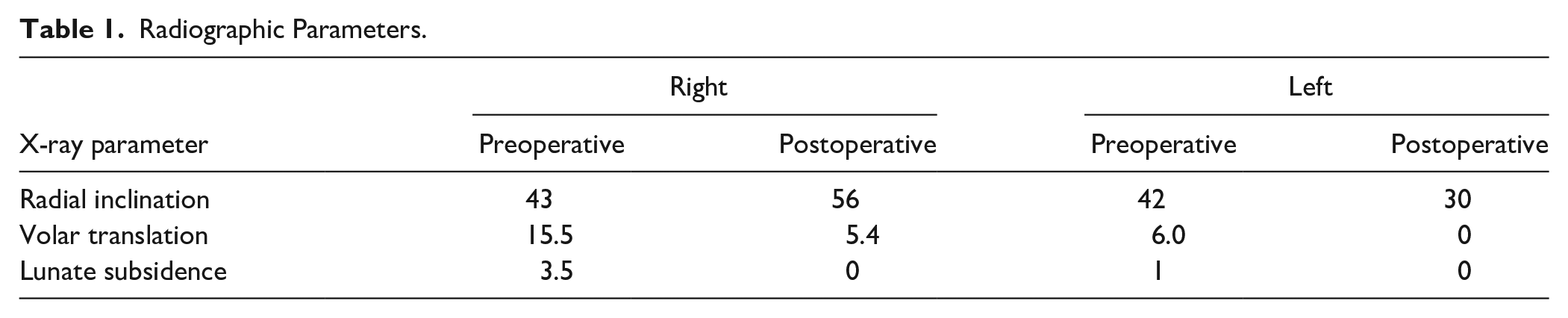
We defined volar translation (VT) as an index of volar displacement of the carpus. Volar translation is the distance from the radial axis to the center of the capitate head on a lateral radiograph. The radial axis is drawn from the midpoint of the radial head to the midpoint of the distal metaphysis. Lunate subsidence (LS) is defined as an index of the proximal migration of the carpus; it is the distance between the most proximal aspect of the lunate and the articular surface of the ulnar head on the anteroposterior radiograph, measured perpendicular to the ulnar axis. The VT was 15.5 mm on the right and 6.0 mm on the left, and LS was 3.5 and 1 mm, respectively.
Arthrography of the right elbow revealed that the radial head was in good shape, and it was possible to regain the normal radiocapitellar contact (Figure 2). Although the patient was almost asymptomatic except for the present deformity, it was anticipated that the deformity could lead to pain in the near future. Therefore, surgery was planned to prevent severe forearm disorder.
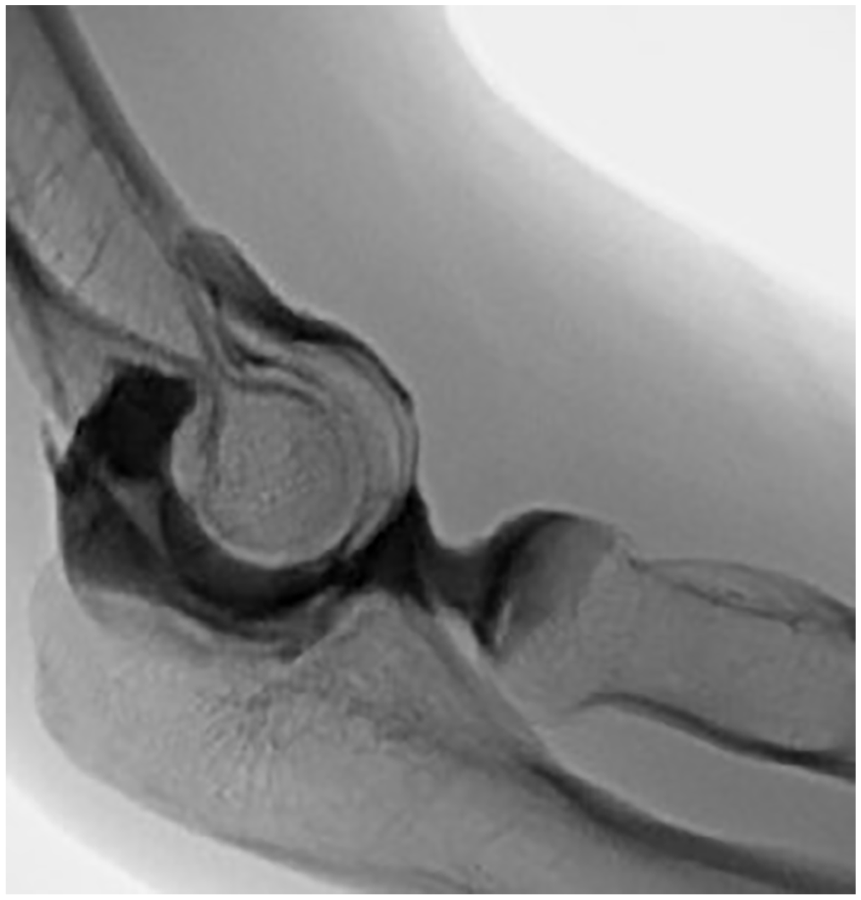
Arthrography revealed that there was no deformity of the radial head. The joint capsule was smooth, allowing the reduction of the joint.
Surgical Procedure
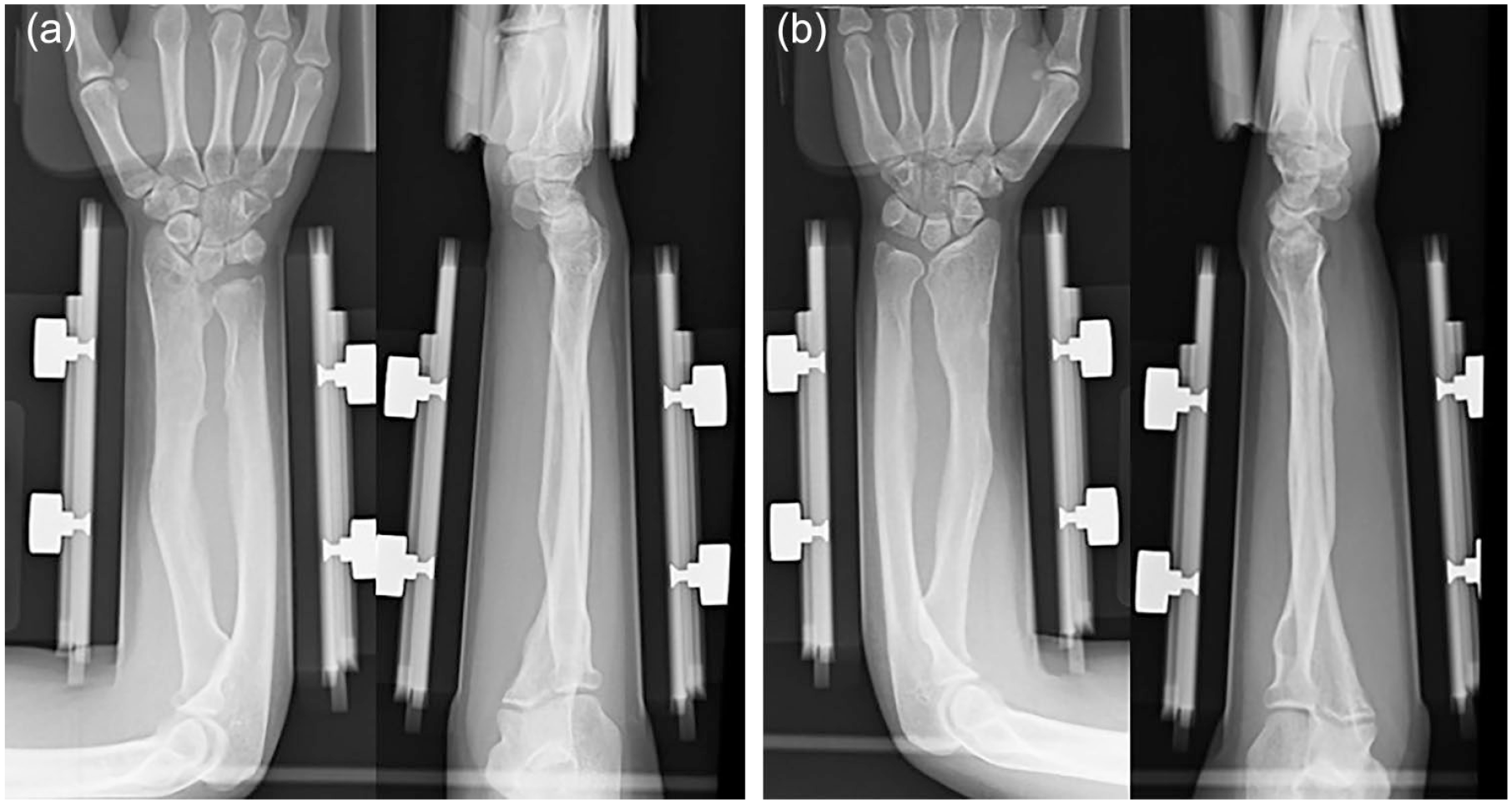
Surgery of the left side was scheduled first. It was performed under general anesthesia with an upper arm tourniquet. The distal radius was exposed through a volar incision, and the Vickers ligament was detached from the radial rim. An osteotomy was performed at the metaphysis of the radius, and the distal fragment was rotated to correct the radial inclination and the volar tilt. An external fixator was applied to maintain this correction and lengthen the radius (Figure 3). Callus distraction was started at 0.5 mm per day after 10 days of waiting. After 3.5 months, a similar surgery was performed on the right side.
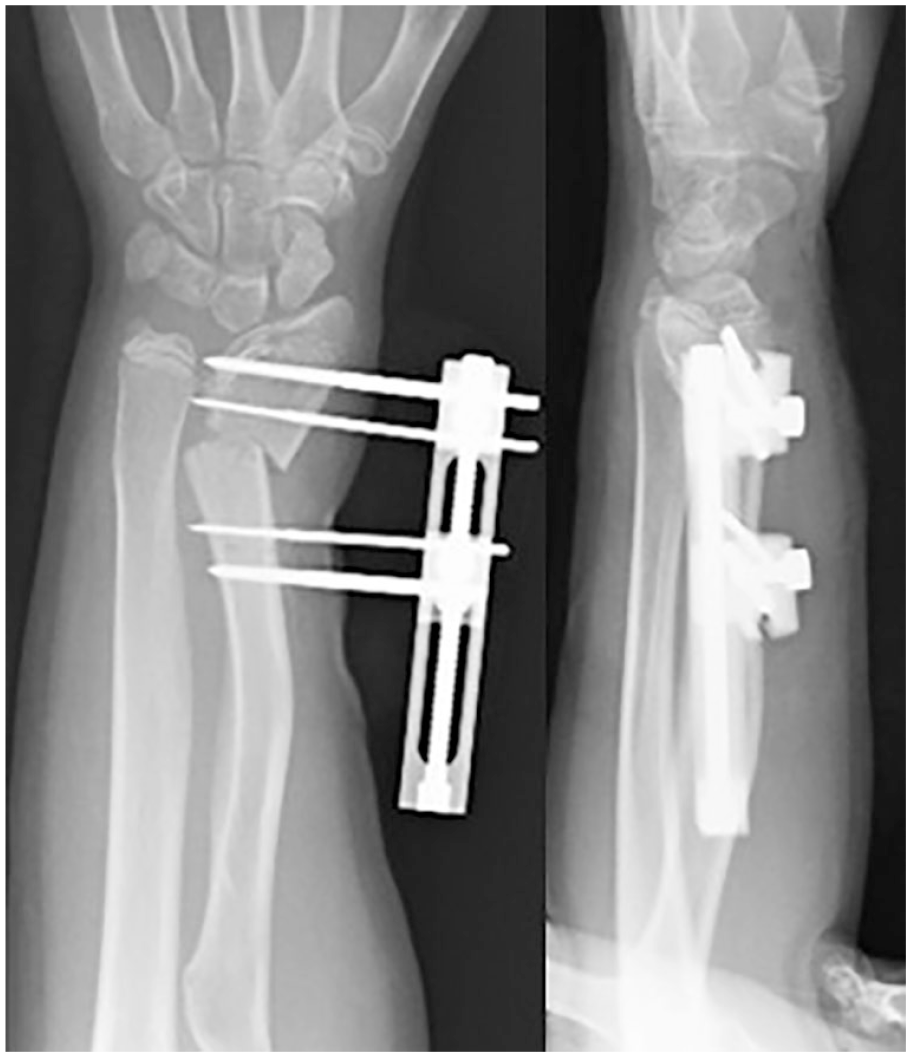
The distal radial fragment was rotated to improve radial inclination. The external fixator was subsequently applied.
Postoperative Results
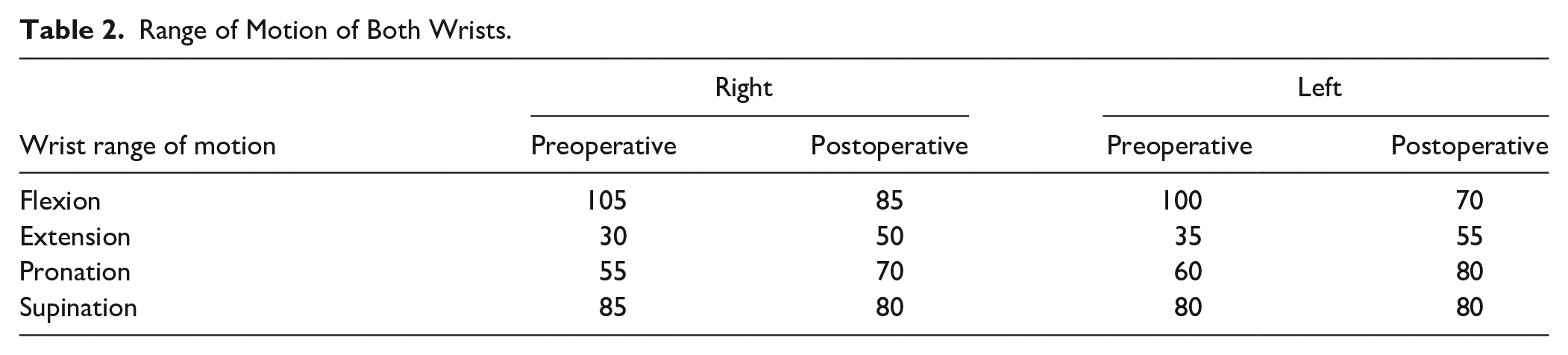
No perioperative complication, such as infection, was noted. The fixator was removed on day 117 on the right and day 88 on the left side. The total distractions were 27.8 and 8.1 mm, and the healing indexes were 42 and 108 days/cm, respectively, on the right and left sides. Callus distraction at the distal radius affected the elbow, and the radiocapitellar joint was spontaneously reduced to obtain a good contact. Forty-three months after surgery, the patient had no pain or difficulties in performing daily activities. The wrist extension was 50° on the right and 55° on the left, flexion was 85° to 70°, forearm pronation was 70° to 80°, and supination was 80° to 80° (Table 2). The radial deviations were 0°, the ulnar deviations were 40° and 35°, and the grip strengths were 26 and 24 kg, respectively, on the right and left sides. Radiography revealed that the overall forearm deformity improved, and the stable radiocapitellar joint alignment was maintained in the right elbow (Figure 4). The radial inclination changed from 43° to 56° on the right and 42° to 30° on the left. The VT changed from 15.5 to 5.4 mm on the right and 6.0 to 0 mm on the left. The LS changed from 3.5 to 0 mm on the right and 1 to 0 mm on the left (Table 1).
Radiographs after 3.5 years of surgery. Bone maturation was completed.
Range of Motion of Both Wrists.
Discussion
Madelung deformity leads to various other deformities due to growth disturbances in the distal radius resulting in wrist and forearm disorders. Treatment should be considered according to patients’ age and the degree of deformity. Generally, conservative treatment is an option for patients with subtle symptoms and deformities; however, surgery is indicated for cases with severe and progressive deformity.
Physiolysis (Langenskiöld procedure) or Vickers ligament resection is a method to release growth arrest and regain bone growth. These procedures are suitable for skeletally immature patients. Steinmann et al 1 reported that the release of the volar ligament improved the radiocarpal joint alignment. Del Core et al 2 reported that although the pain was reduced by Vickers ligament resection, the LS showed a substantial increase. Some benefits of these procedures have been reported; however, simultaneous ulnar shortening or additional secondary surgeries were needed due to residual deformities.2-5 It is difficult to predict how much growth can be regained only by these procedures because the influence on the growth plate starts at birth. Presently, the treatment modality for Madelung deformity is quite different from that for posttraumatic growth retardation.
Additional procedures should be considered to correct the deformity to prevent future hand disorders resulting in possible pain. Radius dome osteotomy is a useful procedure to correct 3-dimensional deformities.1,5 The inclination of the radial joint surface can be effectively corrected; nevertheless, large discrepancies between the radius and the ulna should be addressed by ulnar shortening procedures. However, there are no guidelines to specify the appropriate age to perform either epiphysiodesis or ulnar shortening. A retrospective study by Farr et al 6 reported that shortening osteotomy may be prevented by early ulnar epiphysiodesis in skeletally immature children aged >10 years. However, the forearm itself is already short; therefore, lengthening the short radius is more beneficial, avoiding invasion into the healthy ulna. This technique is a simple method in which the alignment of the radius can be corrected by one skin incision and the balance with the ulna can be adjusted by callus distraction. More sophisticated techniques, such as computer simulation or the usage of a Taylor frame, have been reported to correct complicated 3-dimensional deformities.7-9 Although radiographic improvement might be superior to that observed with traditional osteotomies, the clinical superiority has not been clearly demonstrated. A Taylor frame might disturb not only pronation and supination of forearm but also daily use of operated hand while correcting deformity. Eventually, it would cause some impairments such as contracture. In addition, these procedures have some disadvantages in terms of cost and convenience for patients.
In this patient, the symptoms were subtle despite severe radiographic deformity. Zebala et al 10 reviewed radiographs of Madelung deformities and reported that these deformities affected either the entire radius or the distal radius. The entire radius of this patient was affected. It was predicted that both forearms, including elbows, would develop uncorrectable deformities, eventually severely affecting the activities of daily living. In addition, the patient was approaching the age when bone growth maturity would set in; thus, we could estimate how much length discrepancy between the radius and ulna should be corrected.
Vickers ligament sectioning was performed while expecting some improvement in the carpal alignment. Physiolysis was not indicated because of the patient’s age. Considering the shortness of the forearm and involvement of the radiocapitellar malalignment, we performed radius lengthening at the distal metaphysis, which eventually regained the radiocapitellar contact. Through a simple incision, all surgical procedures were performed without imposing on the ulna. Although the applied external fixator was quite cumbersome, the patient could use her hands and perform daily activities with minimum limitations during the treatment period.
The correction of the distal radial inclination was performed during surgery; therefore, radiographic parameters, such as radial inclination and volar tilt, were not completely corrected due to soft tissue constraints. Radial lengthening could increase radiocarpal pressure, resulting in wrist stiffness with pain. Our patient was followed up until bone maturity. The range of motion was well preserved without any pain, and the patient was also satisfied with the cosmetic outcomes. Based on the results, this surgical technique can be an option for managing Madelung deformity.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
Procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 and 2008.
Statement of Informed Consent
Informed consent was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.