
Abstract
Background:
The purpose of this study was to compare the demographic differences of the most common peripheral nerve compressions in the upper extremity—carpal tunnel syndrome (CTS), ulnar nerve compression (UNC) at the elbow, combined CTS and UNC, radial tunnel syndrome (RTS), and posterior interosseous nerve syndrome (PINS)—as a means to better understand the etiologies of each.
Methods:
A retrospective chart review was performed of all patients over the age of 18 years seen at our institution in the 2018 calendar year. International Classification of Diseases, Tenth Revision codes were used to identify patients with diagnoses of upper extremity peripheral nerve compressions. Demographic details and relevant comorbidities were recorded for each patient and compared with controls, who were seen the same calendar year with no neuropathies. χ2 analyses, independent-samples t tests, and multivariate logistic regressions were performed (P < .05).
Results:
A total of 7448 patients were identified. Those with CTS were mainly women, former smokers, and diabetic (all P < .001) and with a greater average body mass index (BMI) (P = .006) than controls. Patients with UNC were more often men and younger when compared with controls (both P < .001). A history of smoking, diabetes, and average BMI were similar between patients with UNC and controls (all P > .05). Those patients with combined CTS/UNC were mainly men, former smokers, and diabetic (all P < .001) when compared with controls. Patients with RTS/PINS were also mostly men (P = .007), diabetic (P = .042), and were more often current smokers (P < .001).
Conclusions:
The demographics of patients with various compressive neuropathies were not homogeneous, suggesting different etiologies.
Keywords
Introduction
Carpal tunnel syndrome (CTS), ulnar nerve compression at the elbow (UNC), combined carpal tunnel syndrome and ulnar nerve compression at the elbow (CTS/UNC), radial tunnel syndrome (RTS), and posterior interosseous nerve syndrome (PINS) involve compression of peripheral nerve(s) at specific anatomical sites in the upper extremity. Carpal tunnel syndrome, the most common compressive neuropathy, has an annual incidence rate of 2.3 cases per 100 person-years in the United States according to Dale et al. 1 Person-years are calculated by dividing the number of new cases of CTS during a specified time period by the total time each patient was observed. Carpal tunnel syndrome is associated with a variety of risk factors well-documented in the medical literature, which include: female sex,1-5 rheumatoid arthritis,4,6 diabetes mellitus,1,2,4,6,7 pregnancy,4,5 hypothyroidism,4,7 and a high body mass index (BMI).3-5 Postmenopausal women, in particular, have a higher risk of developing CTS.8,9 Ulnar nerve compression at the elbow, the second most common peripheral neuropathy, has an annual incidence of 30 cases per 100 000 person-years. 10 It generally occurs in men,2,4,10-13 those with diabetes,4,14,15 smokers,4,12,16 and those whose work activities require maintaining their elbows in flexed positions for prolonged periods of time, such as keyboard typing, talking on the telephone, or repetitive lifting of heavy objects.4,15,16
Despite substantial literature on the incidence and patient-specific factors associated with CTS and UNC as distinct neuropathies, there is a paucity of information for patients with combined CTS/UNC. Cross and Matullo 17 reported using endoscopic techniques to decompress carpal tunnels and cubital tunnels in men more than women but did not explain reasoning behind the sex difference or provide other demographic details. Seradge and Owen 18 noted that recurrences following cubital tunnel decompressions were significantly higher in patients who also had CTS, suggesting that patients with combined CTS/UNC who undergo surgical decompressions may be at a greater risk of recurrences.
Neuropathies of the radial nerve in the proximal forearm are the least common compressive neuropathies with an incidence of 0.002% to 0.03%.19-21 Although both RTS and PINS involve compression of the posterior interosseous nerve, the clinical presentations differ. Patients with RTS often complain of proximal forearm pain and tenderness, without any motor or sensory deficits.20-22 The tenderness is distinguished from that of lateral epicondylitis by its location. In RTS, the location of the tenderness is usually over the radial tunnel, several centimeters distal to the lateral epicondyle, whereas in a lateral epicondylitis, it is typically localized to the epicondyle at the origin of the extensor carpi radialis brevis.20-22 In contrast, PINS involves a motor deficit in digital extension that may not involve all the digits equally; pain is usually not a predominant symptom.21-23 Unlike CTS and UNC, PINS has no associated sensory deficits and is considered a “motor-only” dysfunction.22,24 Documented risk factors for RTS and PINS include prolonged compression of the forearm, humeral shaft fractures, rheumatoid arthritis, and various occupational factors in laborers.22,24-27 Other demographic associations have not been established, although a compressive neuropathy of at least one other nerve in the extremity has been documented in 17% to 20% of patients with radial nerve compressions.28,29
To our knowledge, this is the only study that seeks to directly compare the demographics of patients with various types of peripheral neuropathies. The aim of this study is to investigate demographic differences by analyzing a set of characteristics in each peripheral neuropathy group (CTS, UNC, combined CTS/UNC, RTS/PINS). We plan to compare our findings with previous literature as well as expand upon the results of past studies by investigating many types of peripheral neuropathies. As neuropathies in the upper extremities are very common, physicians should have an understanding of the demographic factors associated with them for proper diagnosis and treatment. The purpose of our study was to: (1) confirm that CTS, UNC, combined CTS/UNC, and radial nerve compressions (RTS and PINS) commonly affect distinct demographic groups; and (2) identify the differences among the groups to inform physicians of differences in etiology.
Materials and Methods
Our retrospective chart review study was approved by the institutional review board of our medical center. Electronic medical records were accessed to identify all adult patients (≥18 years old) who were seen during the 2018 calendar year. The International Classification of Diseases, Tenth Revision, Clinical Manifestation (ICD-10-CM) was used for the following diagnostic codes: G56.00, G56.01, G56.02, G56.03, G56.10, G56.11, G56.12, G56.13, G56.20, G56.21, G56.22, G56.23, G56.30, G56.31, and G56.32. RTS and PINS diagnoses comprised the fewest number of patients and were thus grouped together in one cohort. All traumatic PINS patients were excluded.
Patient-specific data of age, sex, race, alcohol use, smoking status, and comorbidities, including diabetes, osteoarthritis, rheumatoid arthritis, elevated high-density lipoproteins (HDLs), and hypertriglyceridemia, and average BMI were collected. Patients were divided into female and male groups, and those above and below the age of 50 years to further investigate the relationship of age and sex on peripheral neuropathies. Race was divided based on the grouping used in our institution’s electronic medical record (EMR) system. Occupation was seldom reported systematically in the EMR system, but when available, it was recorded and categorized into one of seven categories (heavy labor, light labor, office job, retired, unemployed, student, or caretaker).
Sex, age, smoking status, the presence of comorbidities (diabetes, arthritis, high HDL, and hypertriglyceridemia), BMI, and occupation were investigated because these characteristics have been studied in the past in at least one of the peripheral neuropathy groups. Alcohol use was included in our analysis because it is known that a high percentage of alcoholics experience polyneuropathy, and further investigation is needed to study a similar association between alcohol use and presence of a mononeuropathy. 4 Finally, race was included in our analysis because it is a commonly collected demographic variable that has not been investigated in this context.
The control group consisted of 991,815 patients who were seen at our institution in 2018 and had no history or clinical signs of a peripheral neuropathy in their upper extremities. χ2 analyses for categorical variables and independent-samples t tests for continuous variables were performed for the peripheral neuropathy cohorts. Multivariate logistic regressions were run for peripheral neuropathy diagnoses. Statistical significance was set at P < .05.
Results
Carpal Tunnel Syndrome
A total of 5726 patients were diagnosed with CTS. Compared to controls, they were mainly women (CTS: 70.9% vs control: 59.0%, P < .001) with an average age of 57.2 ± 16.0 years, compared to an average age of 52.5 ± 18.6 years for controls. Women aged ≥50 years comprised most of the patients with CTS (48.4% vs 32.6%, P < .001) compared with those aged <50 years (22.5% vs 26.4%, P < .001). There were significantly fewer men in both age groups (<50 years: 8.7% vs 16.6%, P < .001, and ≥50 years: 20.3% vs 24.4%, P < .001). Caucasian (66.3% vs 69.5%, P < .001) and Asian (4.9% vs 5.8%, P = .004) subjects were less prevalent among CTS subjects compared with institutional controls, whereas Black, Pacific Islander, Native American, and other race subjects were more prevalent (all P < .05). Patients with CTS included fewer users of alcohol (48.1% vs 51.9%, P < .001) and more former smokers than current smokers (30.1% vs 26.0%, P < .001). There were a significantly greater number of patients with diabetes (10.0% vs 5.9%, P < .001) and high HDL (13.6% vs 11.1%, P < .001) than in the control group. The presence of rheumatoid arthritis (5.6% vs 2.0%, P < .001) and osteoarthritis (41.4% vs 18.6%, P < .001) was higher in the cohort of patients with CTS when compared with controls. Patients with CTS also had a higher average BMI (29.6 ± 6.6 vs 28.3 ± 37.0, P = .006) (Supplementary Table 1). A greater number of patients with CTS were retired (46.8% vs 40.5%, P = .002), whereas a lesser number of those with CTS were students (0.5% vs 2.4%, P < .001) when compared with controls (Supplementary Table 2).
Multivariate logistic regression determined that both male (odds ratio [OR]: 1.160, 95% confidence interval [CI]: 1.049-1.281, P = .004) and female patients (OR: 2.003, 95% CI: 1.845-2.174, P < .001) aged ≥50 years were more likely than their younger counterparts, <50 years old, to be diagnosed with CTS. Diabetes (OR: 1.501, 95% CI: 1.355-1.662, P < .001) and rheumatoid arthritis (OR: 2.225, 95% CI: 1.934-2.559, P < .001) also had a high association with a CTS diagnosis. Caucasian patients (OR: 0.794, 95% CI: 0.739-0.853, P < .001) and those who had never smoked (OR: 0.848, 95% CI: 0.790-0.910, P < .001) were associated with a lesser likelihood of being diagnosed with CTS (Table 1).
Multivariate Logistic Regression to Carpal Tunnel Syndrome.
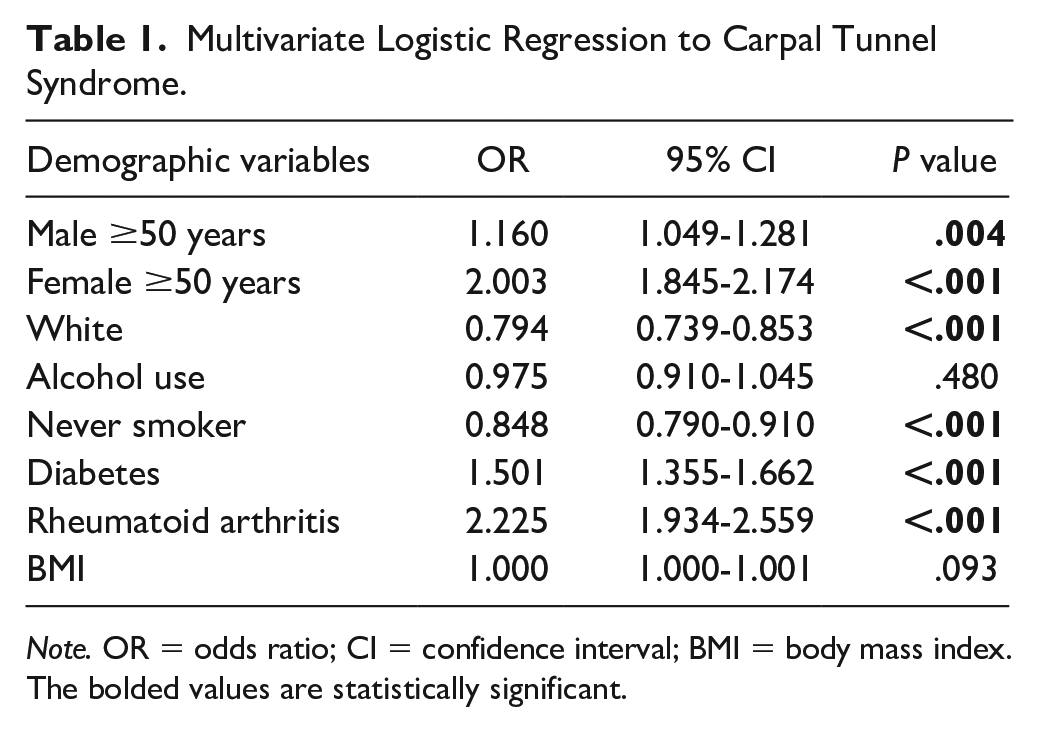
Note. OR = odds ratio; CI = confidence interval; BMI = body mass index.
The bolded values are statistically significant.
Ulnar Nerve Compression
A total of 904 patients were diagnosed with UNC. A greater proportion of patients with UNC were men (51.9% vs 41.0%, P < .001) compared with controls and were also younger (48.5 ± 15.9 years vs 52.5 ± 18.6 years, P < .001). The UNC cohort had more men <50 years (25.4% vs 16.6%, P < .001) and fewer women ≥50 years (22.1% vs 32.6%, P < .001). Alcohol use (58.8% vs 52.6%, P = .001) and those patients diagnosed with hypertriglyceridemia (1.3% vs 0.7%, P = .024) were more prevalent, whereas patients with high HDL (8.5% vs 11.1%, P = .013) were less prevalent. Rheumatoid arthritis (3.4% vs 2.0%, P = .003) and osteoarthritis (28.4% vs 18.7%, P < .001) were more prevalent in the UNC cohort as well. Race, smoking status, diabetes, and average BMI distributions did not significantly differ between patients with UNC and controls (all P > .05) (Supplementary Table 3). Ulnar nerve compression was not found to be associated with any occupation category (Supplementary Table 4).
Multivariate logistic regression determined that women aged ≥50 years were less likely to be diagnosed with UNC (OR: 0.656, 95% CI: 0.530-0.811, P < .001), whereas alcohol users (OR: 1.334, 95% CI: 1.119-1.591], P = .001) and those with rheumatoid arthritis (OR: 2.313, 95% CI: 1.554-1.008, P < .001) were more likely to be diagnosed (Table 2).
Multivariate Logistic Regression to Ulnar Nerve Compression.
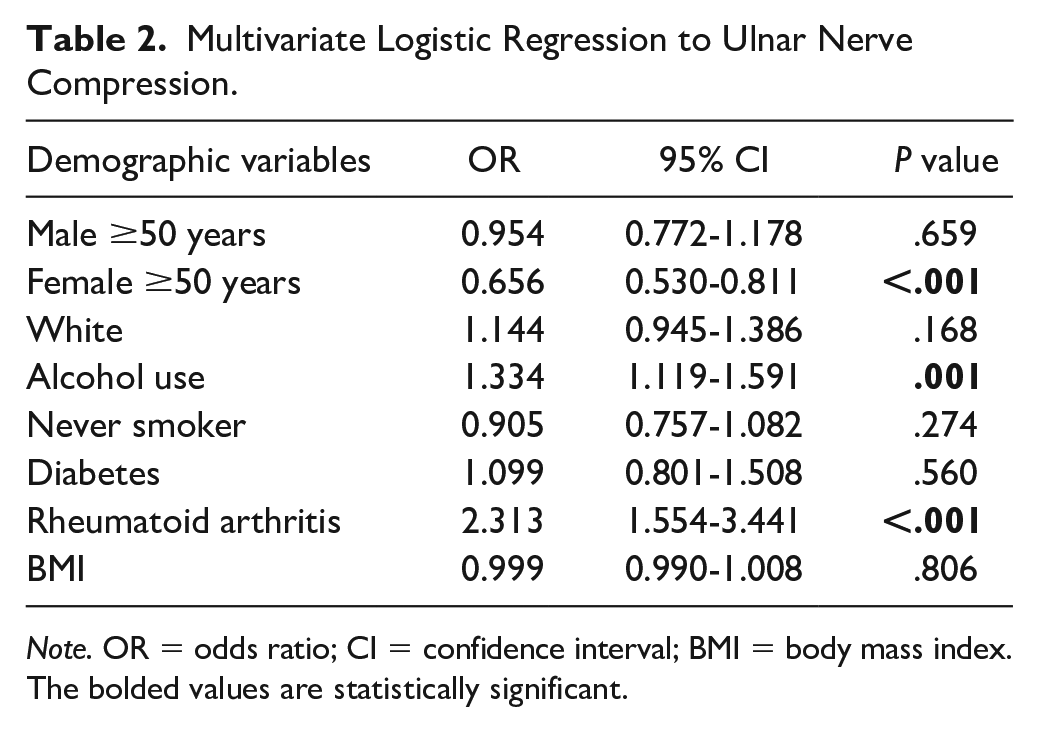
Note. OR = odds ratio; CI = confidence interval; BMI = body mass index.
The bolded values are statistically significant.
Combined CTS and UNC
A total of 657 patients were identified as having combined CTS and UNC. There were a higher proportion of men (47.9% vs 41.0%, P < .001), and patients were older (56.3 ± 14.8 years vs 52.5 ± 18.6 years, P < .001) when compared to controls. Specifically, the CTS/UNC cohort contained more men aged ≥50 years (35.5% vs 24.4%, P < .001) than those aged <50 years (12.5% vs 16.6%, P = .005) and women aged <50 years (17.7% vs 26.4%, P < .001). Black subjects (15.2% vs 12.1%, P = .017) were more prevalent in the CTS/UNC group compared with White, Asian, Pacific Islander, and Native American subjects. Former smokers (38.0% vs 26.0%, P < .001), patients with diabetes (10.7% vs 5.9%, P < .001), patients with hypertriglyceridemia (1.4% vs 0.7%, P = .048), patients with rheumatoid arthritis (3.3% vs 2.0%, P = .019), and patients with osteoarthritis (40.2% vs 18.7%, P < .001) were also more prevalent in the CTS/UNC cohort. Alcohol use, average BMI, and occupation did not differ among the cohorts (all P > .05) (Supplementary Tables 5 and 6).
Men (OR: 1.967, 95% CI: 1.526-2.559, P < .001) and women (OR: 1.515, 95% CI: 1.174-1.956, P = .001) aged ≥50 years were found to have a higher likelihood of being diagnosed with combined CTS and UNC according to multivariate logistic regression. Diabetes (OR: 1.707, 95% CI: 1.296-2.248, P < 0.001) is also related to a higher likelihood of a combined diagnosis, whereas having never smoked (OR: 0.670, 95% CI: 0.550-0.817, P < .001) is related to a lesser likelihood (Table 3).
Multivariate Logistic Regression to Concomitant CTS/UNC.
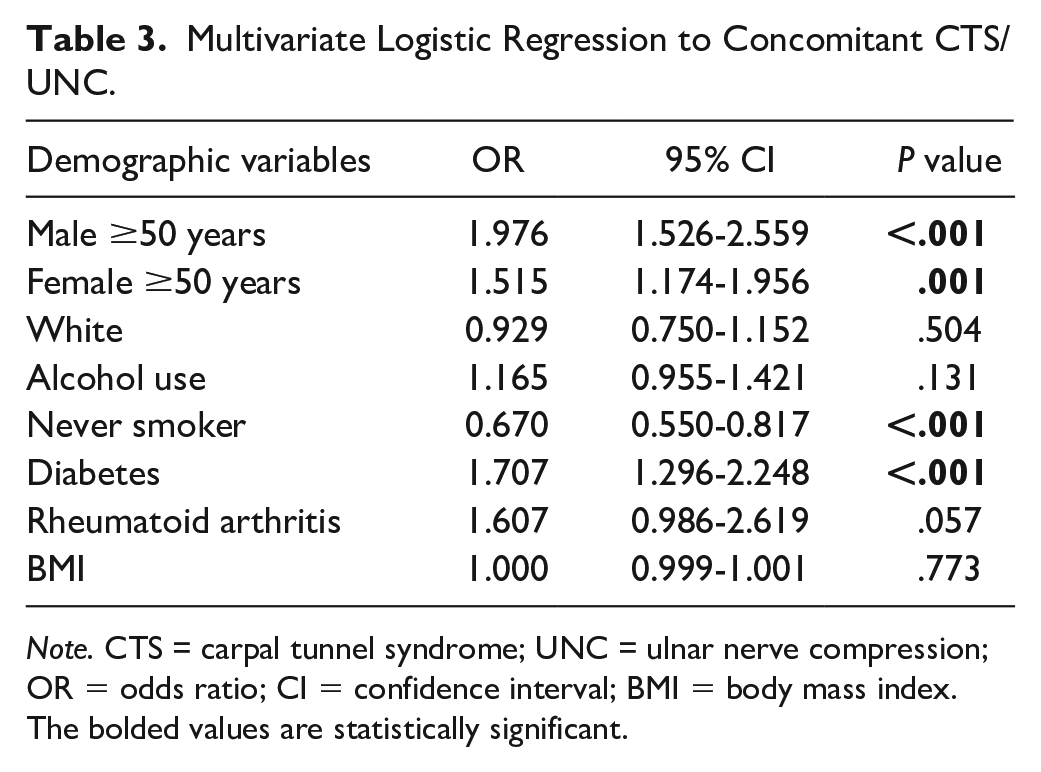
Note. CTS = carpal tunnel syndrome; UNC = ulnar nerve compression; OR = odds ratio; CI = confidence interval; BMI = body mass index.
The bolded values are statistically significant.
Radial Nerve Compressions
A total of 151 patients were identified (132 RTS and 19 PINS). A greater proportion of this cohort were men (54.3% vs 41.0%, P = .001) compared with the control group. There was a higher proportion of men over 50 (33.1% vs 24.4%, P = .013), current smokers (20.2% vs 8.6%, P < .001), and patients with osteoarthritis (32.5% vs 18.7%, P < .001) in the RTS/PINS cohort and a lower proportion of women over 50 (23.2% vs 32.6%, P = .012). Race, alcohol use, diabetes, smoking status, average BMI, and occupation did not differ between patients with RTS/PINS and controls (all P > .05) (Supplementary Tables 7 and 8). Multivariate logistic regression did not find any correlations (all P > .05) (Table 4).
Multivariate Logistic Regression to RTS/PINS.
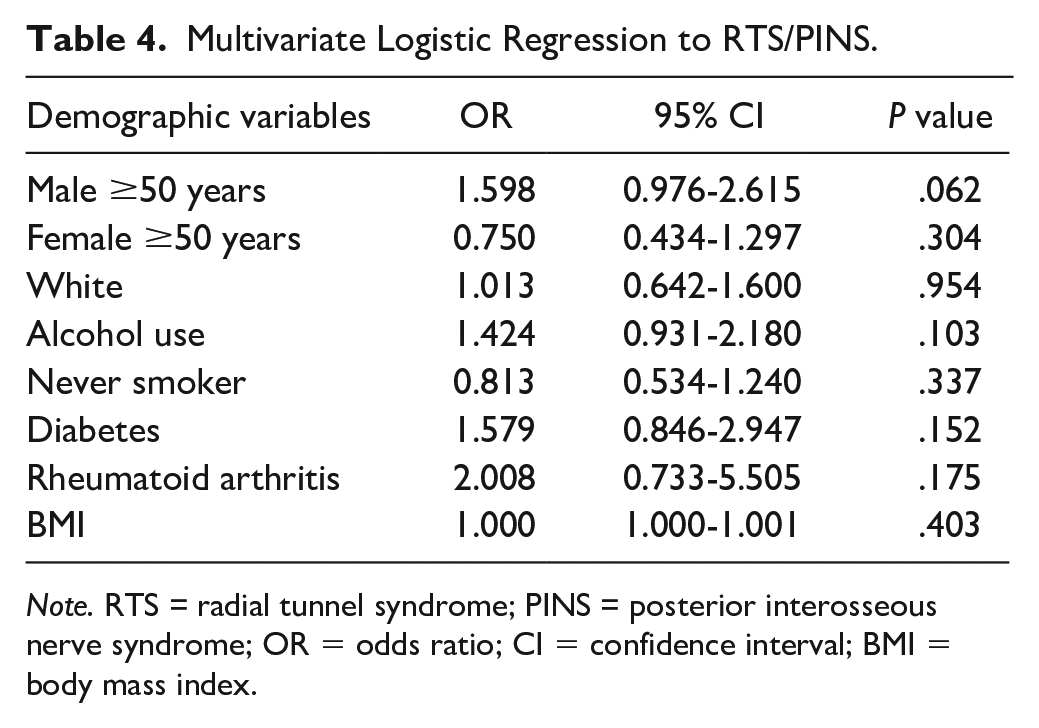
Note. RTS = radial tunnel syndrome; PINS = posterior interosseous nerve syndrome; OR = odds ratio; CI = confidence interval; BMI = body mass index.
Discussion
Our results show that patient demographics are not homogeneous among patient populations with different compressive neuropathies in the upper extremity (Table 5). By comparing patients with CTS with controls at our institution, we identified older women, as well as smoking, diabetes, higher HDL, rheumatoid arthritis, osteoarthritis, and higher BMI to be highly associated with developing CTS. Our results are consistent with the medical literature.2-7 It has been suggested by other authors that the higher incidence in older women, who are most likely postmenopausal, is likely related to a decrease in estrogen levels during menopause and that estrogen could play a protective role in developing CTS.8,9 We also found a low incidence of CTS among the Asian population. However, we believe that this is reflective of the demographics at our institution and would benefit from further investigation in a multi-institutional study. Finally, our analysis of occupation showed that more retirees have CTS while less students have CTS. This supports the known finding that older individuals are more at risk of developing CTS.
Characteristics Associated With Peripheral Neuropathy.
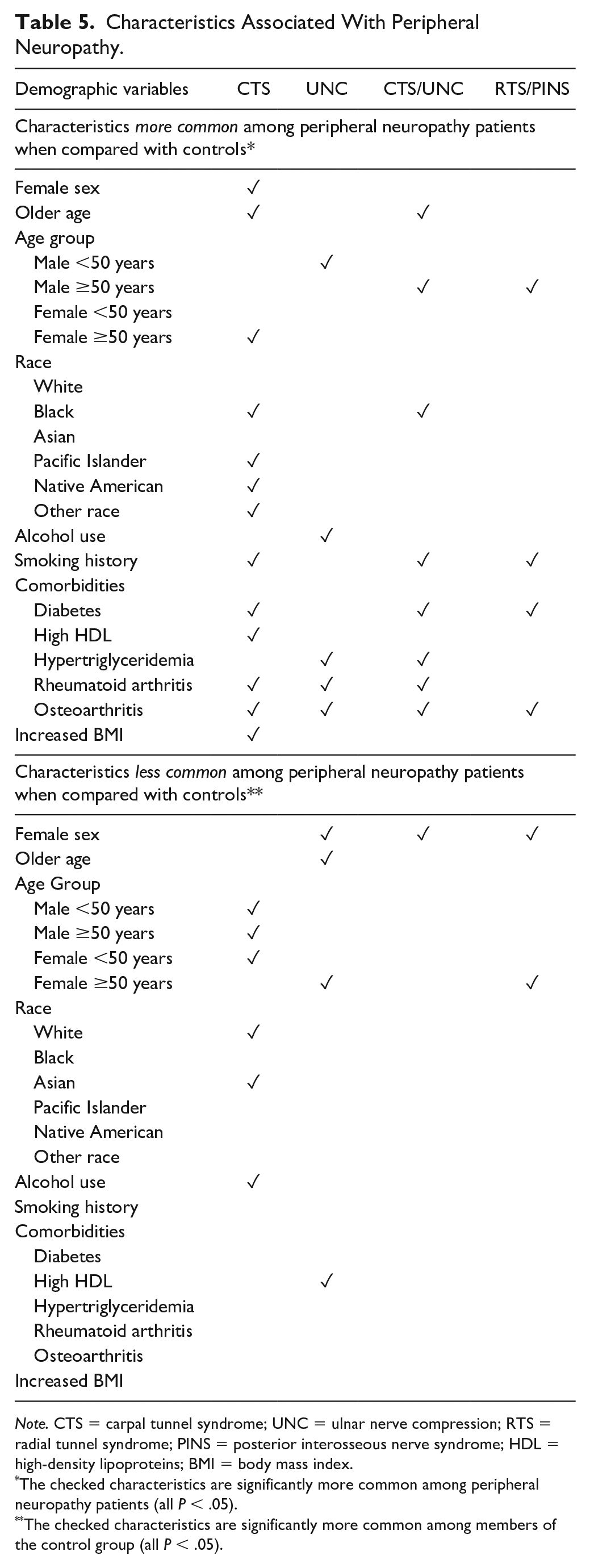
Note. CTS = carpal tunnel syndrome; UNC = ulnar nerve compression; RTS = radial tunnel syndrome; PINS = posterior interosseous nerve syndrome; HDL = high-density lipoproteins; BMI = body mass index.
The checked characteristics are significantly more common among peripheral neuropathy patients (all P < .05).
The checked characteristics are significantly more common among members of the control group (all P < .05).
Regarding UNC at the elbow, our data indicate that men, alcohol use, and a diagnosis of hypertriglyceridemia, rheumatoid arthritis, and osteoarthritis are all strong demographic factors. Our results correspond with previous findings that men are more likely to develop UNC. However, other factors associated with UNC are less well established.2,4,10-13 Similar to Richardson et al, 13 Bartels and Verbeek, 16 and Uzunkulaoğlu et al, 11 we found that a diagnosis of UNC at the elbow was independent of BMI. This differs from the findings of Mondelli et al, who found a high BMI association with UNC. 12 We found no such association between our UNC cohort and diabetes that contradicts other published findings on “diabetic neuropathies” which show that people with diabetes are more likely to have nerve compressions of all types.7,14,15,30 Contrary to our CTS cohort, a greater number of women aged <50 years developed UNC and a greater proportion of men of all ages were diagnosed with UNC. Unlike previous literature that suggests heavy labor jobs or occupations requiring repetitive computer work are at high risk of developing UNC, we did not find an association with UNC and occupation in our population. Race was found to have no impact on the diagnosis of UNC.
Consistent with the findings of Zhang et al 5 that surgical CTS and UNC patients are not homogeneous, we found that our population of patients with combined CTS and UNC differed demographically. Men in an older age group, smoking, diabetes, hypertriglyceridemia, rheumatoid arthritis, and osteoarthritis were all associated with combined neuropathies. Black patients also had a higher incidence of combined CTS/UNC. The older age group as a possible risk factor, regardless of the sex, could support the concept that prolonged hand usage over many decades promotes combined CTS and UNC.4,15,16,31 This concept has been explored in the context of patients with CTS and UNC separately but not when they occur together. These findings suggest a possible divergence in etiology and emphasize the need for further investigation into those with combined CTS/UNC.
Interestingly, more former than current smokers are noted in the combined CTS/UNC group as well as the CTS group. Although this could indicate that a smoking history somehow has a protective effect on compressive neuropathy, it is also possible that this is reflective of an older population who is more likely to have quit smoking. Our current analysis cannot confirm this hypothesis.
Radial nerve compressions RTS and PINS were the least common neuropathies among the entire patient group. Similar to studies done on English and Finnish populations, we found that the majority of our patients with RTS/PINS were men.19,32 That contradicts the findings of Moradi et al, 20 who found that RTS was most prevalent in women in the United States in the 30-50 age range. The average age of the RTS/PINS cohort in our study was 52.2 ± 15.6 years, although our data were not limited to RTS surgical patients as in other studies.20,27,28,33 A history of smoking and osteoarthritis were the only other associations identified in our analysis, although they are not unique to patients with RTS/PINS. Demographic factors that may affect the development of radial nerve compressions seem unrelated to increased BMI or race.
A possible limitation of the analysis of patients with radial nerve compression is the accuracy of the diagnosis of RTS. As previously discussed, RTS can easily be confused with lateral epicondylitis due to similar clinical presentations. Although an inaccurate diagnosis of RTS is possible in some of the patients, our findings differ from previous findings on demographic factors associated with lateral epicondylitis, suggesting that our population includes patients with RTS/PINS as opposed to those with lateral epicondylitis. For example, Park et al 34 characterized their population of patients with lateral epicondylitis as being of female sex with hypertriglyceridemia, which were not associations found in our RTS/PINS cohort. Further investigation is required to better characterize the at-risk populations for radial nerve compressions.
In summary, our data show that CTS, UNC, combined CTS/UNC, and RTS/PINS affect varying populations. In particular, CTS and UNC affect varying cohorts at our institution. In general, older individuals, both men and women aged 50 years and above, and those with rheumatoid or osteoarthritis are more prevalent in the peripheral neuropathy populations. Diabetes is another associated factor across CTS, CTS/UNC, and RTS/PINS cohorts, which is consistent with previous studies.2,5-7,15,30 However, the majority of characteristics investigated in this study are not consistent among peripheral neuropathy groups. Considering the overall heterogeneity of affected populations, our findings increase the suspicion that CTS, UNC, and RTS/PINS have varying etiologies. These results can aid in further investigations of the risk factors associated with peripheral neuropathies and the etiology behind them. In addition, although some results had been previously established, this study provides updated data on a large population, which is useful for tracking demographic trends over time to establish whether they remain consistent among populations. Understanding the factors associated with peripheral neuropathies and the etiology behind them is important for proper diagnosis and treatment.
Our study is not without limitations. Due to the retrospective study design, miscoded information, missing data, and errors within patient medical records are possible. As these data are only from one institution in one geographic location, our study results may not be generalizable to the entire population. Our data collection relied heavily on the coding and documentation by physicians into their patient’s charts, which is subject to limited information, human error, or individual bias. The initial diagnosis of CTS, UNC, combined CTS/UNC, RTS, or PINS found in the medical records may have been incorrectly made as the ICD-10-CM code was entered into the system without confirmatory tests. The method used to assign patients into groups by age and sex, for example, women aged <50 years, possibly misrepresents our patients as 50 years was arbitrarily chosen. There were no other factors used to define these groups by age. In addition, there could be confounding variables present that were not investigated in this study, such as prior trauma or genetics. The severity of the diagnosis as assessed by nerve conduction studies was also not investigated, as this information was not feasible to obtain from such a large cohort. Finally, although our study establishes associations among demographic factors and diagnoses within our population, we cannot confirm causation. Given these limitations, future research should continue to compare the etiologies of peripheral compressive neuropathies.
Supplemental Material
sj-docx-1-han-10.1177_15589447221107701 – Supplemental material for Demographics of Common Compressive Neuropathies in the Upper Extremity
Supplemental material, sj-docx-1-han-10.1177_15589447221107701 for Demographics of Common Compressive Neuropathies in the Upper Extremity by Madeline C. Rocks, Megan R. Donnelly, Alexander Li, Steven Z. Glickel, Louis W. Catalano III, Martin Posner and Jacques H. Hacquebord in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
Ethical approval for this study involving human subjects was obtained from the institutional review board at our institution. Animal subjects were not used in this study.
Statement of Informed Consent
Informed consent was not sought for this article because this is a retrospective review study. A waiver of consent was granted by the institutional review board at our institution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.