
Abstract
Background:
The purpose of this study was to perform a biomechanical investigation on the effect of ulnar variance (UV) on the stability of the distal radioulnar joint (DRUJ) prior to and after DRUJ sectioning.
Methods:
Ten cadaveric forearm specimens were included in the study and baseline UV was assessed radiographically. Radial motion relative to the ulna was evaluated using Intel real sense cameras and a custom developed program. The forearms were dissected, and a radial osteotomy was performed. Using a custom-made plate, radial stability was assessed with an UV of + 4, 0, and −4 mm by measuring the maximum and minimum radial position relative to the ulna during a simulated Shuck test. The volar radioulnar ligaments and triangular fibrocartilage complex (TFCC) were then sectioned, and testing was repeated at each UV state.
Results:
Sectioning significantly increased radial translation at neutral (P = .008), +4 mm UV (P = .008), and −4 mm UV (P = .018). There were no significant differences in translation between the 3 UV groups with the DRUJ intact (P = .124). The ulnar negative (−4 mm) state had significantly lower translation compared to the positive (+4 mm) (P < .001) and the neutral (0 mm) (P = .026) UV states. There were no significant differences between the positive and neutral UV groups with the DRUJ sectioned.
Conclusions:
Fixating the radius in −4 mm of ulnar negativity significantly decreased radial translation after sectioning the volar radioulnar ligament and TFCC. Ulnar variance had no effect on stability with an intact DRUJ.
Study Type:
Biomechanical Study
Introduction
Distal radius fractures (DRFs) are one of the most common upper extremity fractures. 1 One potential complication of DRFs is distal radioulnar joint (DRUJ) instability, especially in the setting of malunions. The DRUJ is stabilized primarily by the superficial and deep radioulnar ligaments but other structures, such as the ulnocarpal ligaments, triangular fibrocartilage complex (TFCC), extensor carpi ulnaris (ECU) sheath, pronator quadratus muscle, and interosseous membrane, as well as osseous restraints, also contribute to stabilization.2,3 After a DRF, there is significant risk of compromise of one or more of these ligaments, which could lead to instability. Distal radioulnar joint instability can result in ulnar sided pain, grip strength weakness, and limited forearm rotation.4,5 Many surgeries have been described to treat subsequent DRUJ instability, falling into 2 categories: reconstructions, such as the Adams-Berger procedure, or salvage operations, such as the Darrach procedure or Sauve-Kapandji procedure.6 -13 These procedures are generally intended for ligamentous injury. Distal radioulnar joint instability after a DRF can be due to ligamentous laxity from a change in ulnar-radial length relationship. Ideally, DRUJ instability after a DRF could be treated during the DRF open reduction and internal fixation (ORIF), thus eliminating the need for an additional surgery.
Prior studies have investigated various factors and approaches that may negate subsequent DRUJ instability after a DRF. For example, Bessho et al 14 reported that DRFs with a decreased radial angulation have increased stiffness in both the setting of an intact or partially sectioned radial ulnar ligament (RUL). Specifically, they suggested that 10° of radial angulation from the original radial inclination should be achieved intraoperatively to minimize the risk of postoperative DRUJ instability. The authors hypothesized that minimizing the radial angulation increased the length of the TFCC, a stabilizer of the DRUJ, thus increasing its tension and resulting in increased DRUJ stability. Similarly, biomechanics studies have demonstrated that ulnar shortening increases the stiffness of the DRUJ through a similar mechanism. 15
Given these biomechanics findings and that ulnar shortening can be accomplished either with an ulnar shortening osteotomy or with radial lengthening via distraction, we postulated that intraoperative ulnar variance (UV), not just ulnar length, may play a significant role in postoperative DRUJ stability. 16
Based on the clinical and biomechanical alterations associated with changes in UV and postoperative observations within our patient population, we hypothesized increasing that ulnar negativity compared to a patient’s baseline may tighten the DRUJ, thus improving stability, after RUL compromise. Therefore, the purpose of this study was to perform a biomechanical investigation on the effect of increasing ulnar positivity and increasing ulnar negativity on the stability of the DRUJ prior to and after DRUJ sectioning. We hypothesized that ulnar negativity would correlate with increasing DRUJ stability in both the DRUJ intact and DRUJ disrupted state.
Materials and Methods
Due to the cadaveric nature of this study, institutional review board approval was not required. No funding was received for this study. Ten cadaveric specimens (ScienceCare, Phoenix, Arizona) were utilized for this study. Prior to testing, all specimens underwent standard posterior-anterior (PA) wrist X-rays to evaluate for the presence of significant osteoarthritis (OA), radiographic factors associated with DRUJ instability (eg, widening of the distal radioulnar space), and baseline UV. 17 The wrist was set in pronation with 90 degrees of elbow flexion and a single investigator measured UV. Ulnar variance was measured as the absolute value of the difference between a line parallel to the distal edge of the radial articular surface (sigmoid notch) with another line parallel to the distal apex of the ulnar head.
After confirming that the cadaveric specimens demonstrated no radiographic indications of DRUJ instability, all specimens were thawed for 24 hours at room temperature. Piano key shuck maneuvers were performed to determine stability prior to operating on the wrists. The wrists were then prepared for testing. A fish-mouth incision was made along the volar and dorsal aspect of the wrist. Visual confirmation of an intact DRUJ was made upon dissection. After superficial dissection, all dorsal structures were left intact, while all of the flexor tendons were sectioned to allow adequate visualization of the radius and ulna for biomechanical testing. The flexor carpi radialis and flexor pollicis longus were retracted and the protractor quadratus was reflected to expose the radial shaft. A transverse extraarticular radial osteotomy was then performed. A 3D printed osteotomy guide set at 6 mm was used to create the radial osteotomy and then a custom distal radius plate (Trimed, Santa Clarita, California) was used, which had notches every 2 mm so that changes in UV could be performed by directly altering the plate (Figure 1). A 6 mm osteotomy was selected because a maximum of + 4 mm and −4 mm UV was being tested, and the maximum baseline UV was 2 mm of the specimens. A maximum and minimum UV of 4 mm were chosen on prior literature. A prior clinical study by Jianda et al, 18 for example, suggested that positive UV greater than 2.5 mm is associated with increased DRUJ instability. In addition, a finite element analysis study by Greybe et al, 19 which evaluated the effect of ulnar shortening, found that DRUJ contact pressures peaked at −3 mm, while contact area peaked at 4 mm of shortening in a model based on someone with natural negative UV. Based on these prior studies, a maximum positive and negative UV of 4 mm was selected. Initially, the plate was fixated based on the specimen’s baseline UV which was normalized to an UV of 0 mm.
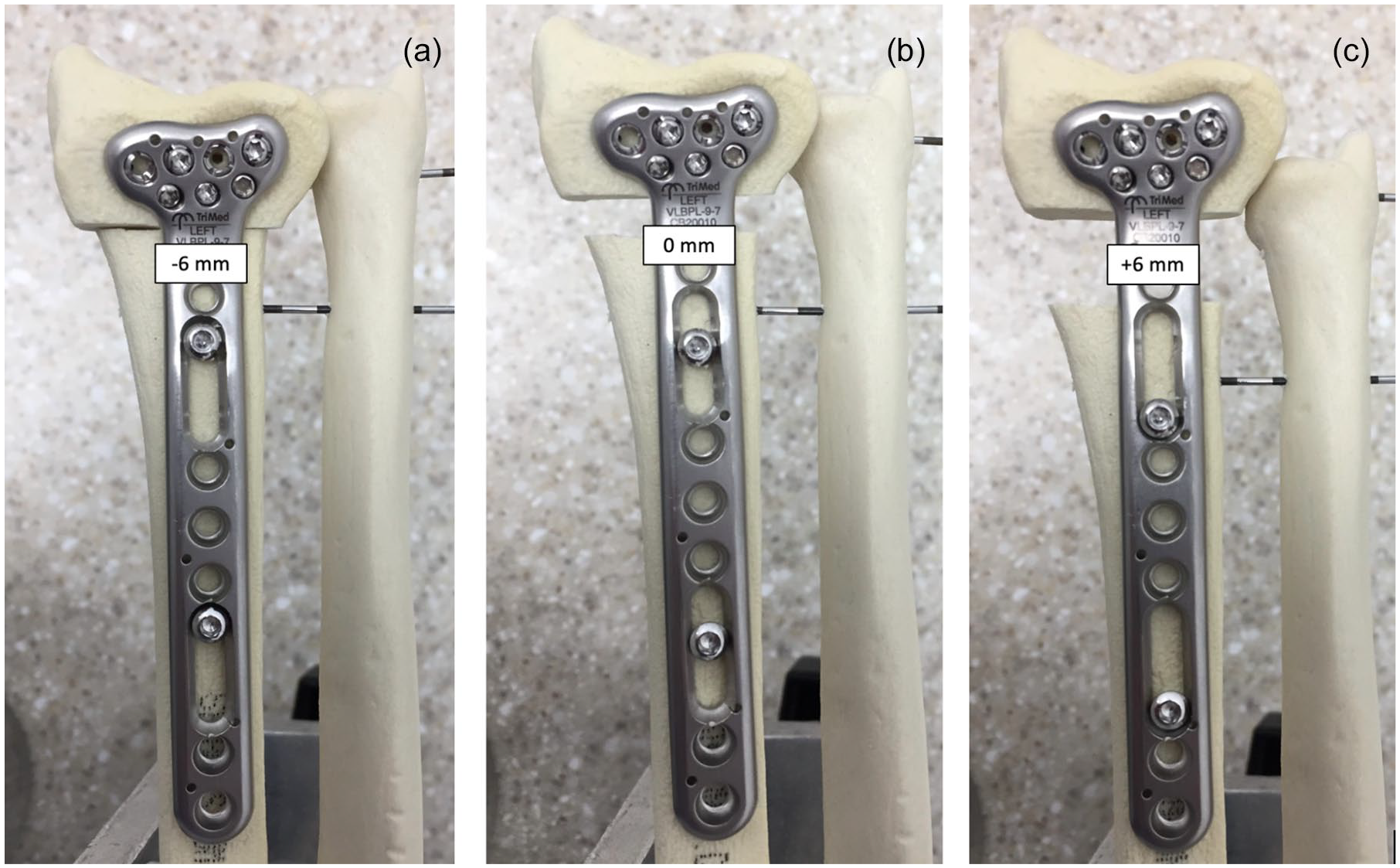
Custom-made radial osteotomy plates used to ensure consistency in ulnar variance between specimens.
The specimen was then secured to the testing table in a neutral position with the elbow at 90° of flexion. Since only the translational motion of the radius relative to the ulna was evaluated, 3 pins in varying directions were inserted into the ulna at approximately the one-third and two-third distances from the elbow. 20 These pins were then stabilized using an external fixator system, which was secured directly onto the testing table.
Radial motion was evaluated using 1 Intel real sense cameras (Intel Corporation, Santa Clara, California) (Supplement A). To measure a change in translation, a purple and green colored ball, each on a Kirschner wire, were inserted into the specimen (Figure 2). The first ball was inserted on the ulnar aspect of the ulna, and the second ball was fixated to the volar aspect of the radial shaft. A pin was then inserted perpendicularly to the dorsal aspect of the radius, within approximately 3 cm from the proximal osteotomy site. To mimic a Shuck test, for each round of testing a perpendicular force was applied by 1 author (WH), who was blinded to the status of the osteotomy, along the dorsal aspect of the radius in a volar direction via the inserted pin with the hand in neutral positioning. The perpendicular pin inhibited any rotational movement by the radius around the ulna. In addition, during the rounds of testing, the ball attached to the radius was visually tracked to ensure no rotation occurred. To ensure a neutral position was maintained, the hand was manually held during testing to inhibit pronation and supination. Radial translation distances were then analyzed using a custom developed Python-coded program (Python Software Foundation, Wilmington, Delaware), which calculated the 3D distance between the centroid of each of the 2 balls at the beginning and end of the simulated shuck test. A white sheet was placed around the specimen to minimize noise interference.
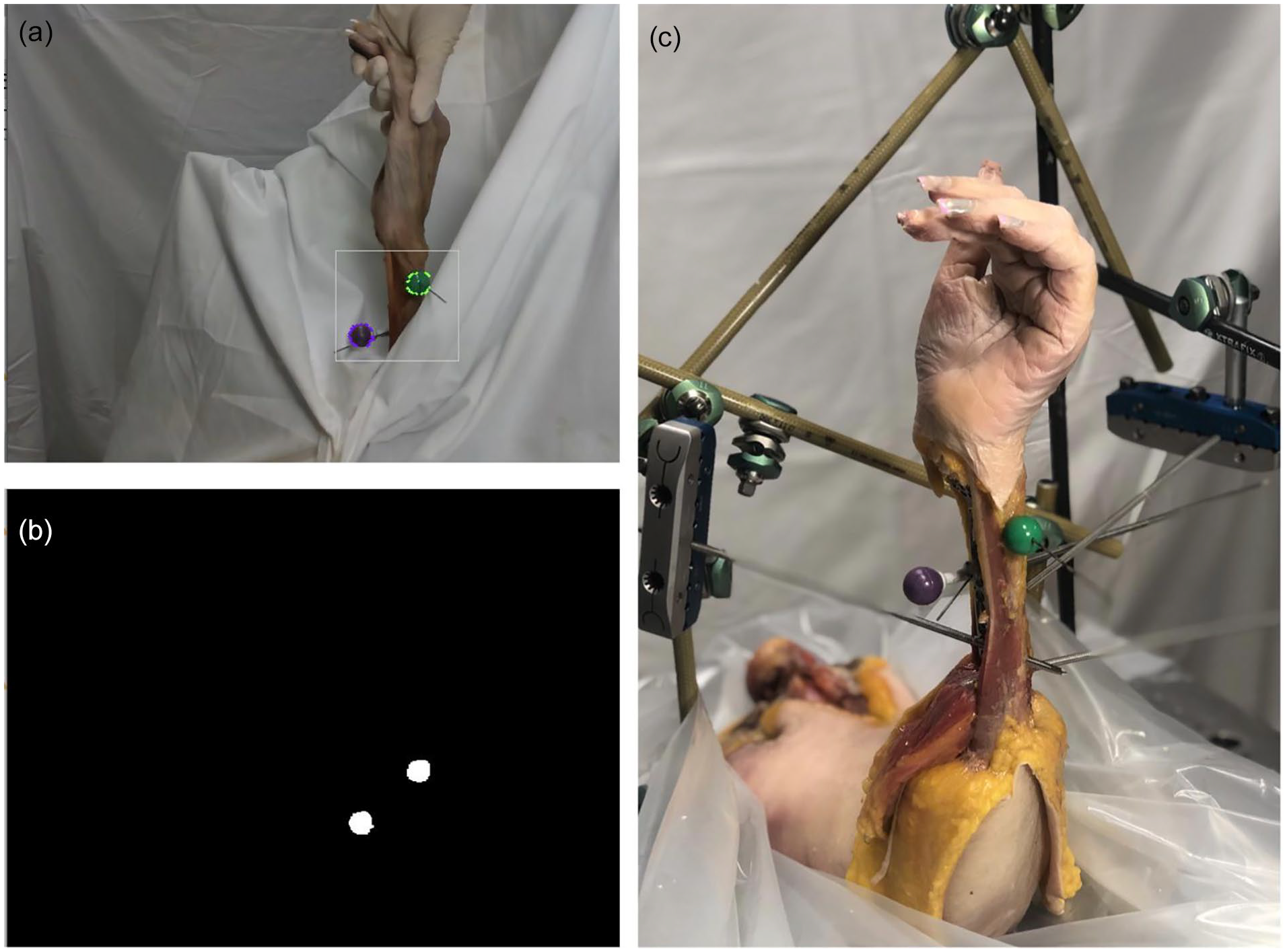
Experimental set-up.
Experimental Testing
Translation testing was conducted at each tested UV state with 3 trials performed per state. Initially, all specimens were tested with the DRUJ intact at the normalized 0 mm UV. The specimens were then tested at + 4 mm or −4 mm UV relative to their natural wrist, the order of which was randomized and changed using the custom-made radial osteotomy plate. A metal block was inserted into the osteotomy site as needed to maintain a rigid radial construct.
After testing was performed in the DRUJ intact state, the DRUJ was sectioned with a scalpel through the TFCC and volar radioulnar ligament to mimic DRUJ disruption after a DRF. The dorsal radioulnar ligament and interosseous membrane were left intact. Testing was then again performed at the normalized UV of 0 mm, + 4, and −4 mm UV, the order of which was again randomized. Three trials were again acquired at each testing state and analyzed using a custom Python program.
Statistical Analysis
Statistical analysis was conducted using RStudio software (v 1.2.1335, R Foundation for Statistical Computing, Vienna, Austria) and STATA (v 13, STATAcorp, College Station, Texas). Data normality was assessed with the Shapiro-Wilk test. The data were found to be non-normally distributed (P < .05). Therefore, the data are presented as median (interquartile range [IQR]) throughout. A Friedman test was used to compare the differences in translation between the 3 UVs tested (+4 mm, 0 mm, −4 mm) with the DRUJ intact and after sectioning. To compare changes from intact to sectioning at each UV, a Wilcoxon signed-rank test was used. Significance was set at P < .05.
Results
A total of 10 cadaveric specimens were included in this study (mean age: 76.00 ± 13.37 years, 5 M/5 F, 10 Left/0 Right). One specimen was utilized for pilot testing. With the DRUJ intact, the pilot specimen demonstrated 1.3 mm and 1.2 mm of translation at + 7 mm and −5 mm UV, respectively. After DRUJ sectioning, the translation at the + 4 mm ulnar positive state was 5.5 mm, while at −5 mm UV only 1.5 mm of translation was observed (Figure 3, Videos 1 and 2). Given these findings, we proceeded with testing the subsequent 9 specimens at neutral (0 mm), ulnar positive (+4 mm), and ulnar negative (−4 mm) with the DRUJ intact and then sectioned. Each specimen was initially adjusted based on their baseline UV, such that each specimen would truly be at 0 mm UV for the neutral state (Table 1).
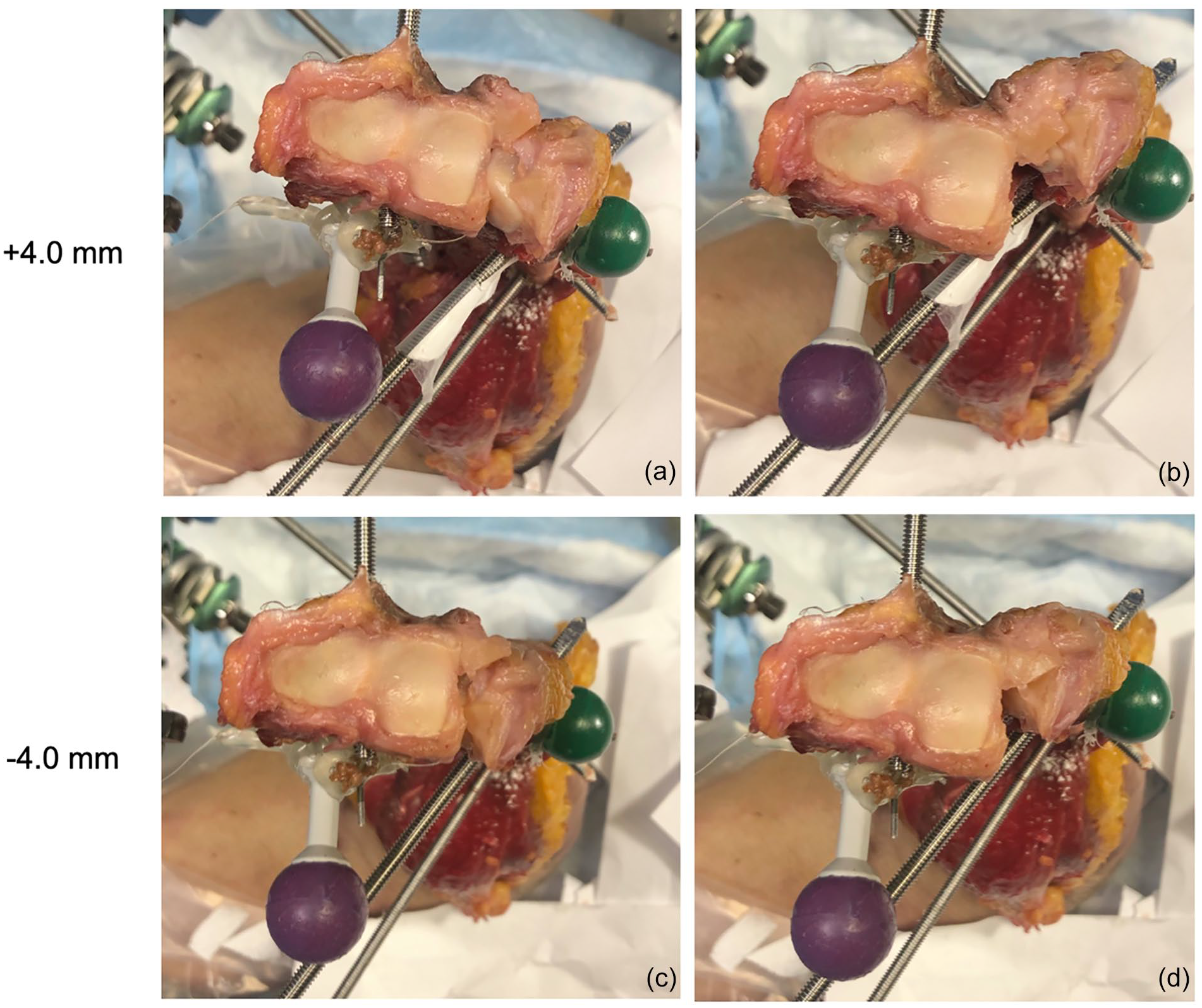
Image stills from videos taken during testing after the DRUJ was sectioned.
Baseline UVs Based Radiographic Measurements and Subsequent UV Adjustments.
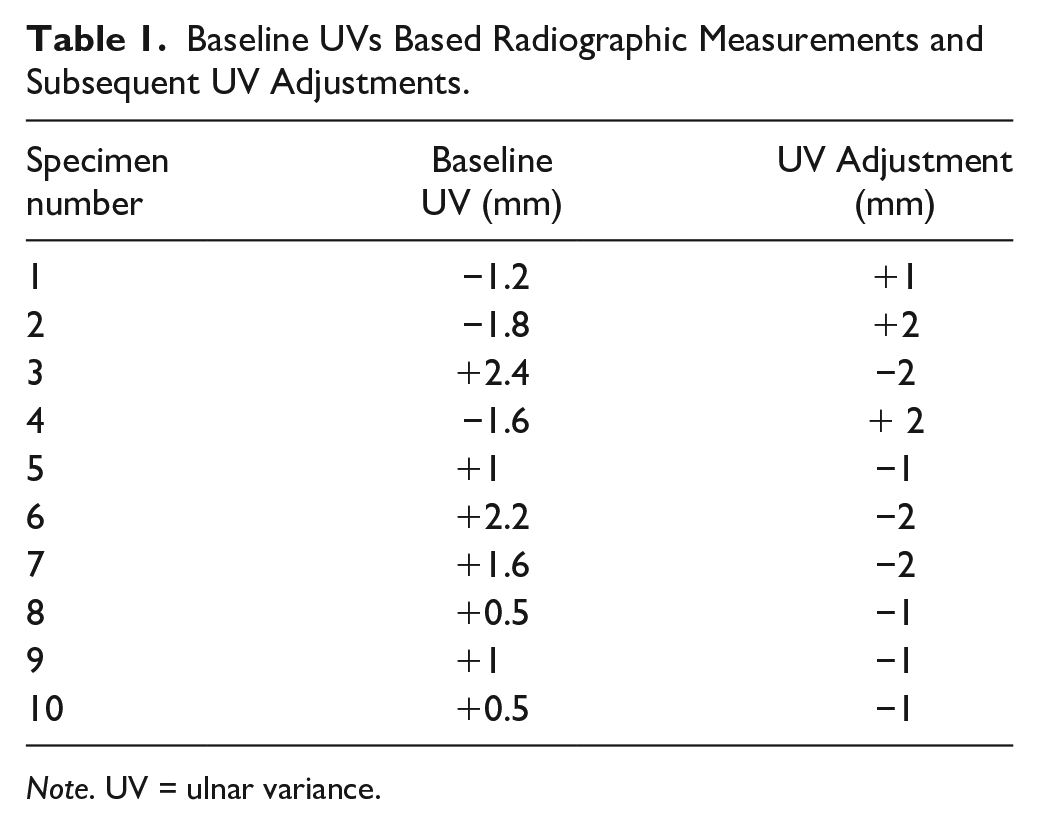
Note. UV = ulnar variance.
Distal radioulnar joint sectioning significantly increased radial translation at neutral (P = .008), at + 4 mm UV (P = .008), and at −4 mm UV (P = .018). Subsequent group comparisons demonstrated no significant difference in translation between the 3 UV groups with the DRUJ intact (P = .124) (Table 2, Figure 4). In contrast, a significant difference in translation was observed between UV groups after DRUJ sectioning (P = .001). Post hoc comparisons demonstrated no significant difference between the positive (+4 mm) and neutral (0 mm) UV states (P = .466). The ulnar negative (−4 mm) state had significantly lower radial translation compared to the positive (+4 mm) (P < .001) variance and the neutral (0 mm) (P = .026) variance states.
Median Translation Before and After DRUJ Sectioning.
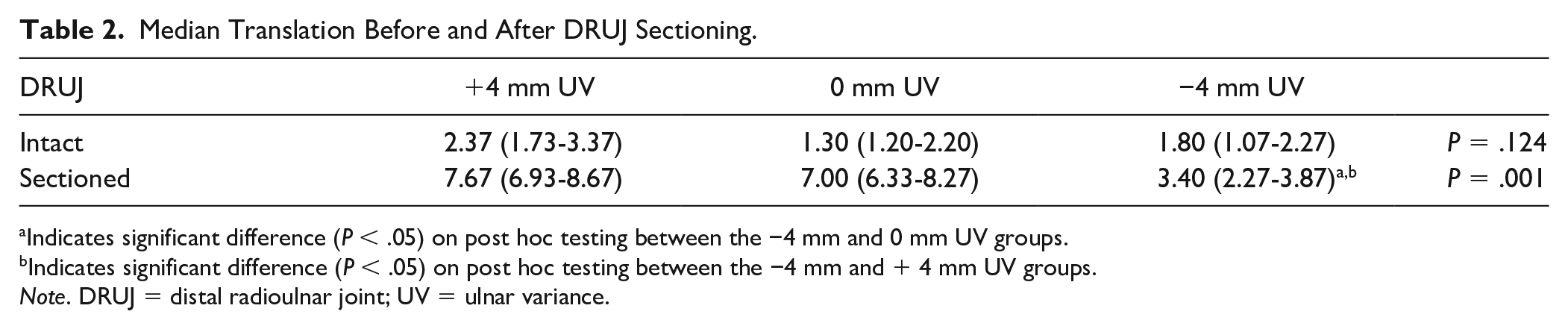
Indicates significant difference (P < .05) on post hoc testing between the −4 mm and 0 mm UV groups.
Indicates significant difference (P < .05) on post hoc testing between the −4 mm and + 4 mm UV groups.
Note. DRUJ = distal radioulnar joint; UV = ulnar variance.
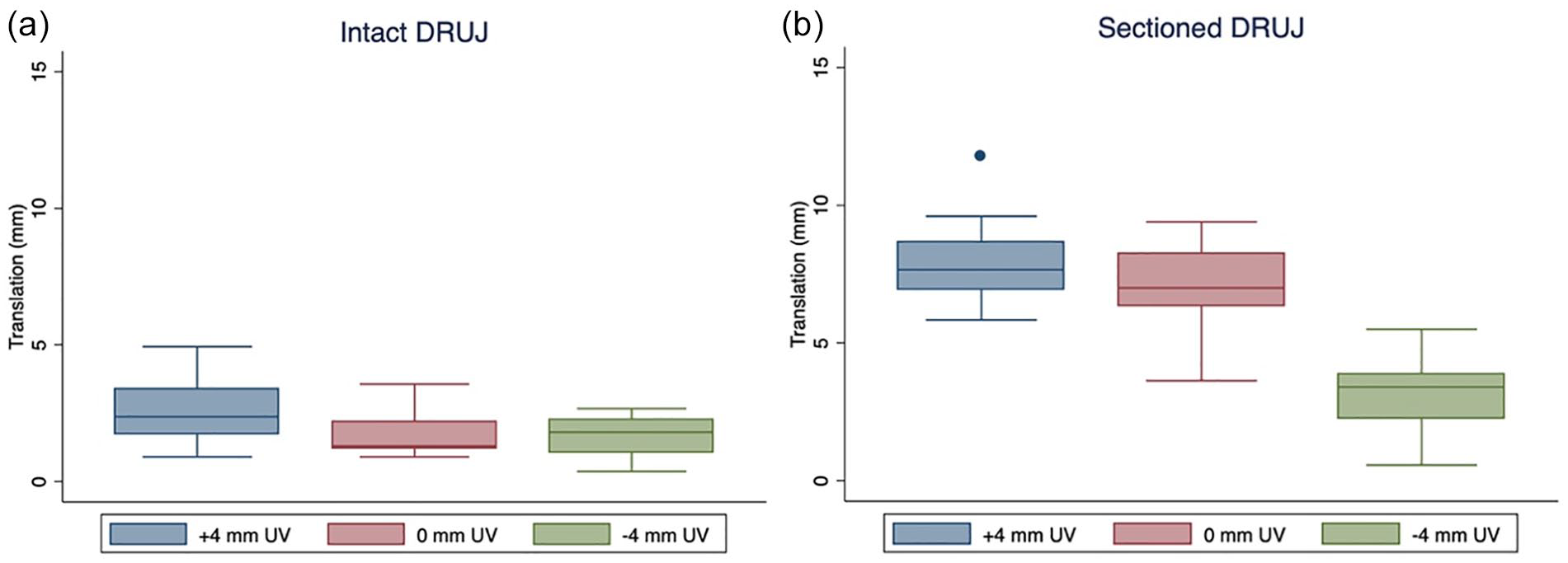
Translation at + 4 mm, 0 mm, and −4 mm (a) UV before and (b) after sectioning the DRUJ.
Discussion
The main finding of this study was that ulnar negativity significantly decreased radial translation after DRUJ sectioning as evaluated with a simulated Shuck test. However, there was no protective effect of ulnar negativity on stability with an intact DRUJ and no difference in radial translation between the 3 UV states. This finding suggests that clinically there may be little consequence of setting a DRF in a neutral, slightly positive, or slightly negative UV on DRUJ stability when the RUL and TFCC are intact. In this setting, UV may mainly affect load distributions across the radius and ulna. When the volar radioulnar ligament is disrupted, whether acutely treating the radius or performing a radial osteotomy in a malunion, inducing ulnar negativity results in decreased radial translation, improving stability of the DRUJ. This approach could target and prevent instability during the index DRF ORIF and decrease the need for subsequent morbidity and procedures related to postoperative DRUJ instability. Our results suggest that not only does inducing ulnar negativity improve DRUJ stability compared to significant ulnar positivity but also compared to neutral UV.
In our study, dorsal radioulnar ligaments were not sectioned since Omokawa and Baek’s studies demonstrated that the type of instability present in DRFs was volar translation of the radius relative to the ulna.21,22 This type of instability was replicated in our scenario. Additionally, the dorsal radioulnar ligament does not tear in DRF, it results in an avulsion injury of the dorsal ulnar corner of the sigmoid notch. This is a reliable and predicable fracture fragment as described in the Medoff classification. 23 Accurate fixation of this fracture fragment will restore dorsal radioulnar ligament stability. However, as our study notates, this may not be adequate for DRUJ stability.
To our knowledge, no prior study has directly investigated the role of negative UV via radial osteotomy on DRUJ instability in the setting of volar RU ligament disruption. One prior biomechanical study by Nishiwaki et al, however, investigated the effect of ulnar shortening on DRUJ stiffness. 24 In contrast to our study, the authors reported that shortening the ulna by 6 mm resulted in a 44% increase in DRUJ stiffness with the arm in a neutral position with an intact DRUJ. Similar to our study, the authors noted an increase in stiffness after sectioning the dorsal, palmar, or complete RUL in the ulnar osteotomy group compared to the control group; however, the ulnar osteotomy failed to restore native stiffness. Negative UV can be achieved either through an ulnar shortening osteotomy or radial lengthening osteotomy. In this study, we decided to evaluate UV by changing the length of the radius, not the ulna, as we believed this would be the most clinically relevant approach when performing a DRF ORIF, but improved DRUJ stiffness through either approach likely occurs through similar mechanisms.
An additional study by Trehan et al investigated DRUJ stability through radial translation after radius shortening osteotomy at 2 locations along the radius (proximal and distal) prior to and after mimicking TFCC detachment through an ulnar styloid detachment. 25 Similar to our data that demonstrated no significant difference between ulnar positive and ulnar neutral states on DRUJ stabilities, Trehan et al, reported no differences between the control and 2- and 4-mm osteotomies in any position (neutral, pronation, and supination). Furthermore, no significant difference in the ulnar styloid detachment scenario was observed. This together with our study suggests that neutral and positive UV likely do not significantly affect DRUJ stability regardless of the status of the TFCC. It is important to note that in our study, only the dorsal to volar direction was examined.
Prior studies on ulnar shortening osteotomies have suggested that this procedure can result in increased DRUJ stability through increasing tension on surrounding structures such as the TFCC. 24 However, the TFCC and RUL were completely transected in this study to generate maximum DRUJ instability. In our testing setting, we hypothesize that increasing ulnar negativity increased tension on the distal oblique bundle (DOB) by increasing the distance between the ulnar and radial DOB insertions. Dy et al, for example, demonstrated that 4 mm coronal displacement of the distal DRF fragment in the presence of an ulnar styloid fracture did not significantly change DRUJ stability compared to the control state, which may be due to increased tension on the DOB. 26 However, prior studies have demonstrated that DOBs are not present in all specimens. 27 , 28 Theoretically, in vivo ulnar negativity would not only increase tension on the DOB but also increase tension on the TFCC as described by Bessho et al., generating greater stability. 14
Limitations
This study should be evaluated within the context of a few limitations. First, this was a biomechanical study and therefore may not directly reflect the in vivo dynamics of the radius. For example, because the hand was removed when testing the DRUJ sectioned state, no load was applied to the forearm muscles, which could have some mild effects on radial translation. Our study also only evaluated 3 states of UV; an ulnar positivity of +4 mm would not be recommended clinically as current dogma teaches that UV should be < 2 mm. However, our findings in the sectioned group were not only significant compared to + 4 mm UV but also compared to 0 mm UV, demonstrating the clinical relevance of our study. The UV threshold at which stability improves and the correlation between degree of negative UV and stability were out of the scope of this study. An additional limitation was that our trials were all performed with the forearm in a neutral position; pronation or supination were not assessed, and this could affect stability due to increased tensioning of the DOB and we did not perform post-testing anatomic studies to confirm the presence of the DOB. In addition, we only tested instability in 1 direction (volar), other directions of movement such as dorsal translation and rotation were not investigated. In addition, the effects on translation of further sectioning of the dorsal radioulnar ligament were not assessed. Furthermore, it is possible that our custom developed 3D acquisition program introduced small amounts of error to the radial translation measurements. This limitation was addressed by averaging 3 trials for each state and UV. It is also important to acknowledge that different shapes of the sigmoid notch may play a role in DRUJ stability. Lastly, there could be minor differences between the locations of the balls that were manually placed, and these differences could alter the measured radial translation.
Conclusion
Fixating the radius in −4 mm of ulnar negativity significantly decreased radial translation after sectioning the volar radioulnar ligament and foveal attachment of the TFCC. Ulnar variance had no effect on stability with an intact DRUJ. A radial osteotomy to decrease ulnar variance may improve DRUJ stability in the setting of volar radioulnar ligament and TFCC injury due to a DRF.
Supplemental Material
sj-docx-1-han-10.1177_15589447221124233 – Supplemental material for Negative Ulnar Variance Lessens DRUJ Instability After DRUJ Disruption: A Biomechanical Analysis
Supplemental material, sj-docx-1-han-10.1177_15589447221124233 for Negative Ulnar Variance Lessens DRUJ Instability After DRUJ Disruption: A Biomechanical Analysis by Hailey P. Huddleston, Joey S. Kurtzman, Liam Deegan, Westley Hayes, Kevin Austin, John Carter, William R. Aibinder and Steven M. Koehler in HAND
Footnotes
Authors’ Note
Study performed at SUNY Downstate Medical Center, Brooklyn, NY.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was no obtained because this study does not contain any human subjects.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.K. has received past speaker honorarium from TriMed, Inc. S.K. is a committee member of the American Society for Surgery of the Hand (ASSH), a paid consultant and speaker for Integra LifeSciences, Inc, a paid consultant for Tissium, Inc., a stockholder and member of the medical advisory board for Reactiv, Inc., and a speaker for TriMed, Inc. W.R.A. is a consultant for Exactech. All other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hardware donated in-kind from TriMed, Inc. No funding was received for this study.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.