
Abstract
Background:
The use of ultrasound in the diagnosis of cubital tunnel syndrome (CuTS) is an attractive alternative to electrodiagnostic (EDX) studies, but its utility is binary with poor severity correlation. We hypothesize that increasing ulnar nerve cross-sectional area (CSA) and power Doppler measurement of intraneural vascularity may predict the extent of disease.
Methods:
We identified 20 elbows from patients with a history of CuTS and 20 elbows in 10 asymptomatic controls. Electrodiagnosis was performed for symptomatic patients. Gray-scale ultrasound and power Doppler ultrasound were performed to measure CSA and intraneural vascularity in all participants. Functional measures, Boston Carpal Tunnel Questionnaire (BCTQ), and Patient-Reported Outcomes Measurement Information System surveys were also completed.
Results:
A strong positive correlation was found between CSA and motor nerve conduction velocity (MNCV) decrease between elbow and forearm, which increased when BCTQ >2 was used as a screening criterion. Increased CSA also demonstrated a high positive predictive value (PPV) in predicting MNCV changes, but poor ability to predict axonal loss. In contrast, power Doppler ultrasound demonstrated 100% PPV and 94% negative predictive value (NPV) in predicting severe CuTS (defined as compound motor action potential [CMAP] amplitude <6 mV and electromyography [EMG] findings).
Conclusions:
Cross-sectional area is a sensitive method for identifying changes in MNCV and amplitude but does not stratify disease severity, as defined by diminished CMAP amplitude and/or evidence of denervation on EMG. The presence of increased intraneural vascularity is relatively sensitive but highly specific for axonal loss. The combination of nerve CSA, BCTQ screening, and power Doppler ultrasound may provide an alternative means for CuTS assessment.
Keywords
Introduction
Cubital tunnel syndrome (CuTS) is the second most commonly diagnosed peripheral nerve compression in the general population. Its annual incidence has been estimated to be 24.7 per 100 000 person-years. 1 However, a cross-sectional study using active surveillance demonstrated a much higher rate of symptomatic CuTS, with a prevalence of 1.8% to 5.9%. 2 Treatment can be effective for early-stage disease, with some patients having complete resolution of symptoms, 3 but late diagnosis leads to irreversible muscle atrophy and hand dysfunction.
Often relied on as the criterion standard in nerve pathology diagnosis, electrodiagnostic (EDX) testing may be normal in early CuTS, particularly when symptoms are from dynamic ischemia. 4 Ultrasound is a promising method to diagnose ulnar nerve compression neuropathy through evaluation of changes in fascicular morphology. Normal sonographic parameters of the ulnar nerve at the elbow have been established in a large clinical trial of asymptomatic patients. 5 Similarly, increased cross-sectional area (CSA) of the ulnar nerve at the cubital tunnel (>10 mm2) has been correlated with clinical symptoms, even in the presence of normal nerve conduction, 6 leading many to recommend the use of ultrasound in CuTS diagnosis.7,8 However, morphologic changes in nerve size have not been well correlated to symptom severity. 9 Therefore, although increased CSA may represent a marker of neuropathy, it is relatively poor at predicting the extent of disease or recovery potential. Given that compressive neuropathies result in chronic hypoxia to the nerve, a compensatory increase in vascularity is a potential indicator of compression and may stratify severity.
Elevated intraneural vascularity can be visualized with color Doppler flow, which uses the Doppler effect to identify the velocity of blood flow. Blood moving at higher velocity is more readily apparent, but slower moving blood may be difficult to detect. 10 Alternatively, power Doppler represents overall signal strength without regard to direction, allowing for more sensitive detection at lower velocity 11 and improved identification of vasculature over color Doppler. 12
The use of ultrasound to aid in CuTS diagnosis is an attractive alternative to EDX, but data on its correlation with disease severity are lacking. Thus, the goal of this study was to identify intraneural vascular changes on power Doppler in symptomatic patients and evaluate the relationship between EDX findings of ulnar nerve compression and changes on ultrasound. We hypothesized that increased CSA and intraneural vascularity, as detected using power Doppler ultrasound, would provide accurate indicators of clinically significant disease.
Materials and Methods
A matched cohort study was performed of adult patients, presenting to the clinics of the senior authors, with clinical symptoms consistent with CuTS and healthy, asymptomatic volunteers. Through this enrollment, we identified a symptomatic cohort of 20 elbows from 20 patients with CuTS, which were matched by age and sex to a cohort of 20 asymptomatic elbows from 10 healthy volunteers.
Clinical Evaluation
The study protocol was reviewed and approved by our institutional review board (IRB). Potential participants were screened when they presented to the private clinics of the participating surgeons. To qualify, patients needed a clinical examination and history consistent with CuTS as defined by the treating physician. Patients with a known diagnosis of cervical radiculopathy, prior elbow surgery, diabetic peripheral neuropathy, or brachial plexus injury were excluded, as were patients unable to give informed consent. Physical examination by the treating surgeon included standardized provocative tests for CuTS (elbow flexion compression test, Tinel sign), plus assessment of 2-point discrimination and Patient-Reported Outcomes Measurement Information System (PROMIS) surveys (including Anxiety, Depression, Pain Interference, and Physical Function domains). If determined eligible, symptomatic patients were either enrolled in clinic by the surgeon or were flagged to be consented over the phone by the research coordinator. Written informed consent was completed at the time of enrollment.
EDX and Ultrasound Assessment
Following enrollment, patients underwent EDX and ultrasound evaluation of the ulnar nerve in the symptomatic extremity. These tests were performed by a physiatrist board-certified in EDX medicine and neuromuscular ultrasound (American Board of Electrodiagnostic Medicine), who was unblinded to the potential diagnosis. Only patients who completed testing at our institution were included to minimize variability in EDX and sonographic technique. Electrodiagnosis was performed in accordance with the American Association of Neuromuscular & Electrodiagnostic Medicine standards using a Cadwell Sierra Summit (Kennewick, Washington) electromyography (EMG) machine. Ulnar motor nerve conduction studies to the abductor digiti minimi (ADM) (8 cm) and first dorsal interosseous, and antidromic ulnar sensory nerve conduction study to the small finger (14 cm) were performed. As reduction of compound motor action potential (CMAP) amplitudes below 6 mV has been correlated with disease severity and prognosis for recovery in CuTS, 13 we defined severe cubital tunnel as CMAP amplitudes below 6 mV and/or evidence of denervation changes on EMG.
Symptomatic patients were bilaterally scanned with a Sonosite X-Porte (Bothell, Washington) ultrasound machine from the mid-arm to the mid-forearm with the elbow in 70° to 90° of flexion (based on clinical measurement). The CSA of the ulnar nerve across the elbow was recorded, using gray-scale ultrasound, at 4 different locations (the epicondylar groove, 7 cm proximal to the medial epicondyle, 3 cm distal to the medial epicondyle, and the wrist) with the free-hand trace function of the machine (Figure 1). Imaging locations were determined using a tape measure. The CSA measurements correlate to the below-elbow and above-elbow stimulations for the ulnar motor nerve conduction studies, which routinely use a tape measure for accurate distances. Abnormal CSA was defined as >10 mm2. Power Doppler ultrasound was performed bilaterally on short and long axis to detect increases in intraneural vascularity (Figure 2). Vascularity was observed to be either present or absent within the nerve, based on the assessment of the power Doppler images, and thus recorded as a binary variable. Ultrasound imaging was conducted bilaterally so that contralateral elbows could be used for comparison with the symptomatic elbow. If bilateral symptoms were present, the ulnar nerve from the side with greater patient-reported symptom severity was deemed symptomatic for analytical purposes.
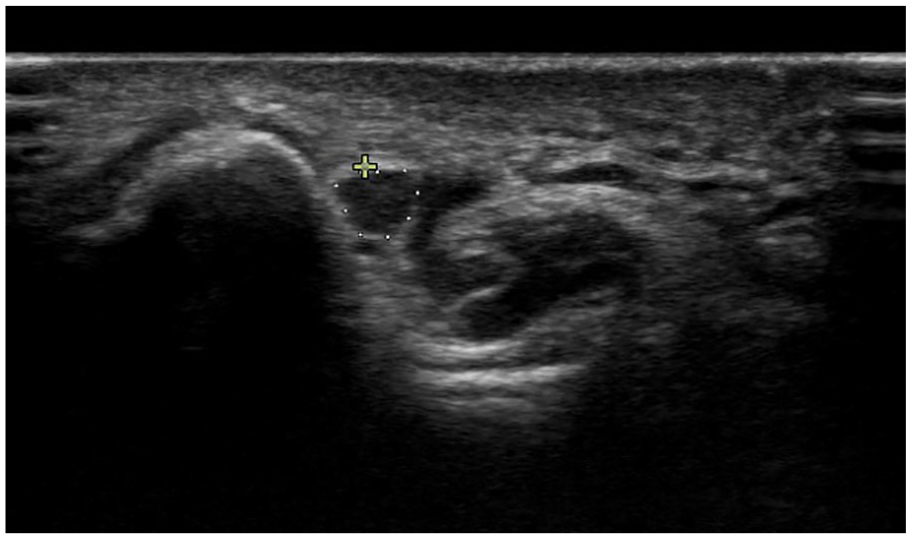
Measurement of cross-sectional area of the ulnar nerve at the level of the medial epicondyle in a control patient.
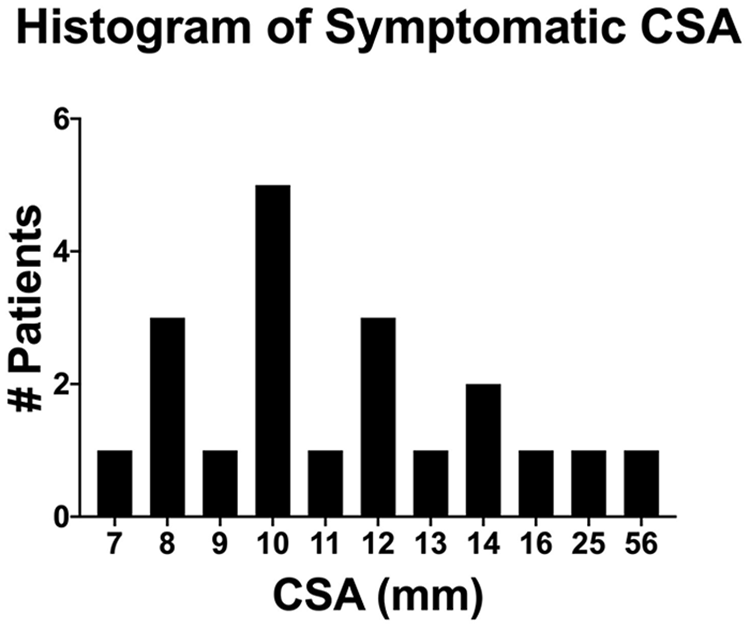
Histogram of CSA in symptomatic patients.
Functional Outcomes
Functional assessment occurred either at the follow-up visit with the treating surgeon or at a separate hand therapy appointment. Impairment measures included: grip and key pinch strength, and Semmes-Weinstein monofilament (SWM) testing. Grip strength was measured with a Jamar hydraulic hand dynamometer; pinch strength was measured with a pinch gauge. An SWM score was calculated by averaging the values recorded across the ulnar aspect of the palm, ulnar aspect of the fourth digit, and entire fifth digit of the hand on the patient’s symptomatic side. Patients also completed the Boston Carpal Tunnel Questionnaire (BCTQ) and PROMIS surveys for anxiety, depression, pain interference, and physical function. The BCTQ was used as a proxy for patient-reported symptom severity to correlate with EDX findings as prior studies have demonstrated validity of this instrument in diagnosing cubital tunnel 2 and assessing postoperative recovery. 14 All tests were completed by either the treating physician or a dedicated occupational therapist to minimize interobserver variability.
Asymptomatic Cohort
Healthy volunteers were enrolled for the control cohort using the services of the study participant registry at our institution. Interested participants were contacted and screened over the phone by the research coordinator using an IRB-approved phone script. To be deemed eligible, participants needed to score <2 on the BCTQ Symptom Severity (BCTQSS) scale, which suggested no underlying upper extremity neuropathy and no history of prior elbow surgery or injury. Following verbal consent, participants were scheduled for ultrasound imaging with the physiatrist. The written informed consent form was completed at the start of the study visit. Control participants were only assessed using ultrasound imaging (both gray scale and Doppler modalities) and not subjected to invasive EDX. Control subjects completed PROMIS surveys and were compensated for their time with gift cards.
Statistical Analysis
Primary outcome measures were the ulnar nerve CSA measurements at the level of the medial epicondyle, the presence of intraneural vascularity on power Doppler, and change in motor conduction velocity of at least 10 m/s across the cubital tunnel. The Fisher exact test was used to perform contingency analysis of the predictive value of BCTQSS regarding EDX, as well as the predictive value of CSA and the presence of power Doppler signal in identifying abnormal thresholds in EDX. Correlations between CSA and change in ulnar motor conduction velocity between elbow and forearm segments, as well as sensory amplitudes were calculated. The Shapiro-Wilk test was used to assess normality, and the Spearman rank test was used for nonparametric assessment. Unpaired 2-tailed t tests were used to compare patient questionnaires across the cohorts, with significance value set at P < .05. Descriptive statistics were calculated for pinch and grip strength as well as SWM in the symptomatic cohort.
Based on data examining power Doppler and CSA in carpal tunnel syndrome, 15 a large difference in vascularity between patients and controls (effect size = 2.0) and a moderate correlation between vascularity and nerve conduction velocity are expected. We conservatively assumed we would observe an effect size of 0.75 and with a sample size of 10 per group would achieve 87.1% power to detect this difference, assuming a 2-sided test at a significance level of .05. Given this sample size, we have 80% power to detect a correlation of 0.76 or higher, assuming a 2-sided test and an α level of 0.05.
Results
A total of 20 patients and 20 elbows were enrolled in the symptomatic group, with a female:male (F:M) ratio of 8:12. Ten asymptomatic patients and 20 elbows were enrolled in the control group with an F:M ratio of 6:4. The average age of the symptomatic patients was 52.1 years, and the average age of the volunteer controls was 50.4 years.
The PROMIS outcome data, as well as SWM testing and grip and pinch strength were not obtained from 4 patients in the symptomatic group due to lack of patient follow-up. The BCTQ data were not obtained in 3 of the same 4 patients. One additional patient was missing grip and pinch strength.
Patient-Reported and Functional Outcomes
No significant difference was found between groups in assessment of Anxiety or Depression PROMIS scores. Pain interference score was significantly higher in the symptomatic group (P < .05, mean difference, 15.6; 95% confidence interval [CI] = 8.6-22.6), whereas Physical Function score was significantly lower in the symptomatic group (P < .05, mean difference, −10.4; 95% CI = −18.6 to −2.2). The BCTQSS score was significantly different between the groups, with an average score of 1.06 in the control group and an average score of 2.7 in the symptomatic group (P < .05, mean difference, 1.6; 95% CI = 0.87-2.4). Boston Carpal Tunnel Questionnaire Symptom Severity scores >2 were found in 11 of the 17 patients with completed questionnaires in the symptomatic group. However, the positive predictive value (PPV) in BCTQSS >2 identifying decreased motor conduction velocity across the elbow was 0.45 (P = .67, 95% CI = 0.22-0.72), and the negative predictive value (NPV) was 0.67 (95% CI = 0.35-0.88). The mean value of SWM testing was 3.66 for symptomatic patients, the average grip strength as percentage of the contralateral side was 83% ± 28%, and the average pinch strength of the contralateral side was 77% ± 26%.
CSA and Intraneural Vascularity
Out of the 4 ultrasound locations, the CSA of the ulnar nerve at the epicondylar groove was observed to be the greatest for all symptomatic patients and chosen for analysis. The average ulnar nerve CSA at the elbow in the asymptomatic cohort was 9.65 ± 3.1 mm2. In the asymptomatic control patients, the CSA of the ulnar nerve was >10 mm2 in 4 of the 20 elbows. Out of the 4 control subjects with ulnar CSA >10 mm2, the nerve was noted to dislocate anterior to the medial epicondyle with end-range elbow flexion in 3 of these patients and perch on the medial humeral epicondyle for the fourth patient. No CSA >10 mm2 was noted in any nerve that did not dislocate, and dislocation was not found in any nerve with a normal CSA.
The average CSA in the symptomatic cohort for symptomatic elbows was 13.75 ± 10.7 mm2, and a histogram of the CSA across the symptomatic patients is seen in Figure 2; 10 of the 20 patients had CSA >10 mm2. The average CSA for the contralateral elbow in the symptomatic patients was 9.95 ± 2.6 mm2. Two patients exhibited complete ulnar nerve dislocation, with CSA of 10 and 12 mm2. Five patients were found to have ulnar perching with flexion, 2 of which had a CSA >10 mm2. In symptomatic patients, CSA was negatively correlated with grip strength (reported as percentage of contralateral side) (r = −0.52, P = .04), but CSA did not correlate with pinch (r = −0.29, P = .29). No significant correlation between CSA and BCTQSS score was identified in a combined analysis of control and symptomatic subjects (r = 0.33, P = .052). Secondary analysis with inclusion limited to patients with BCTQSS >2 again demonstrated no significant correlation between CSA and BCTQ (r = −0.03, 95% CI = −0.62 to 0.58). No patients in the control group had evidence of intraneural vascularity on power Doppler examination, whereas 2 of the patients in the symptomatic group had positive intraneural vascularity.
Correlation of Ultrasound Parameters With EDX Parameters
The Shapiro-Wilk test demonstrated that CSA and ulnar ADM velocity were not normally distributed; therefore, Spearman rank order correlation was performed. A strong correlation (r = 0.69, P < .05) was found between CSA and a decrease in motor ADM nerve conduction velocity between the elbow and the forearm (Figure 3). Notably, this increased when BCTQSS >2 was used as a screening criterion (r = 0.88, P < .05). Cross-sectional area was also moderately negatively correlated with ADM motor amplitude (r = −0.52, P < 0.05) and strongly negatively correlated with sensory amplitude (r = −0.75, P < .05) (Figures 4 and 5).
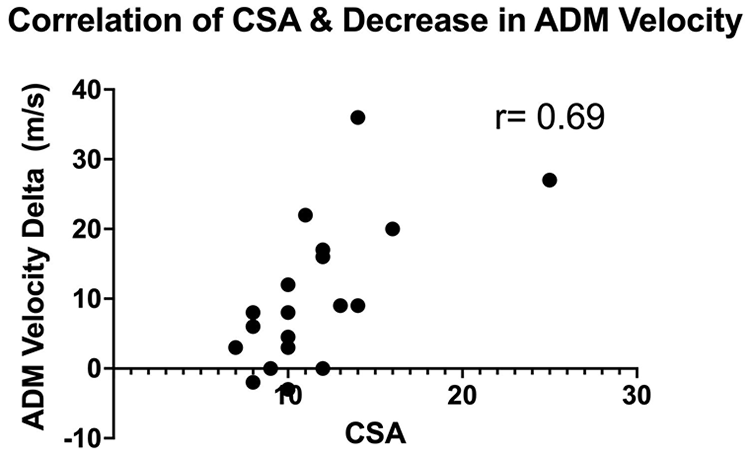
Increasing CSA showed a strong correlation with decrease in motor conduction velocity.
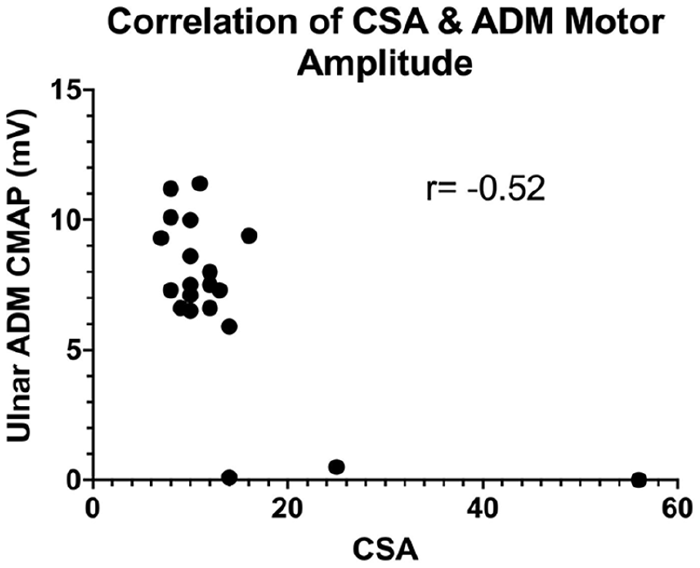
Increasing CSA showed a moderate negative correlation with CMAP amplitude.
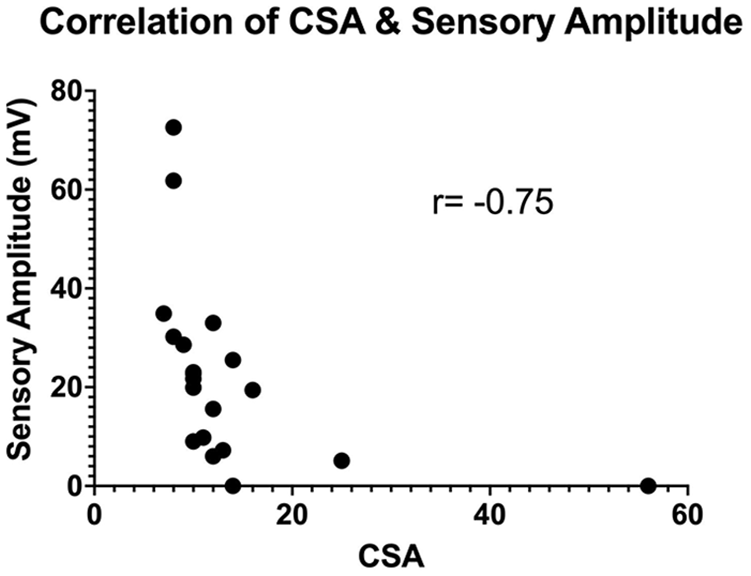
Increasing CSA showed a strong negative correlation with sensory nerve action potential amplitude.
Predictive Value of CSA Enlargement Versus Doppler Ultrasound in Identifying Severe Cubital Tunnel
In patients presenting with clinical symptoms of CuTS, CSA >10 mm2 demonstrated a PPV of 0.70, an NPV of 0.90, a sensitivity of 0.88, and a specificity of 0.75 (P < .05) in identifying an ADM motor conduction velocity difference of at least 10 m/s between the elbow and forearm segments without the need for screening with the BCTQ. Cross-sectional area demonstrated a relatively low PPV (0.30; 95% CI = 0.11-0.60) in identifying severe CuTS, although it showed a high NPV (1.0, 95%CI = 0.72-1.00) with a sensitivity of 1.0 and a specificity of 0.59. In contrast, power Doppler ultrasound demonstrated a PPV of 1.00 (95% CI = 0.17-1.00), a sensitivity of 0.67, an NPV of 0.94 (95% CI = 0.74-0.99), and a specificity of 1.0 (Figure 6) in predicting severe CuTS based on χ2 analysis.
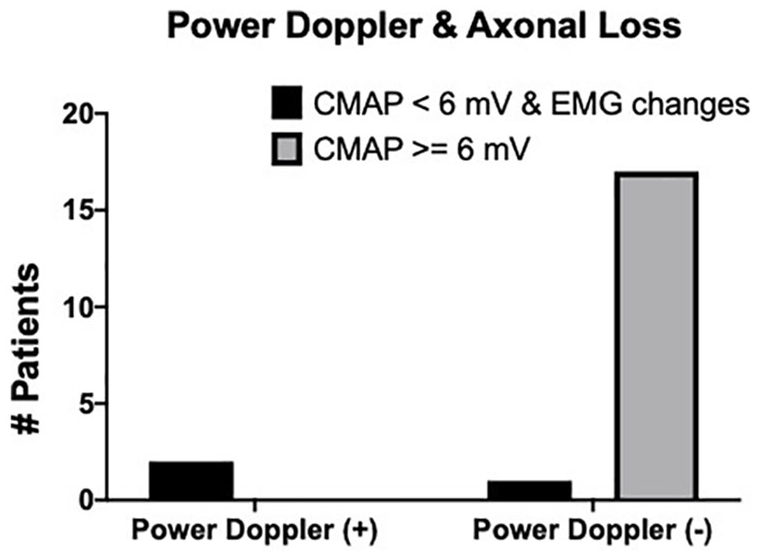
Contingency analysis of the presence of power Doppler signal and evidence of axonal loss. No power Doppler signal was evident in patients with CMAP amplitude ≥6 mV.
Discussion
The presence of increased intraneural vascularity on power Doppler ultrasound greatly improved the positive predictive power of identifying more severe, painful CuTS compared with CSA alone. In the symptomatic group, 2 of the 20 patients demonstrated positive power Doppler findings (Figure 7); both patients displayed severe axonal loss. One of these patients was found to have evidence of a neuroma in continuity proximal to the cubital tunnel from a prior remote injury. Another patient with CMAP amplitude <6 mV and denervation changes on EMG tested negative on power Doppler, despite having a long history of profound ulnar neuropathy. We believe that the lack of intraneural vascularity may be due to the prolonged nature of compression. In carpal tunnel syndrome, reduced intraneural vascularity has been shown to be one of the first variables to improve after surgery, which suggests that it may correlate with chronic inflammation. 16 Interestingly, this same patient (with profound weakness) reported a BCTQSS of 2 and a PROMIS pain interference score of 51.9, which may suggest that the patient had a “cold” nerve 17 that had progressed beyond the painful, inflammatory phase. Therefore, the addition of power Doppler ultrasound may prove useful in diagnosing more advanced disease, potentially overcoming one of the limitations of ultrasound in stratifying CuTS severity in patients with an active inflammatory response or neuritis. However, it may prove less useful in identifying patients with chronically fibrosed nerves. More work is needed to determine whether this inflammatory response correlates with the potential for neurologic recovery.
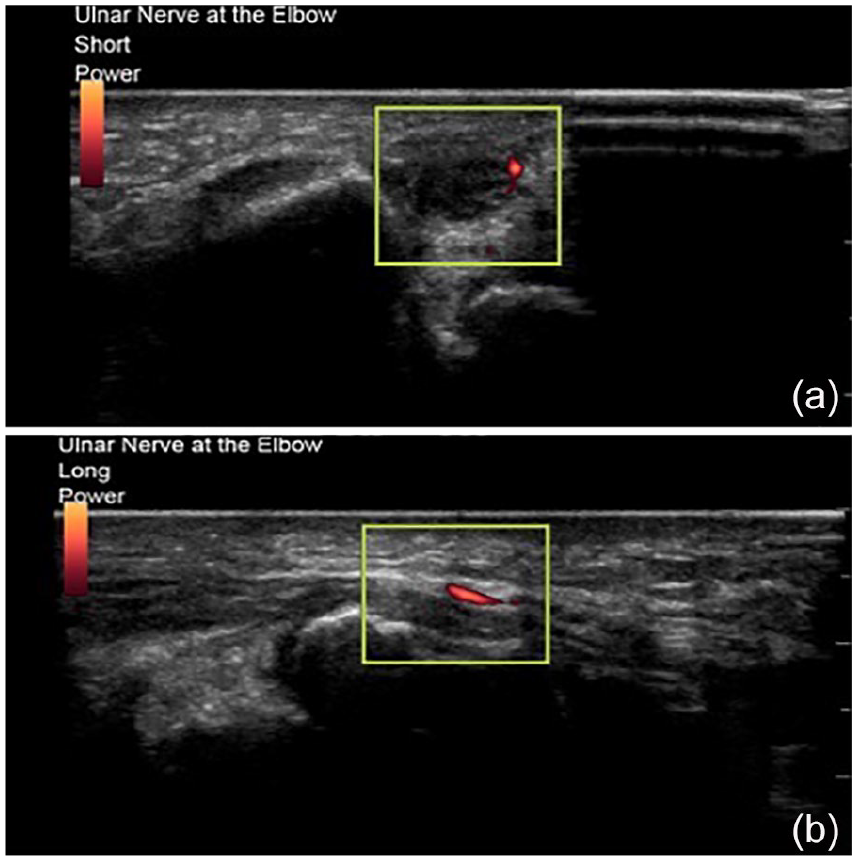
Evidence of power Doppler signal within an enlarged ulnar nerve at the medial epicondyle in both cross sections (a) and along the long axis (b).
Although PROMIS pain, PROMIS physical function, and BCTQSS were significantly different between the groups, BCTQSS did not provide a particularly sensitive method of identifying patients with slowing of their motor nerve conduction velocity. A wide array of outcome measures have been previously used to assess response to treatment of CuTS—a systematic review found 31 postoperative outcome measures in 101 studies. 18 While only reported in 3% of studies, Patient-Related Ulnar Nerve Evaluation (PRUNE) has been shown to have the best validity and responsiveness. 18 Similarly, CSA did not correlate well with BCTQ score in the combined patient cohort or in the symptomatic group alone. This suggests that the CSA of the ulnar nerve taken in isolation does not directly predict symptoms experienced by patients. However, a strong correlation was found between CSA and a decrease in conduction velocity across the elbow, and a negative correlation was found between CSA and sensory and motor amplitudes. Inclusion of PRUNE in future studies would be interesting to assess its potential to enhance the sensitivity of diagnosis of CuTS with ultrasound measurements.
Increased CSA of the ulnar nerve secondary to ulnar nerve instability in asymptomatic patients has been previously reported 19 and was identified in 20% of our asymptomatic subjects, demonstrating its value in identifying potential sources of nerve pathology. However, symptoms of individuals should be considered when interpreting increased CSA. A recent meta-analysis of the literature reviewing the utility of CSA in diagnosis of CuTS estimated a sensitivity of 0.85 and a specificity of 0.91. 9 Cross-sectional area has previously been correlated with slowing of nerve conduction velocity in ulnar neuropathy in a prospective study comparing ultrasound and EDX findings of patients with CuTS. 20 However, although the authors identified a statistically significant negative correlation between CSA and decrease in nerve conduction velocity, the reported correlation coefficients ranged from −0.14 to −0.47, substantially lower than in the present study. Similarly, Bayrak et al 21 reported statistically significant but weak correlations (r = 0.3-0.4) with overall electrophysiological severity. In this study, CSA appeared to correlate more with markers of myelination than axonal health, which corroborates the findings above. Thus, although CSA appears to be sensitive in the diagnosis of CuTS, it may be limited in its ability to discriminate axonal loss.
In contrast, the presence of intraneural vascularity on power Doppler ultrasound was moderately sensitive and highly specific in identifying severe CuTS. Frijlink et al 22 previously evaluated the presence of intraneural vascularization with color Doppler (but not power Doppler) in patients with CuTS and found it to be related to clinical and EDX severity. Ghanei et al 23 found that the presence of intraneural vascularity on color Doppler has a sensitivity of 66% and a specificity of 93% for diagnosis of CuTS and was more likely to be present in patients with severe neuropathy. Cheng et al 24 detected intraneural vascularity using power Doppler in 15% of patients with CuTS and found an association with increasing dysfunction magnitude on EDX. The authors concluded that the addition of power Doppler did not increase the sensitivity of diagnosis compared with gray scale but did help with assessing severity. The presence of intraneural vessels has been shown to have a sensitivity and specificity of 83% and 89% 15 in diagnosing carpal tunnel syndrome, and increases in the pixel area of intraneural vascularity were proportional to the severity of the disease. In a separate study, intraneural vessels were only found in patients with EDX positive for carpal tunnel syndrome. 25
This study is not without limitations, most notably the lack of a criterion standard for diagnosis of CuTS and the relatively small sample size. A much larger study would allow inclusion of a more diverse spectrum of CuTS severity, likely improving the precision of the above correlations. The reliance on EDX as a comparative criterion standard is another source of potential error. Electrodiagnostic sensitivities ranging from 13% to 87% have been reported, although specificity is as high as 95%. 26 If a portion of the nerve is injured from compression, the remaining functional axons may give false negatives on nerve conduction studies (up to 10%). 27 Our study also suffers from incomplete data due to failure of patient follow-up for completion of patient-reported questionnaires in a small subset of the symptomatic group. Finally, an ideal study would also include measurement of EDX in the control group. This poses practical hurdles and ethical considerations given the relative invasive nature of these studies. However, given the tight clustering of BCTQSS scores and lack of any clinical symptoms, this cohort likely represents a reasonable approximation of an asymptomatic group.
Conclusions
In summary, our findings support the use of CSA for diagnosis of CuTS in patients presenting with a compatible history and suggest that power Doppler ultrasound may be useful in identifying patients with severe CuTS and an active inflammatory response of the nerve. Additional research would also help clarify pathophysiologic mechanisms leading to increased CSA and resolution of intraneural vascularity postoperatively. Future studies could also examine the role of ultrasound in identifying asymptomatic patients with evidence of weakness and advanced disease, the so-called “cold nerves.” In symptomatic patients, however, the combination of screening with BCTQ, combined with the measurement of nerve CSA and use of power Doppler ultrasound, may provide a minimally invasive and accurate algorithm for both diagnosis of CuTS and measurement of its severity.
Footnotes
Authors’ Contribution
Dr Brogan, Dr Dy, Dr Colorado, Dr Ray and Mr Lee participated in study design, data collection, data analysis, and manuscript preparation.
Ethical Approval
Consenting and data collection methods were approved by the Washington University in St. Louis Institutional Review Board (protocol number: 201810137).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Department of Orthopaedic Surgery, Washington University in St. Louis.