
Abstract
Background:
Endoscopic and open carpal tunnel releases (ECTR and OCTR) are safe and effective operations. We compared the approaches in terms of postoperative opioid refills and occupational therapy (OT) referrals.
Methods:
We conducted a retrospective study of patients with carpal tunnel syndrome (CTS) treated with ECTR or OCTR. Patients with isolated idiopathic CTS were included; patients undergoing simultaneous bilateral carpal tunnel release (CTR), revision CTR, and additional procedures at time of CTR were excluded. Outcomes included number of patients requiring an opioid refill and/or an OT referral within 6 months of surgery.
Results:
A total of 1125 patients met inclusion criteria. Endoscopic release was performed in 634 (56%) cases and open release in 491 (44%). Unadjusted analysis revealed no difference in number of patients requiring refills (6.0% vs 7.1%, P = .44), mean number of refills among those requiring one (1.29 vs 1.23, P = .69), total oral morphine equivalents (45.1 vs 44.7, P = .84), number of patients calling regarding pain (12.8% vs 14.7%, P = .36), OT referrals (12.1% vs 11.4%, P = .71), or average number of OT visits (4.5 vs 4.2, P = .74) for endoscopic and open techniques, respectively. Adjusted analysis revealed lower age, lower body mass index, and history of muscle relaxant as predictors of opioid refills, and in contrast to the unadjusted analysis, operating surgeon and surgical technique were predictors of referral to OT.
Conclusion:
Endoscopic CTR and OCTR did not differ in terms of unadjusted postoperative patient calls for pain, number of opioid refills, or OT referrals. After correcting for individual surgeon practice, endoscopic was associated with decreased odds of requiring postoperative OT.
Introduction
Carpal tunnel syndrome (CTS) is the most common compressive neuropathy with greater than 400 000 surgical releases performed annually in the United States. 1 The key to successful treatment is full release of the transverse carpal ligament, which can be accomplished in an open or endoscopic fashion. Since the endoscopic approach was first described in 1989, 2 theoretical benefits of reduced postoperative pain, expedited grip strength recovery, earlier return to work and activities of daily living, and decreased scar tenderness and pillar pain have been heavily studied in multiple randomized controlled trials.3,4 Meta-analysis of these trials has supported some, but not all of these claims. Meta-analysis supported earlier return to work, improved early postoperative grip strength, and decreased scar tenderness, but also discovered increased risk of transient nerve injury. 3
Although the study of postoperative pain associated with each technique has been extensive, studies translating these findings to postoperative pain medication requirements have been limited. Ilyas et al 5 noted a trend toward decreased postoperative oxycodone use in endoscopic carpal tunnel release (ECTR) versus open carpal tunnel release (OCTR), but the difference did not reach statistical significance, and the study was limited by small sample size and short follow-up. With the high volume of carpal tunnel releases (CTRs) performed annually, even a small difference in opioid requirements may have a significant effect on the societal opioid epidemic as 13% of opioid-naïve hand surgery patients continue filling narcotics 90 days after surgery, 6 and hand surgeons prescribe 2 to 5 times more opioids than patients use—creating risk for abuse, misuse, and diversion.7 -9
In addition to postoperative pain medications, some patients are referred for occupational therapy (OT) during their recovery from carpal tunnel surgery. In a prospective randomized study, patients underwent short incision CTR and were randomized into 2 treatment groups: Both groups received instructions on home exercises to aid with nerve gliding while the experimental group also received 2 weeks of supervised hand therapy. Supervised therapy failed to show improvement in any of the metrics measured, including grip strength, pain, and time to returning to work. 10 Although the routine use of therapy is not the standard of care, a review of large insurance claims database revealed up to 17.5% of patients are prescribed OT following CTR averaging 5 to 6 visits and costing an additional $450. 11 Compared with OCTR, Zhang et al 12 found a trend toward decreased OT costs after ECTR; however, to our knowledge, no study has compared therapy referrals following the 2 procedures.
Given the high prevalence of CTS requiring operative intervention, outcomes associated with either OCTR or ECTR may have a profound impact on society and the health care system. In this article, we investigate 2 aims examining how endoscopic and open approaches to CTR compare in relation to postoperative: (1) opioid prescription patterns; and (2) OT referrals.
Methods
Study Population
Study approval was granted by the institutional review board of The Ohio State University Wexner Medical Center. Retrospective chart review was performed to identify all patients who underwent either ECTR or OCTR between September 1, 2017, and November 19, 2019, by our fellowship-trained hand surgeons at our institution. In total, 2000 patients were identified using CPT codes 29848 and 64721 corresponding to ECTR and OCTR, respectively. Inclusion criteria included patients with idiopathic CTS requiring operative intervention. Exclusion criteria included patients undergoing simultaneous bilateral release, revision surgery, multiple procedures at once (eg, trigger finger release, cubital tunnel release, carpometacarpal (CMC) arthroplasty), or traumatic CTS. Baseline patient characteristics, including age; sex; body mass index (BMI); preoperative opioid, anxiolytic, or muscle relaxant use; diabetes; smoking; alcohol; and drug use were documented. Operating surgeon and type of anesthesia (local only, local plus sedation, or local plus general), and multimodal pain prescriptions (ibuprofen and acetaminophen) were also included. Although most providers adhered to an established protocol (5 tablets of 5 mg oxycodone) for postoperative narcotic prescribing, initial oral morphine equivalents (OMEs) were recorded to assess for potential variance from the protocol.
Surgical Techniques
Each CTR was performed by 1 of 7 hand fellowship–trained surgeons (4 orthopedic trained and 3 plastic surgery trained) based on surgeon preference. Three of the surgeons performed predominantly or only endoscopic release and 4 performed predominantly or only open release. The open release varied slightly between surgeons, but generally was performed through a 2.5 cm incision at the base of the palm and dissected down to the transverse carpal tunnel which was divided distally into the palmar fat pad and proximally 1 to 2 cm proximal to the wrist crease with digital palpation confirming complete release. The endoscopic technique was performed through a small transverse incision in the distal wrist crease with dissection carried down to the transverse carpal ligament which was then divided using several passes of the endoscope from distal to proximal. In addition, antebrachial fascia of the distal forearm was incised with scissors under direct visualization.
Outcomes
Two primary outcomes were the focus of the study: (1) number of patients requiring an opioid refill within 6 months after surgery; and (2) number of patients requiring an OT referral within 6 months of surgery. For each patient, all postoperative clinic and telephone encounters with our clinic were reviewed within the electronic medical record system to identify opioid refills and OT referrals related to their CTR surgery. Occupational therapy referrals were offered to patients during follow-up visits if they demonstrated difficulty with range of motion, scar tenderness, or difficulty returning to activities of daily living. Secondary outcomes included total OMEs prescribed, total number of therapy visits, and number of patient phone calls regarding postoperative pain. Phone calls were examined to serve as an additional metric of outpatient resource utilization, but also to serve as an internal control taking into account that providers may have different thresholds for providing narcotic refills.
Statistical Analysis
The χ2 tests and Fisher exact tests were used to compare categorical variables as indicated. The Student t test was used to compare means of continuous variables. Multivariable linear regression was used to identify predictors of the number of patients requiring refills postoperatively; a separate regression was used to identify predictors of the number of patients requiring OT postoperatively. Variables examined included operating surgeon; surgical technique; age; sex; preoperative opioid, anxiolytic, and muscle relaxant use; diabetes; smoking; BMI; and type of anesthesia. To account for clustering at the surgeon level, a sensitivity analysis was performed using a multilevel binary logistic regression. Stata 16.1 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, Texas: StataCorp LLC) was used to perform statistical analysis.
Results
Of the 2000 patient charts reviewed, 1125 (56%) met inclusion criteria. Endoscopic release was performed in 634 (56%) cases and open release in 491 (44%). Both cohorts were well matched in terms of baseline characteristics and did not differ in mean age, BMI, sex, smoking history, alcohol use, illicit drug use, or preoperative opioid, anxiolytic, or muscle relaxant use (Table 1). Each group was prescribed similar amounts of OMEs (40.5 vs 38.7, P = .147), acetaminophen (32.6% vs 34%, P = .63), and nonsteroidal anti-inflammatories (NSAIDs; 27.0% vs 29.3%, P = .38) on the day of surgery; and similar types of anesthesia (local only or sedation: 92.9% vs 92.9%, general: 7.1% vs 7.1%; χ2 P = .99) for endoscopic and open techniques, respectively (Table 2). The most common postoperative regimen was 5 tablets of oxycodone 5 mg with instructions to take over-the-counter NSAIDs and acetaminophen scheduled around the clock. Primary outcomes were statistically equivalent with similar rates of narcotic refills (6.0% vs 7.1%, P = .44) and rates of OT referrals (12.1% vs 11.4%, P = .71) for endoscopic and open techniques, respectively (Figure 1). Secondary outcomes were also similar with equivalent mean number of refills among patients requiring a refill (1.29 vs 1.23, P = .69), total OMEs prescribed (40.5 vs 38.7, P = .84), OT visits (4.5 vs 4.2, P = .74), and rate of patient phone calls related to postoperative pain (12.8% vs 14.7%, P = .36) for endoscopic and open techniques, respectively (Figure 1).
Demographic Characteristics for ECTR and OCTR Cohorts.
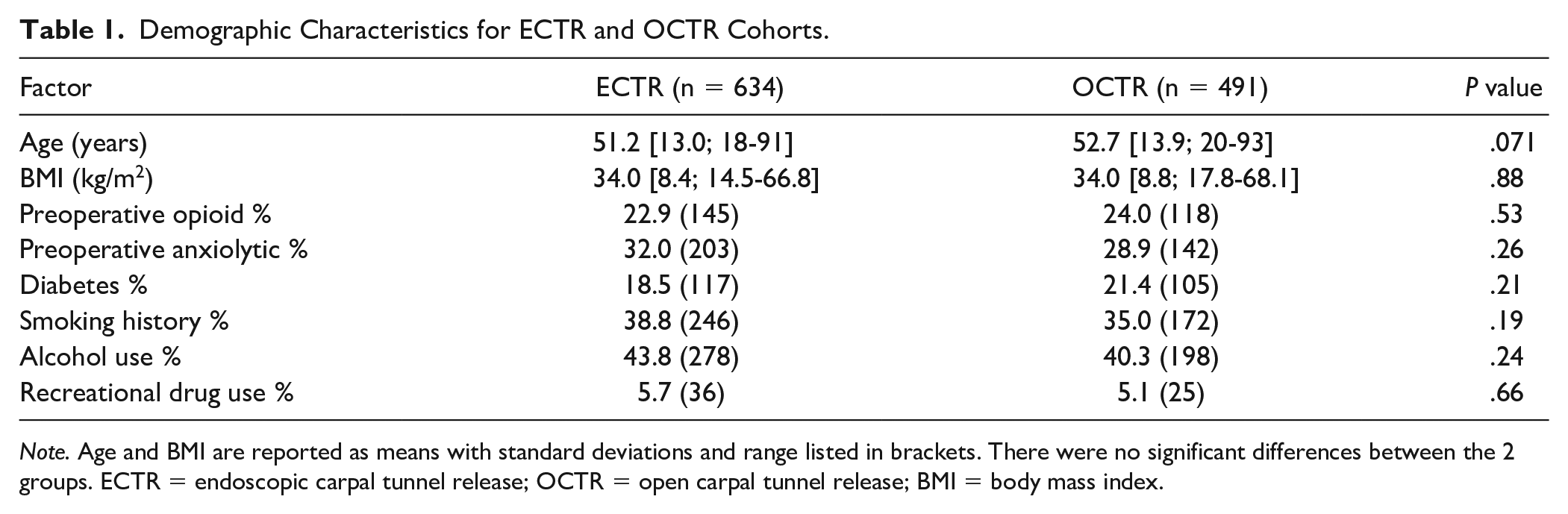
Note. Age and BMI are reported as means with standard deviations and range listed in brackets. There were no significant differences between the 2 groups. ECTR = endoscopic carpal tunnel release; OCTR = open carpal tunnel release; BMI = body mass index.
Opioid Prescription Patterns, Patient Calls for Pain, and Therapy Requirements for Patients Undergoing ECTR and OCTR.
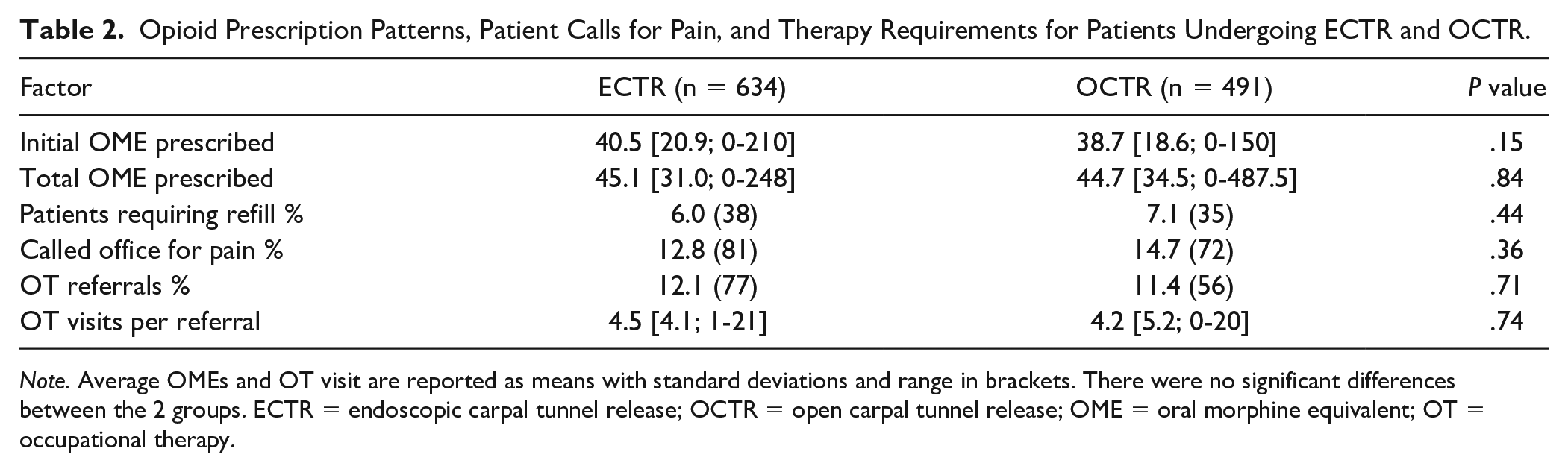
Note. Average OMEs and OT visit are reported as means with standard deviations and range in brackets. There were no significant differences between the 2 groups. ECTR = endoscopic carpal tunnel release; OCTR = open carpal tunnel release; OME = oral morphine equivalent; OT = occupational therapy.
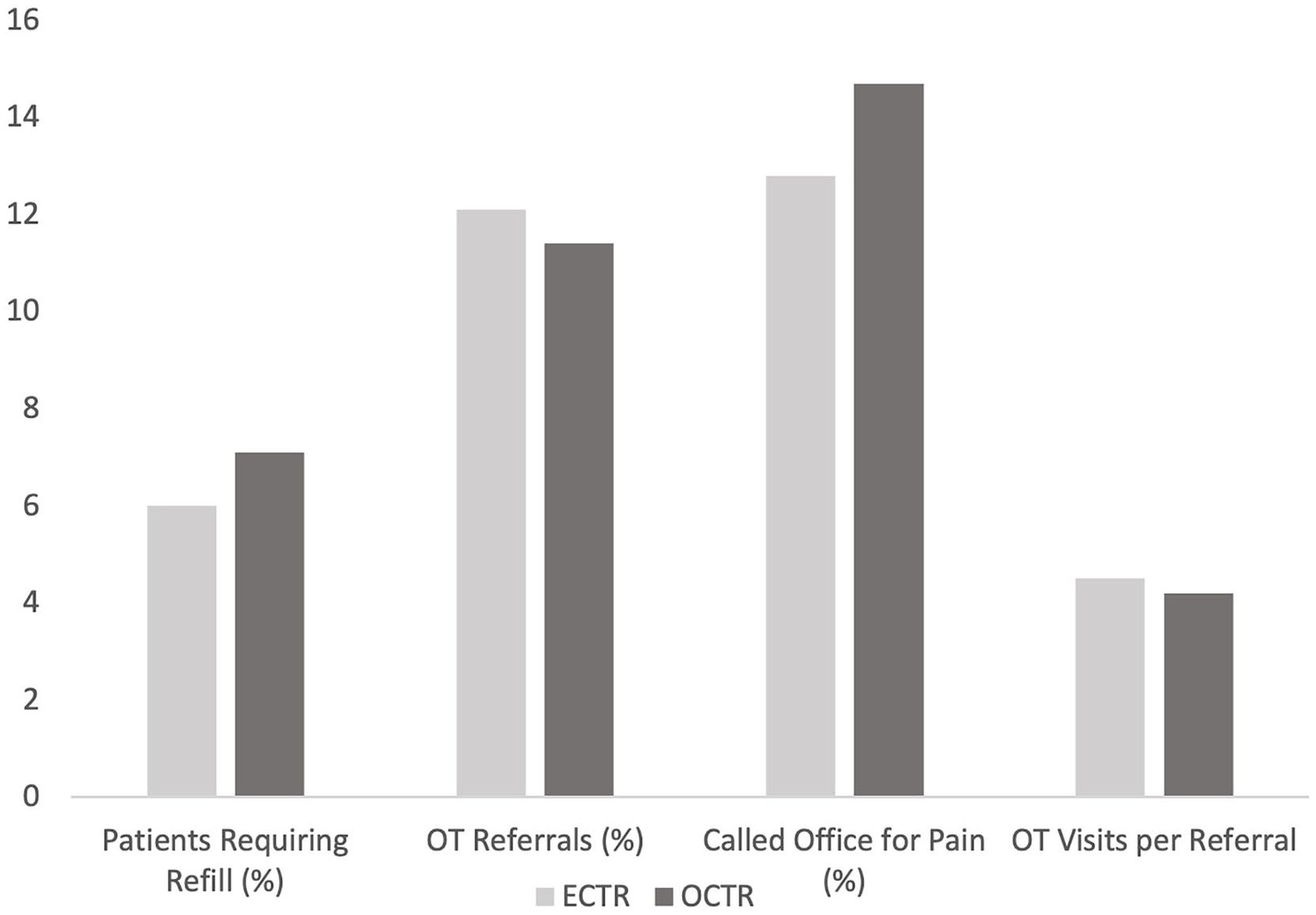
Graph of primary (refills and OT referrals) and secondary (calls for pain, OT visits per referral) outcomes. There were no significant differences between the 2 groups.
Multivariable binary regression identified current muscle relaxant use as a predictor of requiring an opioid refill, whereas increased age and BMI were predictors of not requiring an opioid refill (Table 3). That is, as age increased and BMI increased, patients were less likely to require an opioid refill. Importantly, surgical technique, that is, endoscopic or open, was not a predictor of requiring an opioid refill (Table 3). Of note, operating surgeon was also not a predictor of requiring an opioid refill indicating each surgeon in the study prescribed opioids at similar rates (Table 3).
Multivariable Binary Regression on Requiring an Opioid Refill.
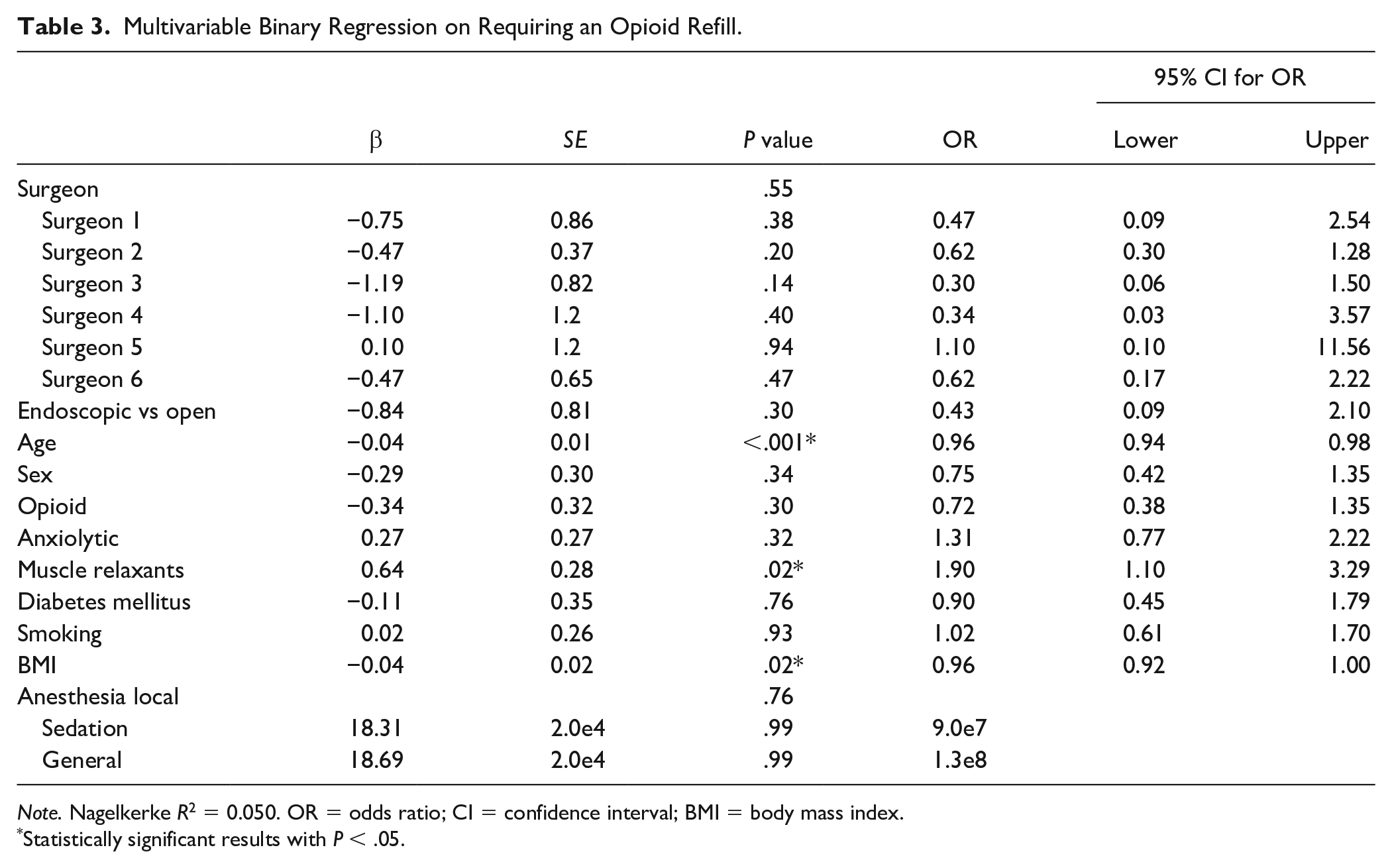
Note. Nagelkerke R2 = 0.050. OR = odds ratio; CI = confidence interval; BMI = body mass index.
Statistically significant results with P < .05.
A separate multivariable binary regression was performed to identify predictors of requiring an OT referral. Operating surgeon was predictive with surgeon 2 and surgeon 4 less likely to refer patients to OT (β = −1.617, P = .025, and β = −1.372, P = .046, respectively; Table 4). Surgeon 2 performed predominately ECTR (294 of 295 cases) and surgeon 4 performed predominately OCTR (16 of 18 cases). Male sex (β = −0.584, P = .013) and increased BMI (β = −0.025, P = .032) were also negative predictors of referral to OT (Table 4). Last, endoscopic technique (β = −1.430, P = .035) was also a negative predictor of being referred to OT. In other words, after controlling for operating surgeon, patients undergoing open release were 4.18 times more likely to be referred to OT compared with those undergoing endoscopic release (odds ratio [OR] = 4.184, P = .035; Table 4).
Multivariable Binary Regression on Requiring an OT Referral.
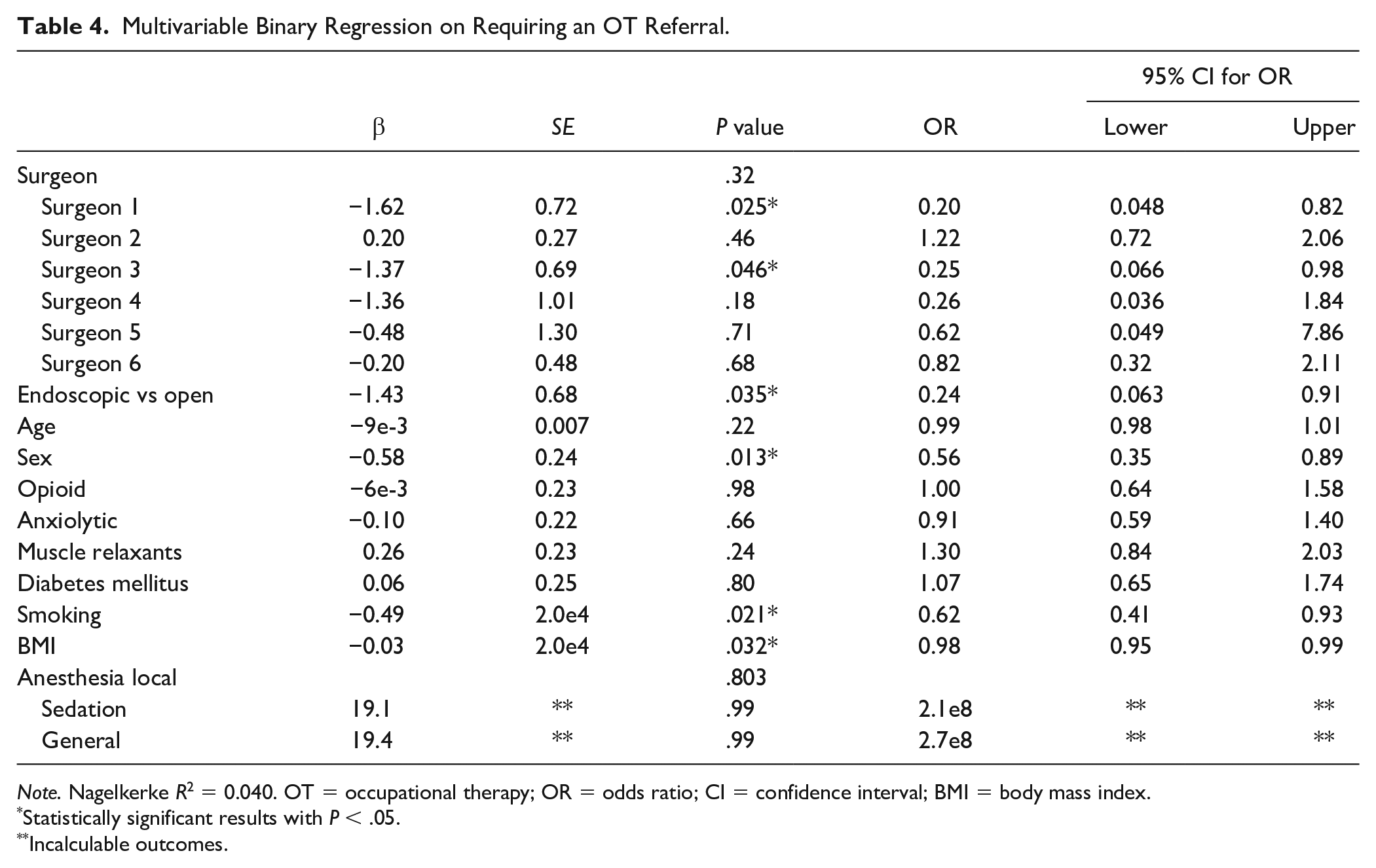
Note. Nagelkerke R2 = 0.040. OT = occupational therapy; OR = odds ratio; CI = confidence interval; BMI = body mass index.
Statistically significant results with P < .05.
Incalculable outcomes.
To account for clustering at the surgeon level, a sensitivity analysis was performed using a multilevel binary logistic regression; no statistically significant clustering was identified with respect to opioid refills and OT referrals with an interclass correlation of less than 0.001 for each outcome.
Discussion
The aim of our study was to compare endoscopic and open approaches to CTR as each relates to postoperative opioid refills and OT referrals. Both endoscopic and open techniques were associated with similarly low rates of opioid refills of 6.0% and 7.1%, respectively, and did not differ in terms of total OMEs prescribed. A previous study of a large insurance database found preoperative opioid use, drug and substance abuse, and depression are positive predictors of prolonged postoperative opioid use. 13 Another prospective study identified age and sex as predictors of post CTR opioid consumption. 7 In our study, each cohort had similar rates of these potential confounding variables (Table 1). Furthermore, both groups were prescribed similar OMEs and nonopioid medications on the day of surgery. Also, because opioid refills are often prescribed over the phone after the patient has called reporting pain, it was considered there may be provider-dependent thresholds for prescribing pain medications during these calls. Therefore, the rates of patient phone calls regarding pain was recorded for each cohort and found to be similar with 12.8% and 14.7% of patients calling following endoscopic and open releases, respectively. Operating surgeon was also included in the multivariable binary regression to further scrutinize the potential for provider-dependent variations in opioid prescribing but was not in fact a predictor of prescribing an opioid refill (Table 3). Last, the multivariable binary regression, controlling for potential confounding variables, found surgical technique was not a statistically significant predictor of requiring an opioid refill (Table 3). In consideration of these findings, our study suggests rates of postoperative opioid refills are similar following carpal tunnel surgery irrespective of endoscopic or open approach.
Occupational therapy referrals were also similar between the endoscopic and open cohorts. In the endoscopic group, 12.1% of patients were prescribed therapy with an average of 4.5 visits compared with 11.4% of patients in the open group with an average of 4.2 visits. Although the unadjusted odds for requiring an OT referral were similar between endoscopic and open techniques, the adjusted OR revealed patients undergoing open release had 4.18 times greater odds of being referred to OT compared with patients receiving an endoscopic release (Table 4). The stark difference between the adjusted and unadjusted results seemed to be secondary to the effect of the operating surgeon. All surgeons prescribed OT for similar clinical indicators including persistent pillar pain, scar tenderness, and decreased range of motion unrelieved by scar massage, ice, elevation, and home exercises; however, no objective criteria or rating scales were used. Both surgeon 2 and surgeon 4 were significantly less likely to refer a patient to OT suggesting a difference in practice standards compared with the other surgeons in the study. To confirm the effect of operating surgeon, an additional regression without operating surgeon was performed and the adjusted OR was similar for both the endoscopic and open techniques (Supplemental Table 1). These finding suggest that after correcting for individual surgeon practice, a patient undergoing open technique is 4.18 times more likely to be referred for postoperative OT, but the duration of therapy remains similar for both techniques.
Although open and endoscopic techniques for CTR have been extensively compared against one another, to our knowledge, this has been the first study to directly compare the 2 techniques as they relate to postoperative opioid and therapy prescribing patterns. Although our study is limited by its retrospective nature and lack of surgeon standardization regarding postoperative care, these limitations are minimized and addressed with well-matched cohorts and use of multivariable binary regressions. We found postoperative opioid refills are similar following carpal tunnel surgery irrespective of endoscopic or open approach. We acknowledge that the design of our study does not allow us to compare the actual consumption of opioids, but argue the amount dispensed is equally important as it relates to the opioid burden on society. Because of the high volume of CTS surgery performed annually, number of refills is an important metric to track as refills have the potential to introduce access of a high volume of narcotics to the public risking distribution and misuse. To minimize this risk, future studies may investigate opioid-sparing protocols as recent findings show equivalent patient satisfaction and functional outcomes with nonopioid regimens. 14 Our findings provide evidence that such protocols can be developed irrespective of surgical technique.
Previous reports of earlier return to work, improved early postoperative grip strength, and decreased scar tenderness associated with ECTR 3 are consistent with the results observed in our study as these outcomes are closely related to need for postoperative OT. Although regression analysis revealed decreased odds of OT referral with endoscopic technique, the unadjusted OR was similar due to variations in therapy referrals based on operating surgeon. This interprovider variation is an important finding when considering health care spending especially when acknowledging there is limited evidence supporting therapy interventions following CTS surgery. Therefore, future development of guidelines for therapy referrals may help reduce health care costs associated with carpal tunnel surgery and further help in comparing these 2 techniques.
Conclusion
Given the high prevalence of CTS requiring operative intervention, outcomes associated with either OCTR or ECTR may have a profound impact on society and the health care system. In this article, we investigated how endoscopic and open approaches to CTR compare in relation to postoperative opioid prescription patterns and OT referrals. We found postoperative opioid refills are similar following carpal tunnel surgery irrespective of endoscopic or open approach, and after correcting for individual surgeon practice, endoscopic technique is associated with decreased odds of requiring postoperative OT.
Supplemental Material
sj-docx-1-han-10.1177_15589447221130092 – Supplemental material for Open Versus Endoscopic Carpal Tunnel Release: A Comparison of Opioid Prescription Patterns and Occupational Therapy Referrals
Supplemental material, sj-docx-1-han-10.1177_15589447221130092 for Open Versus Endoscopic Carpal Tunnel Release: A Comparison of Opioid Prescription Patterns and Occupational Therapy Referrals by Michael J. Schroeder, Nihaal Reddy, Andrew Rust, Andrew L. O’Brien and Sonu A. Jain in HAND
Footnotes
Ethical Approval
This study was approved by our Biomedical Institutional Review Board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was not required for this retrospective study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.