
Abstract
Background:
Targeted muscle re-innervation (TMR) is increasingly being used for treatment of postamputation pain and myoelectric prosthesis (MYP) control. Palmaris longus (PL) is a potential target following transradial amputation. The purpose of this study was to determine the branching pattern of the median nerve (MN) as it pertains to the PL motor branch entry point (MEP) and to present clinical results of patients who had PL used as a target.
Methods:
Eight cadaveric arms were dissected and branching patterns of the MN were documented. Additionally, we reviewed adult patients from a prospectively collected database who underwent TMR using PL. We recorded patient-reported outcomes and signal strength generated by the PL.
Results:
The average distance from the medial epicondyle to PL MEP was 53 mm. All palmaris motor branches passed through a chiasm within the flexor digitorum superficialis muscle belly, which was a mean of 18 mm away from the MN proper. Patients with long-term follow-up reported an average Pain visual analog scale of 3.3 and Disabilities of the Arm, Shoulder and Hand of 46.2. All but one patient were using an MYP, and all generated at least 10 mV of signal from the PL, which is ample signal for surface electrode detection and MYP control. There were no postoperative neuromas and only one patient-reported postoperative phantom limb pain.
Conclusions:
Palmaris longus is a suitable target for TMR. Our objective measurements and anatomic relationships may help surgeons consistently find the PL’s motor branch. Our series of patients reveal sufficient signal strength and acceptable clinical outcomes following TMR using the PL.
Keywords
Introduction
In the United States, there are over 2 million people living with loss of a limb. 1 Unfortunately, over half of these individuals will develop significant post-amputation pain. Post-amputation pain can have a major impact on patients’ psychological well-being leading to depression and anxiety, it can increase opioid consumption and addiction, and it is a primary reason that up to 30% of amputees abandon the use of a prosthesis. Globally, these factors negatively impact healthcare costs and unemployment rates. The pain is attributed to 2 distinct but highly related processes: residual limb pain (RLP) and phantom limb pain (PLP).2,3 Residual limb pain or “stump pain” is localized to the residual limb and is often described as sharp, burning, and electrical in either a superficial location or deep within the limb. Etiologies are diverse and include painful scar tissue, heterotopic ossification, and neuroma formation. 2 Phantom limb pain is described by patients as originating from their missing body part and is more commonly dull, squeezing, and cramping in nature. In both cases, neuroma formation (aberrant nerve regeneration resulting in ectopic afferent input) is thought to contribute to these sensations of pain. 2
Many strategies have been attempted to treat post-amputation pain with variable success. Targeted muscle reinnervation (TMR) is a relatively new technique that has been shown to effectively treat both PLP and RLP.4,5 Additionally, TMR can serve a second, functional, role by optimizing myoelectric signals that can be utilized for prosthesis control.
Briefly, this technique reroutes the amputated, residual nerve stumps that have lost their distal targets and transfers them to the motor branches of residual, more proximal muscles. 6 By providing a distal target and a vascularized scaffold on which to guide axonal sprouting, TMR prevents the formation or reformation of painful neuromas and allows for intuitive control of myoelectric prosthetics through muscular contraction caused by the redirected efferent action potentials. 7
While appealing, successful TMR requires appropriate selection of target muscles. This can be quite difficult depending on the specifics of each amputation. For this reason, Pierrie et al developed a list of criteria that should be met when selecting a target muscle intended for both symptom treatment and myoprosthesis control. The criteria include the following: the muscle must be in close proximity to the donor nerve (to permit a tension free coaptation), it should not be fibrosed or scarred, it should be superficial, it should be expendable (inconsequential or redundant), and it should be either traumatically or surgically denervated at the time of the TMR procedure. 6
Following transradial amputations, 1 target option (if present) is the palmaris longus (PL) muscle as it commonly meets all of the aforementioned criteria. However, while the general branching pattern of the median nerve is well documented,8,9 the specific branches of the median nerve to the PL muscle have not been described. Furthermore, functional and patient-reported outcomes have not been reported for patients following the use of PL as a target post-amputation.
The purpose of this study is twofold: First, it elucidates the anatomical branching pattern of the median nerve as it pertains to the PL motor branch. Second, it provides a case series reporting the outcomes of patients who underwent TMR using the PL as a target.
Materials and Methods
Cadaveric Dissection (Supplemental Video 1)
Six embalmed and 2 fresh frozen cadaver arms with a mean age at death of 78 were utilized for dissection. There were 6 left arms and 2 right arms with a palpable PL tendon. A longitudinal skin incision was extended from the midpoint of the proximal wrist crease and terminated on the medial aspect of the forearm, 5 cm proximal to the elbow flexion crease (Figure 1). The presence of a PL tendon was confirmed, and dissection began at the level of the elbow. We identified the main trunk of the median nerve, medial and deep to the biceps tendon, and followed the nerve proximal-to-distal identifying each of its branches, starting with the most proximal branch to pronator teres (PT) and ending with the branching of the anterior interosseous nerve (AIN). Each branch encountered was isolated and traced toward the muscle belly until the motor entry point was visually confirmed. The tendons of the PL, PT, and flexor carpi radialis (FCR) were divided distally, and reflected proximally, to ease the dissection and accurately identify the termination of each nerve branch into the muscle motor entry point (MEP).
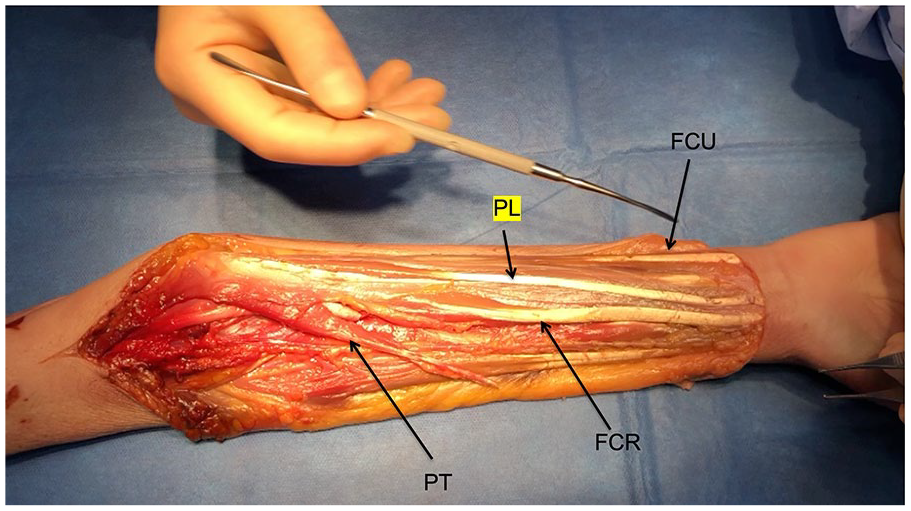
Example of extensile exposure of the volar forearm musculature.
The previously reflected muscles were positioned anatomically and nerve branching patterns were recorded. With the elbow in full extension and supination, the distance was measured using a digital caliper between constant bony landmarks—medial epicondyle (ME) to ulnar styloid (US), ME to common FCR-PL nerve trunk (containing the nerve to PL), ME to PL MEP, and median nerve to the flexor digitorum superficialis (FDS) fascial chiasm.
Clinical Series
For the clinical portion of our study, International Review Board approval for chart review as well as data collection on transradial amputee patients treated at our institution from 2016 to 2019 was obtained. A query of our prospective database of transradial amputees was performed to identify patients who had undergone a transradial amputation and TMR utilizing the PL muscle as a target either at the index surgery or in a delayed fashion.
Demographic data on sex, age, race, diagnosis, hand dominance, and follow-up period were recorded. Subjective patient reported outcome data were collected. These included visual analog scale (VAS) for pain and Disabilities of the Arm, Shoulder and Hand (DASH) scores. Finally, objective data on resultant PL signal strength, prosthesis usage, and associated phantom limb sensation and pain were recorded.
TMR to PL Surgical Technique (Clinical Series)
In all cases, the same surgical technique was used for TMR to the PL. The motor nerve to the PL was identified (see details for identification below) and transected 1 to 2 cm proximal to the MEP. The proximal nerve end was not formally addressed given that it does not contain somatosensory nerve endings. Next, the preselected donor nerve (median or ulnar) was coapated to the distal PL motor nerve stump. A tension free end-to-end coaptation was performed using 8-0 nylon simple interrupted sutures. Additionally, due to the size mismatch that is often encountered between the nerve ends, the coaptation was augmented with a epineurium-to-epimysium neurorrhaphy was performed using 6-0 nylon suture as described by Pierrie et al 6
Results
Cadaveric Study
There was a consistent pattern of a single PL motor nerve, branching in a common trunk together with the nerve to FCR, which was identified in all 8 cadaver arms. While there was a variable amount of interconnection between the PL and FCR trunks, in every cadaver a consistent trajectory of the terminal PL nerve was identified. After terminally branching from the FCR-PL nerve trunk, the PL motor nerve proper passed through a myofascial chiasm found in the proximal FDS muscle prior to innervating the PL (Figures 2 and 3).
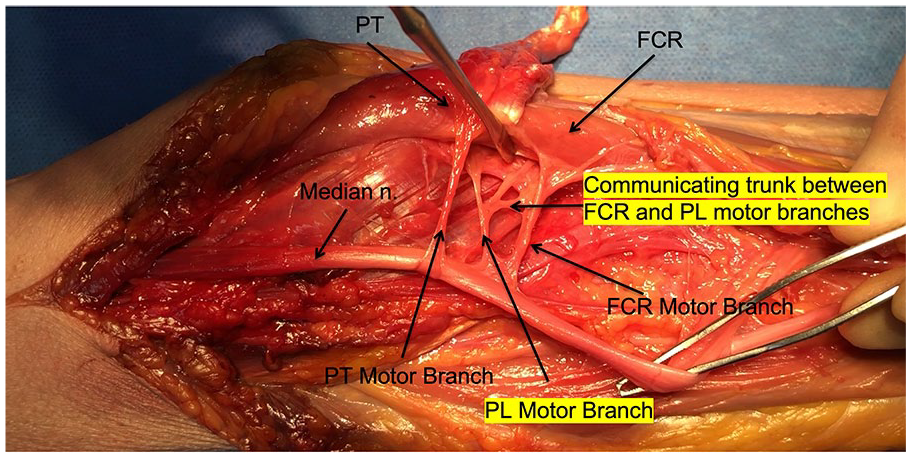
Motor branches to the flexor capri radialis, pronator teres, and the palmaris longus.
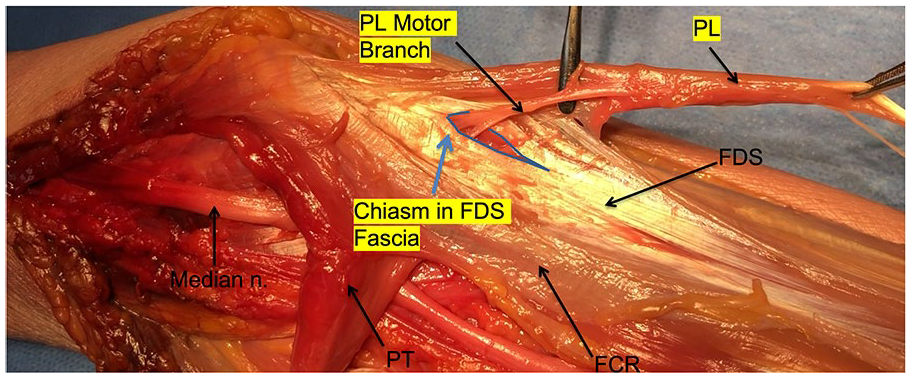
Palmaris longus motor branch penetrating the flexor digitorum superficialis fascia.
The average length of the forearms from ME to US was 25 cm (21-29 cm), the average length from the ME to the FCR-PL nerve trunk was 31 mm (8-40 mm), the average length from ME to palmaris muscle motor entry point was 53 mm (30-77 mm). Additionally, all palmaris motor branches passed through a tunnel within the FDS muscle belly, the average distance of which was 18 mm (7-36 mm) away from the median nerve proper (Table 1).
Median Nerve Branching: Relevant Anatomic Relationships.
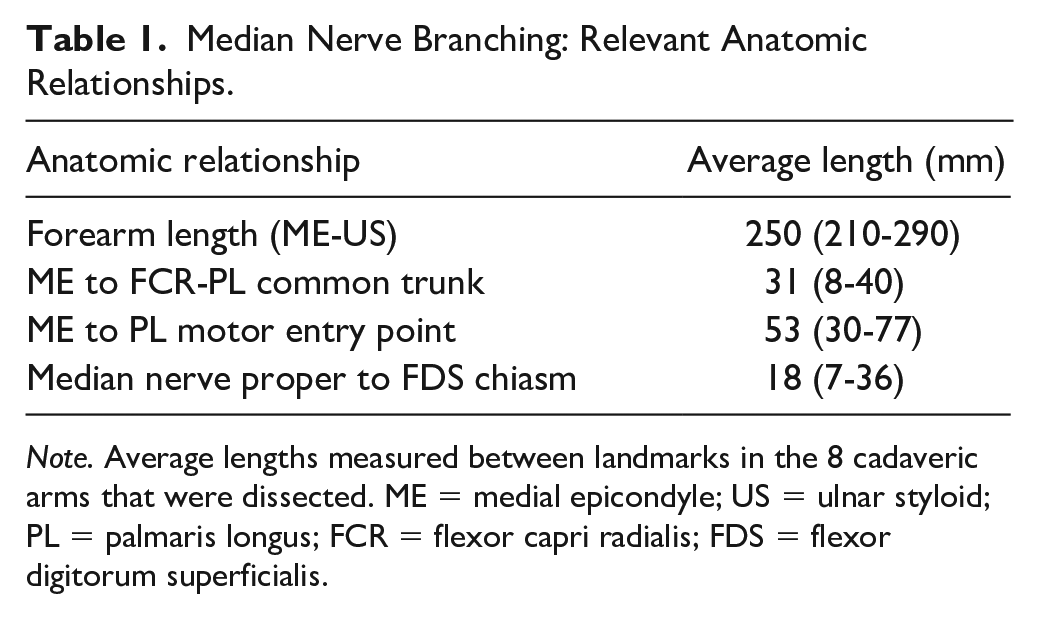
Note. Average lengths measured between landmarks in the 8 cadaveric arms that were dissected. ME = medial epicondyle; US = ulnar styloid; PL = palmaris longus; FCR = flexor capri radialis; FDS = flexor digitorum superficialis.
Clinical Study
The prospectively collected amputee database at our institution was reviewed to identify 7 patients with 8 upper extremities where PL was utilized as a TMR target for transradial amputation. The average patient age at the time of TMR was 48 years (range: 39-68). Three patients were female and 4 were male. One patient underwent bilateral amputations. The reason for amputation was trauma in 4 patients, vasopressor-induced ischemia in 2 patients (3 arms), and peripheral vascular disease in 1 patient. The delay between amputation and TMR procedure was 266 days on average (range: 0-1236 days). The PL muscle branch was utilized as a target for the median nerve in 3 patients and for the ulnar nerve in 4 patients (5 extremities) (Table 2).
Demographics.
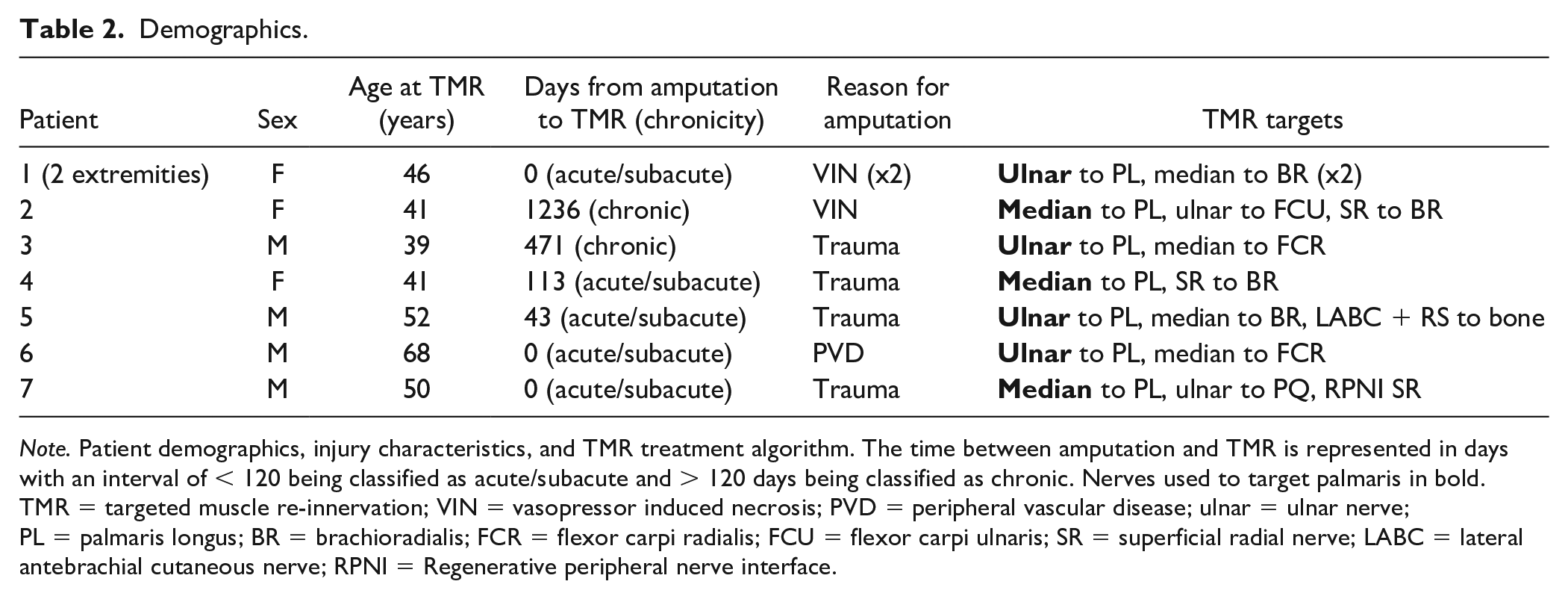
Note. Patient demographics, injury characteristics, and TMR treatment algorithm. The time between amputation and TMR is represented in days with an interval of < 120 being classified as acute/subacute and > 120 days being classified as chronic. Nerves used to target palmaris in bold. TMR = targeted muscle re-innervation; VIN = vasopressor induced necrosis; PVD = peripheral vascular disease; ulnar = ulnar nerve; PL = palmaris longus; BR = brachioradialis; FCR = flexor carpi radialis; FCU = flexor carpi ulnaris; SR = superficial radial nerve; LABC = lateral antebrachial cutaneous nerve; RPNI = Regenerative peripheral nerve interface.
Long-term follow-up was available for 5 out of the 7 patients (7 extremities), with 1 patient lost to follow-up after her first postoperative visit. Average duration of follow-up as 18 months (range: 1-47 months). The 6 longer term patients reported an average pain VAS of 3.2 and DASH of 46.2 (moderate disability) at final follow-up. All transradial amputees were successfully using a prosthesis, with all but 1 utilizing a myoelectric prosthesis (Table 3). Only one of these patient reported experiencing phantom pain. Importantly, signal strength following TMR was assessed in each of these 5 long-term follow-up patients, and they were found to generate over 10 mV from each of their targets (including the PL), which is a standard minimal threshold for adequate signal strength for detection by surface electrodes and control of a myoelectric prosthesis. Additionally, at every follow-up visit patients were assessed for the development of symptomatic neuromas using Eberlin’s criteria. 10 None of the patients were found to develop a neuroma at any of their target sites throughout the duration of their follow-up (Tables 4).
Patient Reported Outcomes.
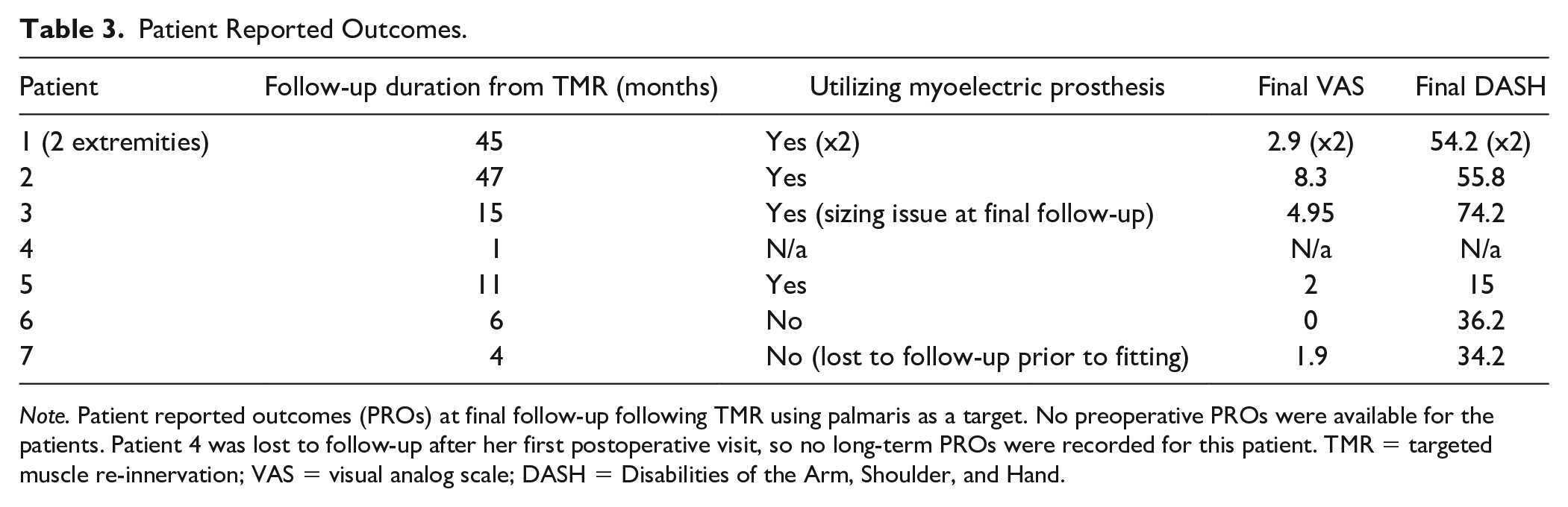
Note. Patient reported outcomes (PROs) at final follow-up following TMR using palmaris as a target. No preoperative PROs were available for the patients. Patient 4 was lost to follow-up after her first postoperative visit, so no long-term PROs were recorded for this patient. TMR = targeted muscle re-innervation; VAS = visual analog scale; DASH = Disabilities of the Arm, Shoulder, and Hand.
Residual/Phantom Limb Outcomes.
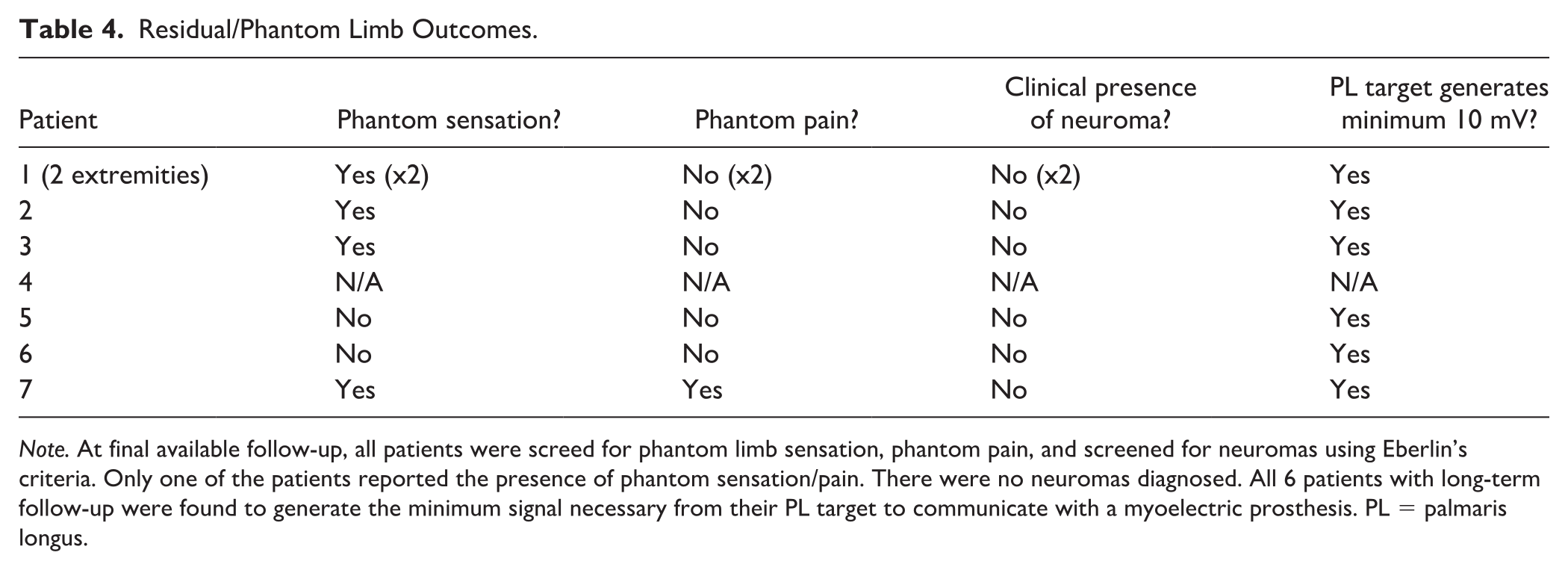
Note. At final available follow-up, all patients were screed for phantom limb sensation, phantom pain, and screened for neuromas using Eberlin’s criteria. Only one of the patients reported the presence of phantom sensation/pain. There were no neuromas diagnosed. All 6 patients with long-term follow-up were found to generate the minimum signal necessary from their PL target to communicate with a myoelectric prosthesis. PL = palmaris longus.
We further stratified the patients according to the timing of the TMR procedure. When TMR was performed within 120 days after the index amputation, this was classified as “acute/subacute.” When TMR occurred after 120 days, this was classified as “chronic.” Five patients (6 extremities) stratified into the acute/subacute TMR group and 2 patients into the chronic TMR group. The acute group average VAS score was 2 and the chronic group was 6.6. The DASH score for the acute group was 38.8, and for the chronic group it was 65.
Discussion
Major extremity amputations take a substantial psychosocial, economic, and clinical toll on individual patients and the medical community. Targeted muscle reinnervation is a promising surgical technique used concomitantly or following upper and lower extremity amputations. Targeted muscle re-innervation serves a dual purpose by treating RLP and PLP, which plague over 50% of all amputees and helps patients regain function by improving intuitive myoelectric prosthetic control. Myoelectric prosthetics function by transcutaneously recording electrical signals produced by muscles in the residual limb. The prosthetics then convert these signals into upper extremity functions such as thumb abduction and opposition, grasp, digital extension, and forearm rotation. 6 However, the ideal muscular targets for TMR have not yet been fully elucidated for transradial amputees. When selecting targets, surgeons must select muscles that are expendable, have satisfactory bulk to generate sufficient contraction, and are superficial enough to be clearly detected by the cutaneous sensors located within prosthetics.
The PL meets the above criteria and is therefore an attractive target for TMR following transradial amputation. It is superficial, expendable, and in close proximity to the median and ulnar nerves which allows for a direct, tension-free coaptation. This is not to suggest that the PL is superior to other potential targets that meet these criteria (ie, the FCR and PT), but rather it is useful addition. In our practice, we have found that the anteromedial and superficial location of the PL places it in an excellent location for communication with surface electrodes. When used as a target for the median nerve, contraction of the PL provides an intuitive signal for thumb opposition in the myoelectric hand prosthesis. Additionally, this location avoids compressive pressure from the radial and ulnar molds of forearm level prosthetics. These molds can otherwise cause pain and irritation by compressing underlying TMR innervated muscles.
The specific branching of the PL nerve has not been well described previously. Through dissection of 8 cadaveric arms we found that the motor branch to the PL invariably originated from a common trunk (including the motor branch to the FCR) and then traversed a myofascial tunnel in the proximal FDS (roughly 1-4 cm from the median nerve proper) prior to innervating the PL. Though the specific distance varied based on patient size, this is a consistent observation in the lab as well as the operating room. We have found that elevating the PL muscle in a distal to proximal direction facilitates identification of this pedicle as it penetrates the tunnel in the FDS musculature and is the most reliable method to identify the target nerve. As the interest in peripheral nerve surgery grows, it has become apparent that the specific anatomic relationships of many nerve branches are not well documented in the literature with the level of detail required by a peripheral nerve surgeon. Thus, defining this pattern makes the PL a more readily accessible target for surgeons.
Comparing clinical outcomes based on the recipe of muscles utilized for TMR in transradial amputation is complex and any direct conclusions regarding the superiority of PL as a target are not possible given the small sample size and multiple potential confounding factors in this patient cohort. However, it is encouraging to see that when PL was utilized as a target in this cohort it generated sufficient signals for myoelectric prosthetic control and with good clinical outcomes. Importantly, none of the patients in this cohort developed symptomatic neuromas based on Eberlin’s criteria. Low mean pain VAS scores were reported across all subjects at 3.3 with none of the patients reporting symptoms of PLP. Patients involved in the study were found to have moderate disability with a mean DASH score of 46.2.
Interestingly, however, when stratified based on timing of TMR the acute group had a mean VAS and DASH scores of 2 and 38.8, respectively, versus 6.6 and 65 in the chronic group. Though this study is a case series and is underpowered to draw any statistical conclusions, it is likely that timing of TMR impacts symptoms following amputation. The existing literature supports the use of TMR both acutely and in a delayed fashion following amputation, but there are no studies available that directly compare outcomes in these 2 cohorts of patients.11,12
From a functional perspective, each of the study patients was able to produce an adequate signal (10 mV minimum) from PL muscle contraction to drive myoelectric prosthetic control. Additionally, all but one patient reported regular use of a myoelectric prosthesis. There was one patient who refrained due to lack of interest and social barriers. These findings are promising and provide additional support for the use of PL as a potential target in forearm TMR and its role in controlling a myoelectric prosthesis.
There are several limitations to this study. First, while we observed a consistent trajectory of the nerve to the PL, we cannot state with certainty that there are no further anatomic variants in existence. The second limitation is, the PL is absent anywhere from 2.5% to 30% of the population, which precludes these patients as candidates for this procedure. Finally, TMR to the PL is a very rare procedure, and while the clinical outcomes in this study are favorable, there is no comparison group nor a large enough cohort of patients to conclude statistical or clinical significance of our findings. Additionally, preoperative patient-reported outcomes were not available in this cohort to compare against those recorded at final patient follow-up.
Conclusions
Forearm level TMR following transradial amputation provides both symptomatic and functional benefits for patients. This study serves 3 purposes, it provides a consistent anatomic relationship to help surgeons identify the motor nerve to the PL, it demonstrates the efficacy of using PL for control of a myoelectric prostheses, and it provides anecdotal evidence that using PL as one of the targets in forearm TMR can yield acceptable clinical outcomes.
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.H. and M.D. declare that they have no relevant disclosures. E.M. has received consulting fees from Axogen and IP royalties from NewClip Technics. D.N.D. has consulting fees from Axogen and Exosmed. B.L. has received consulting fees from Hanger Clinic and is a paid speaker for Hanger Clinic, he is also a paid consultant and paid presenter or speaker for Checkpoint Surgical. G.G. has received royalties and consulting fees from Biomet, consulting fees from BME, Hanger Clinic, Integra, Restor3d, and Stryker; was a paid presenter or speaker for DePuy, Endo Pharmaceutical, Integra, and Zimmer; is a member of the American Association for Hand Surgery and American Society for Surgery of the Hand, is also on the editorial board of Journal of Hand Surgery.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.