
Abstract
Background:
Infection following surgical fixation of a distal radius fracture can markedly compromise a patient’s functional outcome. This study aimed to compare infection rates in pediatric (5-14 years) and adolescent (15-17 years) patients undergoing fixation of a distal radius fracture to a cohort of young adult (18-30 years) patients.
Methods:
A matched retrospective study was performed using PearlDiver to determine the rates of postoperative infection following distal radius fixation. χ2 and logistic regression were used to assess differences in rates, while linear regression was used to analyze rates of infection over time.
Results:
In 32 368 patients, young adults experienced postoperative infection at a significantly increased rate (odds ratio [OR] = 1.81; 95% confidence interval [CI], 1.45-2.27). This trend was consistent among the male (OR = 1.96; 1.49-2.57) and female (OR = 2.11, 1.37-3.27) cohorts. In the multivariate model, the adult cohort remained at increased risk (OR = 1.40; 95% CI, 1.04-1.89), with open fracture (OR = 4.99; 3.55-6.87), smoking (OR = 1.76; 1.22-2.48), hypertension (OR = 1.69; 1.20-2.33), and obesity (OR = 1.37; 1.02, 1.80) identified as other significant risk factors. There was no significant change in the rate of postoperative infections over the 11-year study period.
Conclusion:
This study demonstrated that although surgical site infections following distal radius fixation are low in patients aged 30 years or younger (0.97%), young adults develop infections at a significantly increased rate. This is important for surgeons to recognize when counseling patients on the risks of surgical fixation.
Keywords
Introduction
Distal radius fractures are among the most common orthopedic injuries encountered by surgeons, with incidence estimates as high as 162 to 270 injuries per 100 000 person-years within the general population.1,2 Within the pediatric population specifically, distal radius fractures account for nearly 25% of all experienced fractures. 3 Fractures to the hand and wrist, depending on severity, can lead to permanent loss of function and even psychological trauma as these patients often lose the ability to participate in various formative experiences such as educational and recreational activities. 4 In pediatric and young adult patients, surgical management via open reduction internal fixation or closed reduction percutaneous fixation is an effective method of treatment used to decrease the morbidity associated with fractures in unacceptable alignment for nonoperative management, helping to prevent malunion and nonunion. 5
These operations, like all surgical treatments, pose the risk of postoperative infection, a serious complication associated with high patient morbidity and health care costs. 6 A recent study demonstrated that the average cost of the surgical management of a distal radius fracture is $6383 ± $13 903. However, when the same procedure is complicated by a postoperative infection, the average total cost of the operation balloons to $23 355 ± $40 412. 7 These infections not only lead to worse patient outcomes but are also a significant financial burden on health care systems.8,9
Postoperative infections have been well described in adult and elderly patients following procedures such as anterior cruciate ligament reconstruction and joint arthroplasty, but less so among the pediatric and adolescent populations, especially in distal radius fracture repair.10 -12 In a recently published study, Constantine et al 7 reported that age above 65 was associated with decreased rates of postoperative infection following distal radius fracture fixation. While the Constantine study did include pediatric patients in the analysis, there was no discussion about the difference in rates of infection among the pediatric population compared with the adult population. Postoperative infections, especially in the pediatric population, often lead to prolonged periods of immobilization, limiting their participation in important formative activities in childhood. A better understanding of the infection risk in these younger populations can help limit the consequences of these complications in patients navigating their developmental years. Hence, this study seeks to build on the aforementioned study to determine risk factors and compare the rates of postoperative infection following distal radius fracture fixation among patients of pediatric and adolescent age (5-17 years) with those of young adult age (18-30 years).
Methods
Data Source
The Mariner data set within PearlDiver (PearlDiver Technologies) was queried to perform a retrospective cohort analysis over an 11-year period. This data set is generated using all insurance claims made through Humana Inc., which includes more than 120 million different patients and their respective insurance claims from 2010 through 2020. This provides researchers the means to longitudinally track patients and their care, including procedures, medications, medical diagnoses, emergency department visits, and more. However, to ensure patient privacy, all groups with 10 patients or fewer were not reported by the database and therefore were reported as <11 in this study. The data set was used in this study to compare the rates of postoperative infection within 6 months following surgical fixation of distal radius fracture among pediatric and young adult cohorts.
Identifying Distal Radius Fracture Fixation and Generating Cohorts
The MUExtr subset within Mariner, which contains all patients who have made an insurance claim for an upper extremity complaint, was queried for all patients who filled a claim for surgical fixation of a distal radius fracture from 2010 to 2020. This was performed using Current Procedural Terminology (CPT) codes 25606 (closed reduction and percutaneous pinning [CRPP]) and 25607 through 25609 (open reduction internal fixation [ORIF]). To ensure full medical records, only patients who were active within the database for 30 days before the operation and 180 days after the operation were included in the study. Only patients aged 5 to 30 years were included. Patients aged 5 to 17 years were combined into the pediatric/adolescent cohort. This group was subdivided into 5 to 14 years (pediatric) and 15 to 17 years (adolescent). Patients between 18 and 30 years were combined into an adult cohort. 13 Each group was also divided into male- and female-specific cohorts for continued analysis.
Identifying Postoperative Infection
Using the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10), all patients within each cohort who made an insurance claim for a postoperative infection complication were identified. All included ICD-9 and ICD-10 codes can be seen in Supplemental Table 1. Only those infections that occurred within 180 days of the operation were included in the analysis to better ensure the infection was truly associated with the operation. The CPT codes 10180, 25028, 25031, 29840, 29843, 29844, 29845, and 29846 were used to determine the rate of postoperative infection that required surgical intervention.
Statistical Analysis
To compare the rates of postoperative infection following surgical repair of a distal radius fracture between the pediatric/adolescent and young adult populations, χ2 analysis was performed. Multivariate logistic regression was used to determine the influence of age group on rates of infection while controlling for sex, fixation strategy (CRPP vs ORIF) performed on the patient, the type of fracture (open vs closed), tobacco use within a year prior to surgery, diabetes, obesity (body mass index [BMI] >30 kg/m2), lung disease, chronic kidney disease (CKD), and hypertension. Linear regression was used to assess for significant changes in the rates of postoperative infection among the overall cohort and the male- and female-specific cohorts. Odds ratios (OR) and 95% confidence intervals (CIs) were reported for each comparison. A cutoff of P < .05 was used to assess for statistical significance. All analyses were done using the embedded R Statistical Package within PearlDiver.
Results
The query of the Mariner data set within PearlDiver returned 32 368 patients between the ages of 5 and 30 years who made an insurance claim for surgical fixation of a distal radius fracture. Of the 32 368 patients, 15 058 patients were between the ages of 5 and 14 years (pediatric group), 4244 patients were between the ages of 15 and 17 years (adolescent group), and 13 066 patients were between the ages of 18 and 30 years (adult group), and most of the patients were men (19 962). Table 1 shows the number of patients in each age group broken down by fixation strategy (CRPP vs ORIF).
Number of Patients in Each Age Group Broken Down by Fixation Strategy.
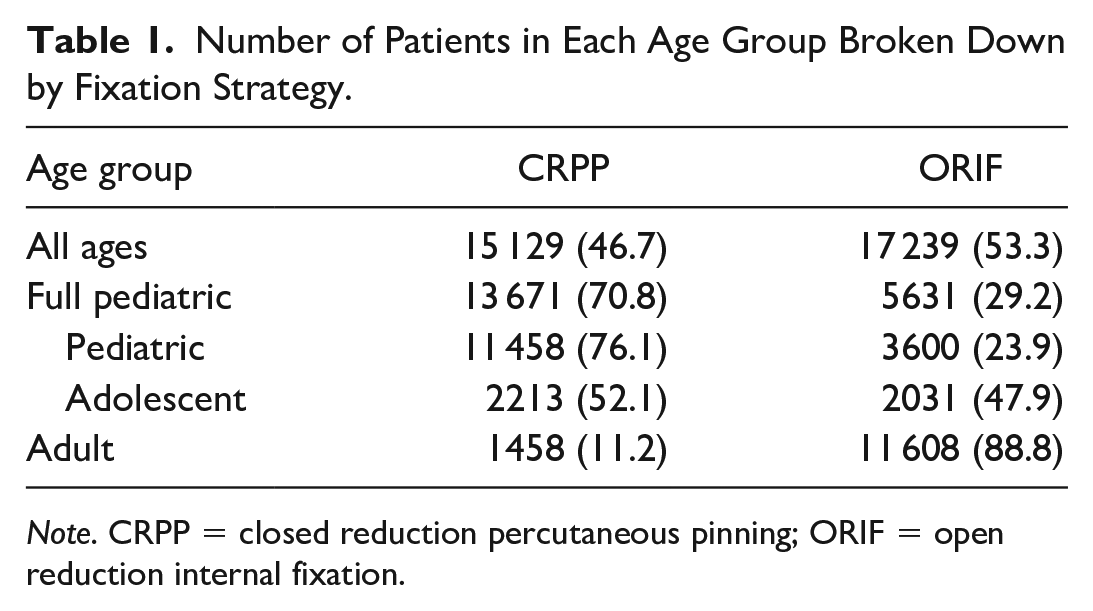
Note. CRPP = closed reduction percutaneous pinning; ORIF = open reduction internal fixation.
The overall rate of infection within the full population was 0.97% (313/32 368). Of the 313 postoperative infections, 15 required surgical debridement (4.8%). The rate significantly differed among the pediatric, adolescent, and adult subgroups. In the binary analysis, adult patients who underwent surgical fixation of a distal radius fracture were 86% more likely to experience postoperative infection compared with the adolescent subgroup (OR = 1.86; 95% CI, 1.27-2.77). This difference was also seen within the male subcohort, where adult male patients were 130% more likely to experience infection compared with the adolescent male subgroup (OR = 2.30; 95% CI, 1.47-3.60). There was no difference seen between the pediatric subgroup and the adolescent subgroup (Table 2). There was also no difference between the rates of infection in the female adult and pediatric groups compared with the female adolescent group.
Rates of Postoperative Infection Within the Pediatric (5-14 Years), Adolescent (15-17 Years), and Adult (18-30 Years) Cohorts and a Comparison Between the 3 Cohorts Using χ2 Analysis.
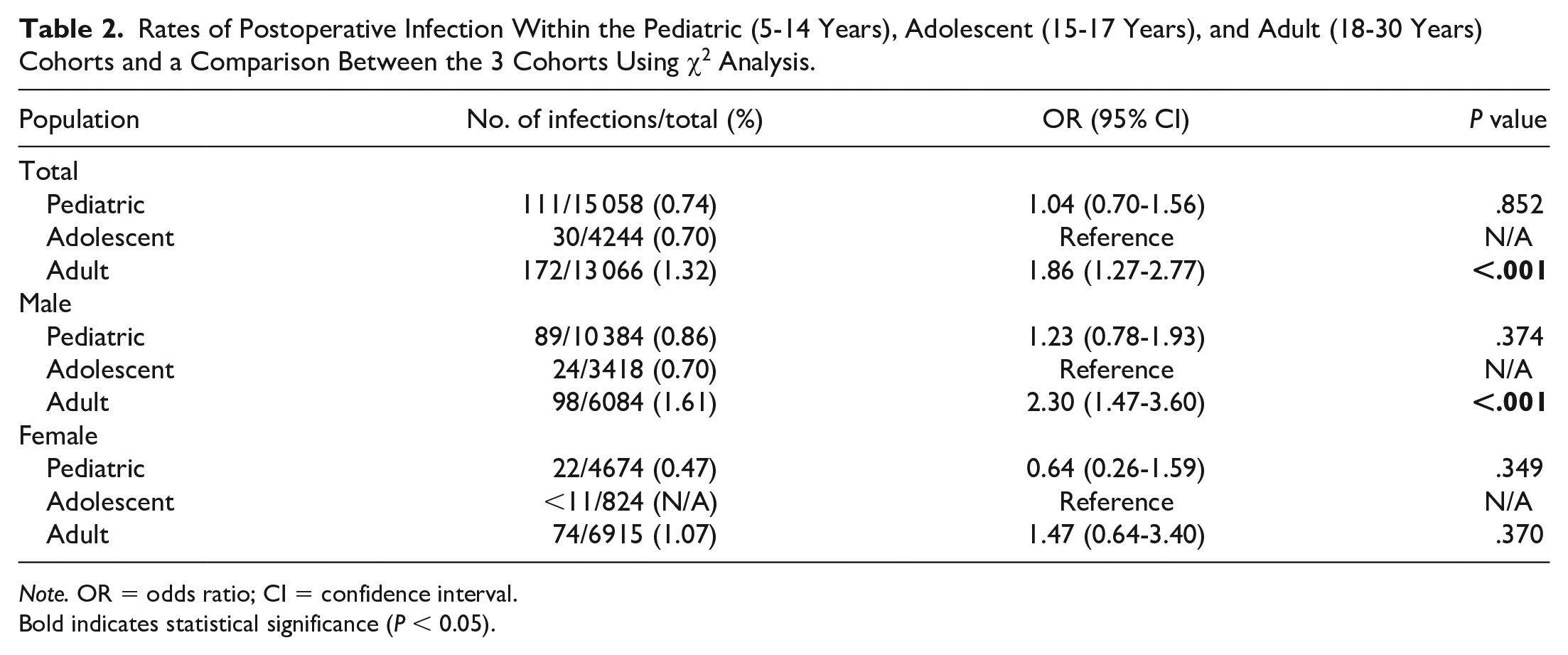
Note. OR = odds ratio; CI = confidence interval.
Bold indicates statistical significance (P < 0.05).
The same analysis was conducted between a combined pediatric/adolescent subgroup that contained all patients aged 5 to 17 years and the adult group (Table 3). The combined analysis demonstrated a significantly increased rate of infection among young adult patients in the full cohort (OR = 1.81; 95% CI, 1.45-2.27), male-specific cohort (OR = 1.96; 95% CI, 1.49-2.57), and female-specific cohort (OR = 2.11; 95% CI, 1.37-3.27). Adult patients also underwent surgical debridement to address a surgical site infection more often than their pediatric counterparts (P = .006) (Table 4). χ2 analysis comparing surgical site infection rates between men and women also revealed a significant difference. Male patients in all age categories aside from the adolescent cohort experienced increased rates of surgical site infection (Table 5).
Rates of Postoperative Infection Within the Full Pediatric/Adolescent (5-17) Cohort and the Adult (18-30 Years) Cohort and a Comparison Using χ2 Analysis.
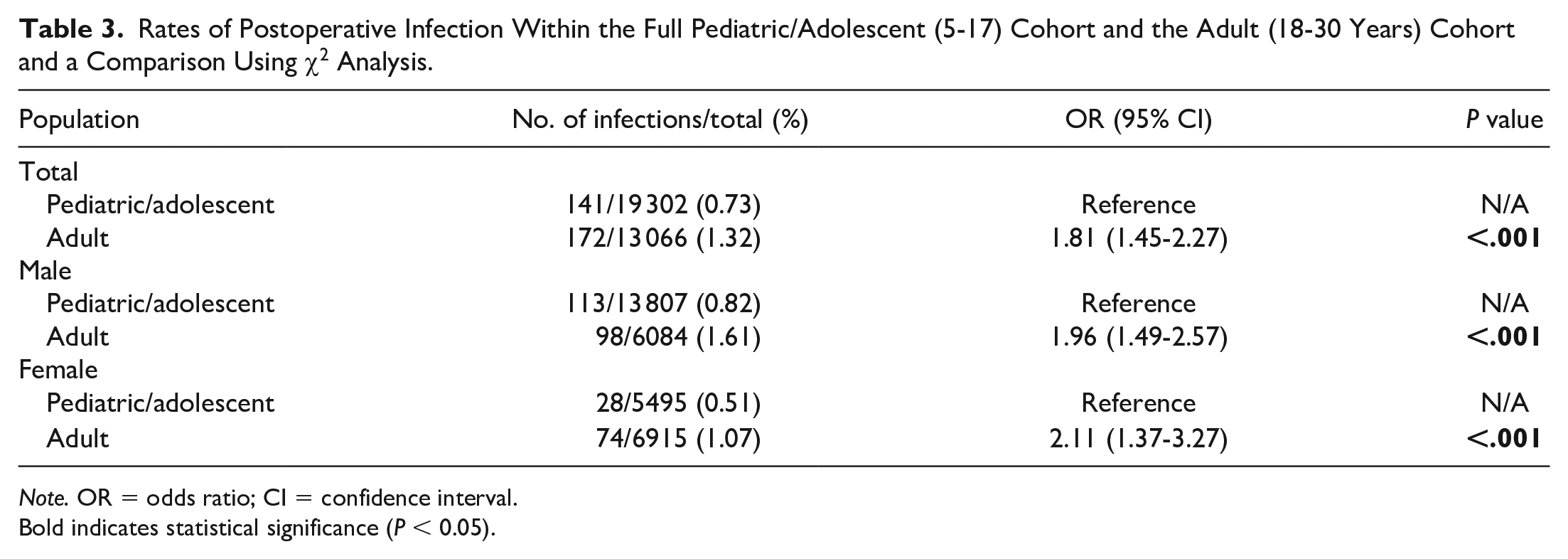
Note. OR = odds ratio; CI = confidence interval.
Bold indicates statistical significance (P < 0.05).
Rates of Postoperative Infection Requiring Surgical Debridement Within the Full Pediatric/Adolescent (5-17) Cohort and the Adult (18-30) Cohort and a Comparison Using χ2 Analysis.
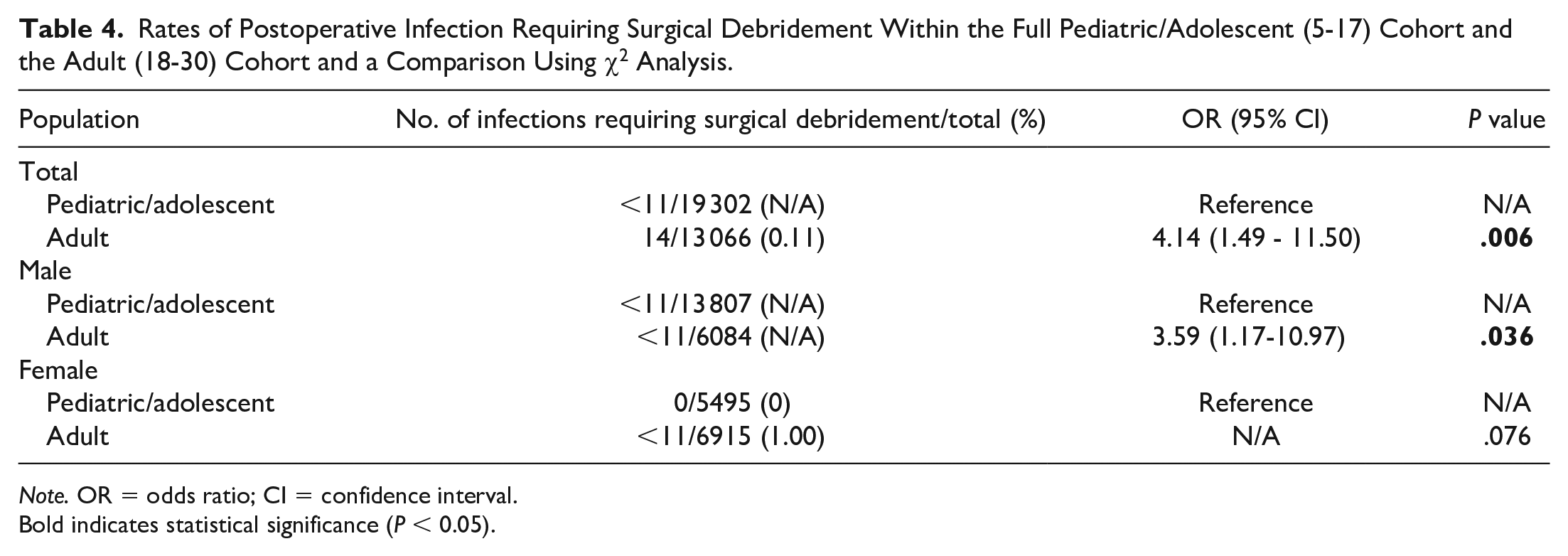
Note. OR = odds ratio; CI = confidence interval.
Bold indicates statistical significance (P < 0.05).
Age-Constant Comparison of the Rates of Postoperative Infection in Men and Women.
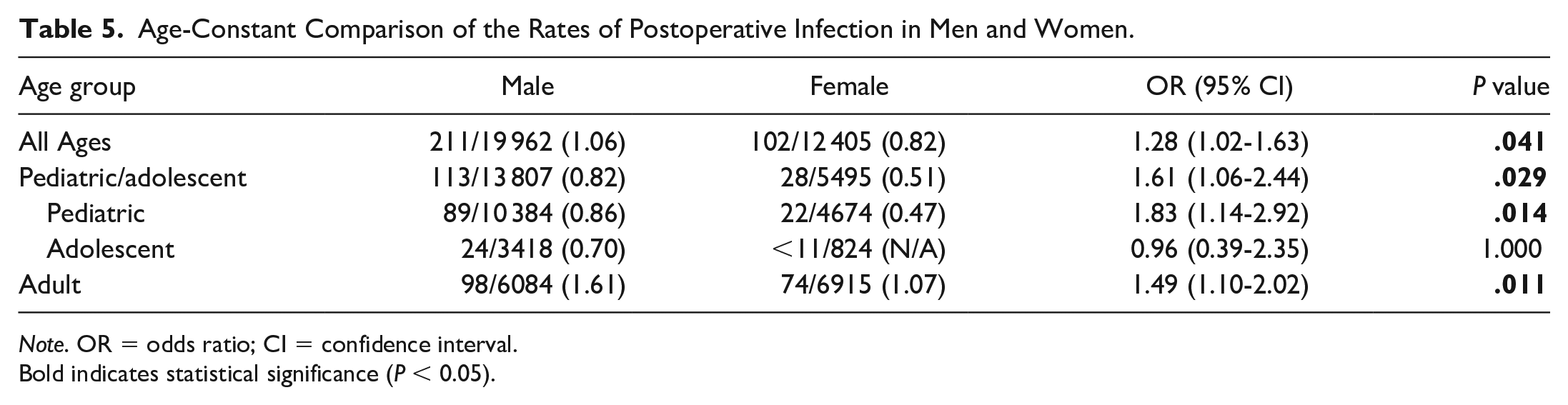
Note. OR = odds ratio; CI = confidence interval.
Bold indicates statistical significance (P < 0.05).
χ2 analysis comparing the type of operation used to address the distal radius fracture demonstrated that the pediatric population was significantly more likely to undergo percutaneous fixation (CPT-25606) compared with ORIF (CPT-25607, CPT-25608, CPT-25609) (P < .001). The multivariate logistic regression model demonstrated that within these 2 populations, percutaneous fixation was not associated with an increased or decreased rate of postoperative infection. Young adult age (compared with pediatric age), smoking, the presence of an open fracture, hypertension, and obesity were significant predictors of postoperative surgical site infection following distal radius fixation (Table 6).
Multivariate Logistic Regression Demonstrating Significant Risk Factors of Postoperative Infection in the Pediatric and Young Adult Population.
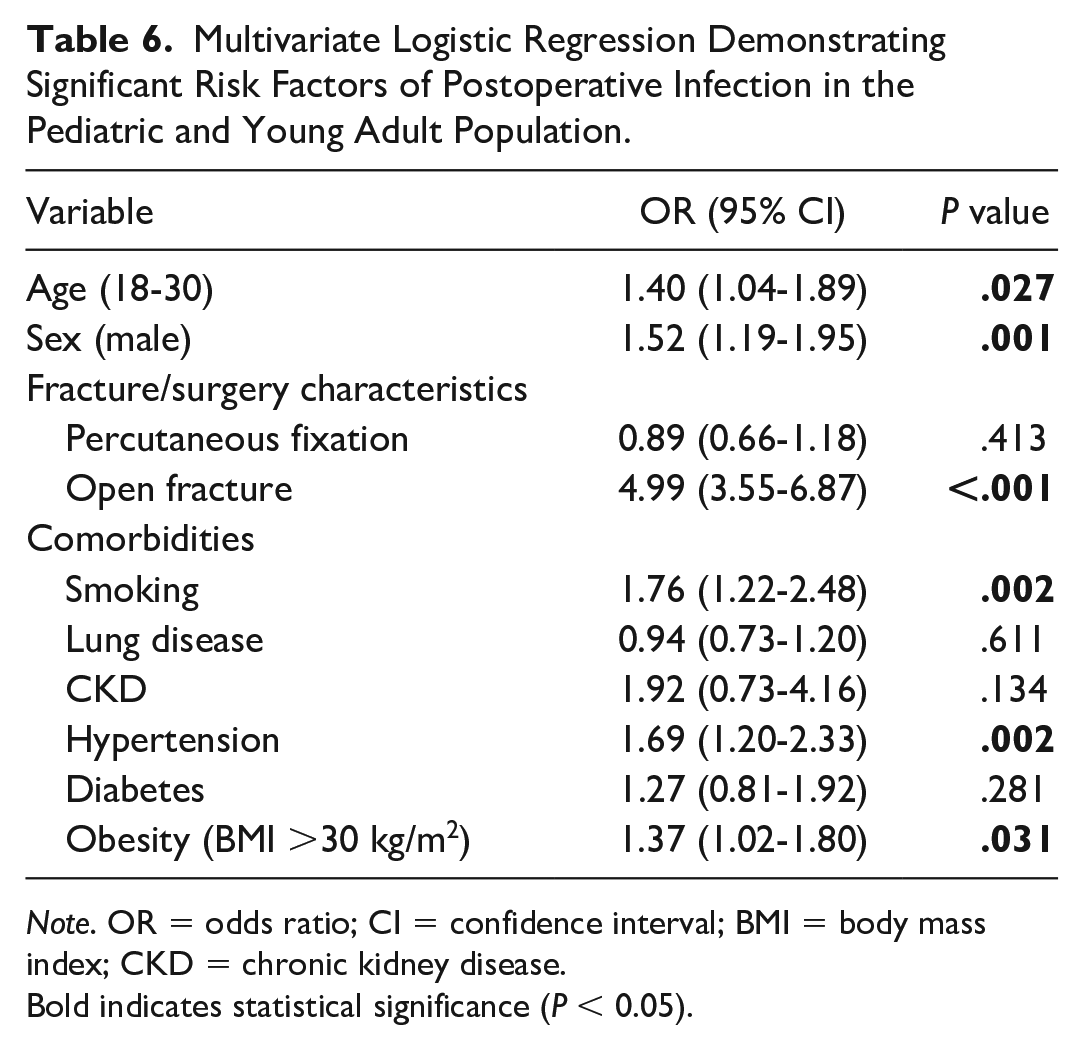
Note. OR = odds ratio; CI = confidence interval; BMI = body mass index; CKD = chronic kidney disease.
Bold indicates statistical significance (P < 0.05).
Regarding changes in the infection rates over time, linear regression analysis demonstrated no change in postoperative infection rate following fixation of a distal radius fracture over the study period for the overall cohort, the male-specific cohort, and the female-specific cohort (Figure 1).
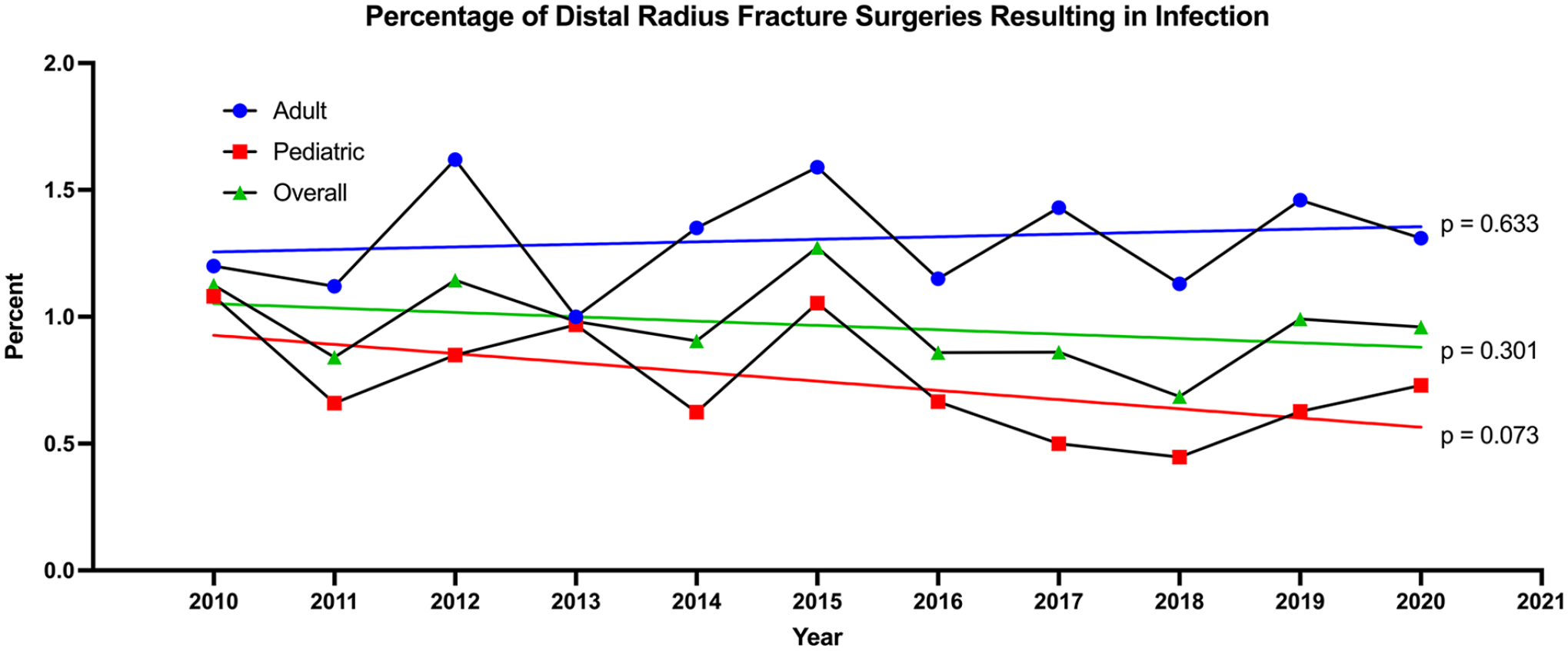
Trends in the rates of postoperative infection following surgical repair of distal radius fractures between 2010 and 2020. Linear regression trend lines are included for each set of data.
Discussion
The purpose of this study was to continue investigations regarding the relationship between age and postoperative infection following fixation of distal radius fractures. 7 The rate of surgical site infection in the pediatric, adolescent, and young adult combined population was 0.97%, comparable to the rate reported by Constantine et al (0.90%) in older patients. Separately, the rate of infection in young adults was 1.32%, compared with 0.73% in the pediatric/adolescent population. In a binary analysis, this difference was significant (P < .001), with young adults (81%) more likely to be diagnosed with an infection. The largest difference in rates was seen in male young adult patients as they were 130% more likely to experience postoperative infection compared with the male pediatric/adolescent cohort. This pattern was not seen between the male adolescent and male pediatric groups. In addition, no significant difference in infection rates was seen across any of the female subgroups or the young adult and pediatric/adolescent age groups using a multivariate logistic regression to control for confounders.
Previous studies have examined risk factors for developing postoperative infections irrespective of the age group. Comorbidities such as diabetes mellitus, obesity, hypertension, lung disease, kidney disease, and smoking have been identified in prior studies as risk factors for postoperative infection following various types of surgeries.14 -19 Preoperative risk stratification in orthopedic procedures allows surgeons to identify patients at higher risk of perioperative and postoperative complications and subsequently use different injury management or safety precautions for those patients to help reduce complication rates.20,21 In addition, age may also be a relevant risk factor in the development of postoperative infections, as highlighted by both the present study and Constantine et al.
Both tobacco use and obesity have been demonstrated to significantly increase the risk of postoperative infection following distal radius fracture fixation in the young population. Tobacco has been linked with impaired wound healing, specifically by decreasing fibroblast migration, collagen synthesis, and vascular oxygen tension. 22 As a result, smoking was found to be associated with a 51% increase in postoperative infections. 23 Young adults, aged 18 to 25 years specifically, have the highest incidence of smoking behaviors of all ages. 24 This magnitude of smokers likely influences the significance of smoking on postoperative infection in distal radius fracture fixation. In contrast, the idea of obesity as a primary factor of postoperative infection is controversial. Multiple studies on increasing BMI and infection in upper extremity surgery found a nonsignificant increase in infection risk.25,26 However, a meta-analysis by Yuan and Chen demonstrated that patients with a BMI ≥30 kg/m2 were 91% more likely to experience surgical site infections. 27 Interestingly, Ebinger et al 15 found that obese patients were more likely to experience complex distal radius fractures demanding more invasive surgical techniques that may predispose these patients to infection. This likely means the true relationship between obesity and postoperative infection, specifically following distal radius fixation, is complex and multifaceted.
Several studies have described how other comorbidities, such as diabetes mellitus and CKD, place patients at increased risk of postoperative infection.17 -19 One systematic review found that patients with diabetes are at an increased risk of surgical site infections (OR = 1.53) compared with those without diabetes. 17 Similarly, CKD has been shown to delay wound healing and predispose patients to postoperative complications, both in a murine model and in a propensity-matched cohort analysis.18,19 However, neither diabetes nor CKD was a significant predictor of postoperative infection in this analysis of patients aged 5 to 30 years. Although it is not exceedingly rare for young populations to develop chronic conditions such as diabetes and CKD, the prevalence of these conditions likely has not progressed to a point that could influence the rate of postoperative infection following distal radius fixation. 28 However, as the prevalence of early-onset chronic conditions increases, comorbid diseases such as diabetes in these age cohorts may begin to influence the rate of postoperative infections to a greater extent. 29
Ultimately, the strongest identified predictor of postoperative infection in this study was the presence of an open fracture, increasing the infection risk nearly 5-fold (OR = 4.99). This is nearly double the OR (2.54) reported by Constantine et al, 7 indicating that open fractures in the younger population have an even greater influence on infection. Multiple studies evaluating a range of injuries, including distal femur fractures, tibial plateau fractures, and upper extremity fractures, consistently found open fractures to be an independent risk factor for infection after operative fixation.30 -33 Open wounds increase the likelihood of wound contamination; therefore, current practice guidelines recommend early systemic antibiotic administration as a prophylactic measure. 34 Conversely, operative technique did not influence the rate of infection in our population. Two recent meta-analyses by Anderson et al 35 and Zong et al 36 found percutaneous pinning to be associated with an increased rate of superficial infection when compared with ORIF with volar plating. Furthermore, Constantine et al described a similar relationship regarding treatment technique. Our results, however, do not align with these findings, possibly due to our focused sample size potentially biasing the strength of this association. Alternatively, the protoplasm of younger individuals, who likely have fewer comorbidities, may reduce the burden of infections related to percutaneous pinning, where pins left outside of the body are predisposed to developing infections.
As with many retrospective database studies, this study has several limitations. Although PearlDiver contains health records of more than 100 million patients, this is not a random sample and only includes insured patients, and is therefore subjected to potential sampling bias. This study also depended on ICD and CPT billing codes to isolate specific diagnoses and procedures. As a result, there is the possibility of miscoding. However, as the sample size was greater than 30 000, we believe this limitation to have minimal impact on the overall results of the study. Understanding the true nature and severity of each fracture is also impossible through a database study, and as the nature of each injury changes management, the inability to properly assess each injury does limit the general applicability of the study. Finally, due to the small rate of infection, it is not possible to differentiate between superficial, deep, and pin site infections as PearlDiver does not give specific values when populations are less than 11 patients.
Conclusion
In conclusion, this study based on insurance data of 19 302 pediatric/adolescent patients found the postoperative infection rate for distal radius fixation to be 0.73%. We found this population to be at a significantly decreased risk of infection compared with young adults. However, there was no difference in infection rates between the pediatric and adolescent subgroups. Pediatric and young adult men were at an increased risk of infection compared with their female counterparts, with no sex difference seen among adolescents. In addition, open fractures, smoking, hypertension, and obesity were significant risk factors for infection among patients aged 5 to 30 years. This study provides a reference rate of infection following pediatric and adolescent distal radius fixation along with several associated risk factors that may be clinically useful to the practicing upper extremity surgeon.
Supplemental Material
sj-docx-1-han-10.1177_15589447221142896 – Supplemental material for A Comparison of the Rates of Postoperative Infection Following Distal Radius Fixation Between Pediatric and Young Adult Populations: An Analysis of 32 368 Patients
Supplemental material, sj-docx-1-han-10.1177_15589447221142896 for A Comparison of the Rates of Postoperative Infection Following Distal Radius Fixation Between Pediatric and Young Adult Populations: An Analysis of 32 368 Patients by J. Alex Albright, Ozair Meghani, Elliott Rebello, Omar Karim, Edward J. Testa, Alan H. Daniels and Aristides I. Cruz in HAND
Footnotes
Ethical Approval
This study did not require review by our institutional review board.
Statement of Human and Animal Rights
There were no violations of human or animal rights throughout the duration of the work conducted for this study.
Statement of Informed Consent
This study used a de-identified data set and did not require patient informed consent.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.A.A., O.M., E.R., O.K., and E.J.T. do not report any disclosures. A.H.D. reports disclosures as follows: EOS, paid consultant; Orthofix, Inc., paid consultant, research support; SpineArt, paid consultant; Medtronic/Medicrea, paid consultant; Springer: publishing royalties, financial or material support; Stryker: paid consultant, all outside submitted work. A.I.C. reports disclosures as follows: POSNA, committee board member, PRiSM, committee board member.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.