
Abstract
Background:
Extensor carpi ulnaris (ECU) subsheath injuries are an increasingly recognized cause of ulnar-sided wrist pain in elite athletes. There is a lack of surgical outcome data in elite athletes, and unique considerations exist for these patients.
Methods:
We performed a retrospective review of our hand center experience of 14 elite professional or collegiate athletes who prospectively underwent radially based extensor retinacular sling ECU subsheath reconstruction by 3 hand surgery-fellowship-trained surgeons between April 2011 and April 2021. Clinical, magnetic resonance imaging (MRI), and intraoperative findings were cataloged. Subgroup analyses of elite hockey players and acute subsheath injuries were also conducted. Statistical analysis was performed via a 2-tailed paired t test.
Results:
Mean age at the time of surgery was 21.3 years (range, 18-34). Mean time from symptom onset to surgery was 102.1 ± 110.7 days. All 14 patients underwent preoperative MRI. Five patients (35.7%) had intrinsic ECU tendinopathy, 9 patients (64.3%) had ECU tenosynovitis, 6 patients (42.9%) had triangular fibrocartilage complex tears, and 9 patients (64.3%) had ulnocarpal synovitis. Mean postoperative pain on a Visual Analog Scale was 0.25 ± 0.43. Grip strength (P = .001), wrist flexion-extension (P = .037), and pronosupination arcs (P = .093) showed excellent recovery postoperatively. Mean time to unrestricted return to sports was 92.5 ± 21.0 days. There were no complications. Subgroup analyses found similar functional improvement and characterized injury patterns.
Conclusions:
Overall, our findings suggest surgical management of ECU subsheath injuries is a viable option in both acute and chronic settings in elite athletes and may be favorable compared with nonoperative management.
Introduction
Extensor carpi ulnaris (ECU) subsheath injuries are increasingly recognized as an etiology of ulnar-sided wrist pain, especially in elite stick and racquet athletes. The ECU tendon is stabilized within the sixth dorsal compartment by its own fibro-osseous cartilaginous subsheath along the distal ulna deep to the overlying extensor retinaculum (ER).1,2 Subsheath insufficiency with or without frank ECU tendon instability often presents concurrently with intrinsic ECU tendon pathology and other ulnocarpal compartment injuries (such as triangular fibrocartilage complex [TFCC] and/or lunotriquetral interosseous ligament injuries). The coincidence of these injuries is rooted in the ECU “system” concept outlined by Graham 3 and further emphasizes the importance of identifying treatment options that can simultaneously address concomitant pathologies contributing to symptoms and dysfunction. While 2 different classification systems, the Inoue and Tamura 4 classification and the Allende and Le Viet 5 classification (Figure 1), have been developed to describe various subsheath injuries, treatment of these injuries in the athletic population is predicated on multiple variables, including sport, position, hand dominance, and timing within the season.
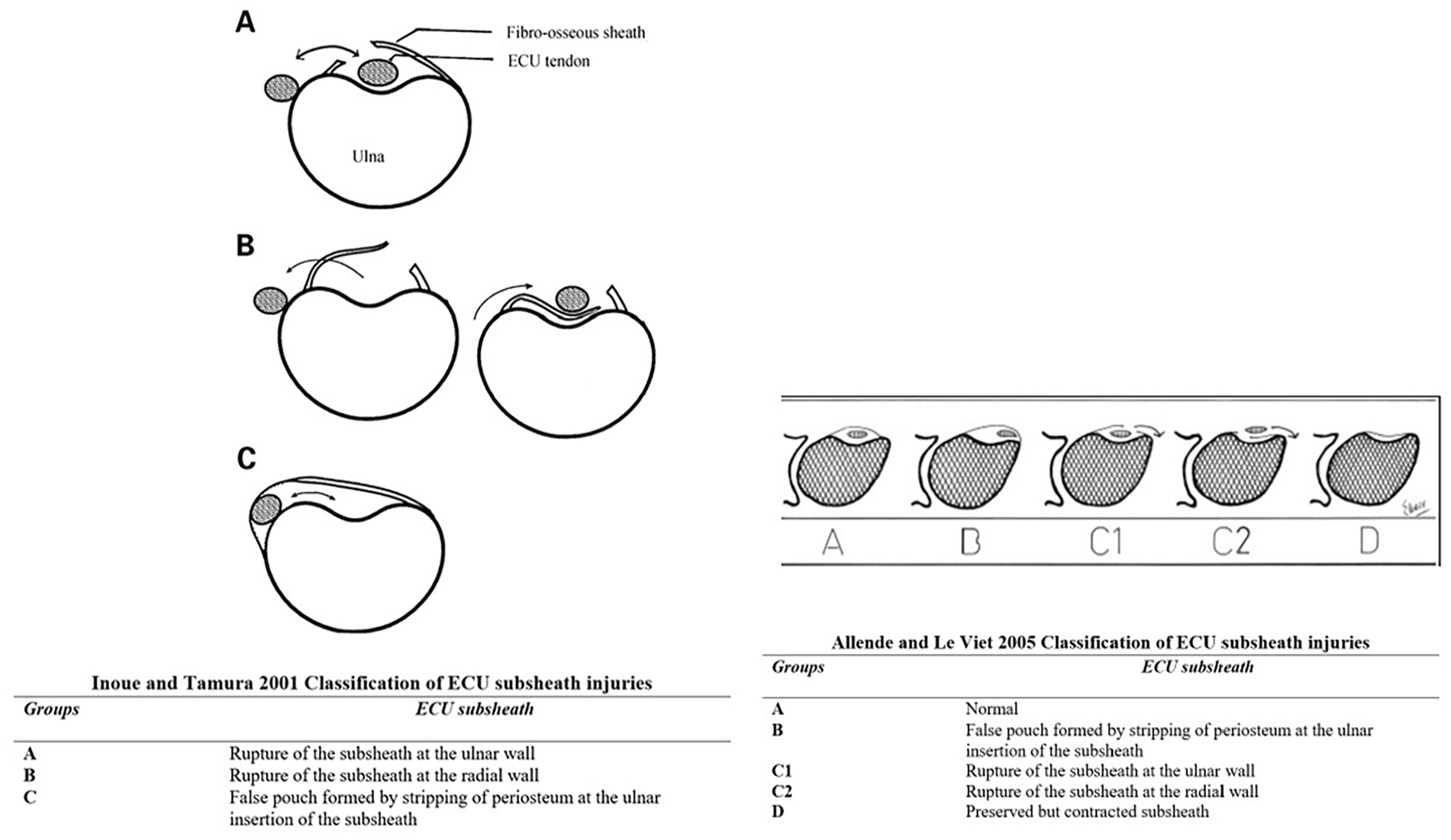
The Inoue and Tamura 2001 classification and the Allende and Le Viet 2005 classification of ECU subsheath tears.
Maximal biomechanical stress and rupture of the ECU tendon subsheath is most commonly a result of forceful hypersupination, flexion, and ulnar deviation of the wrist. 6 This often results in frank instability and painful ECU snapping with subluxation of the tendon outside the distal ulnar groove and linea jugata, and/or apprehension with dynamic stress examination.2,7 -9 In tennis, acute traumatic ECU subsheath injuries often occur from a 2-handed backhand stroke, as the dominant hand moves forcefully and rapidly from pronation to supination to impart spin on the tennis ball, 10 whereas in golf, traumatic injuries typically occur to the leading wrist. 9 Hockey players are also very susceptible to ECU injuries, with the leading bottom wrist most at risk during shooting with wrist supination and flexion, although top-handed subsheath injuries can occur as well.
Previous studies have highlighted the increasing incidence of ECU tendon and subsheath injuries in stick athletes, namely in tennis and golf.10 -12 Montalvan et al 11 described their case series of professional tennis players treated nonoperatively; 42% demonstrated ECU instability and 50% had tenosynovitis or tendinopathy. Other stick athletes such as hockey and baseball players are also at high risk of ECU subsheath injuries, although they are currently not well represented in the literature. One case report by Tomori et al 13 highlighted the treatment course of a competitive hockey player, who also suffered an acute traumatic TFCC injury in addition to an ECU subsheath injury.
Acute ECU subsheath injuries can often be treated successfully with nonoperative management, including nonsteroidal anti-inflammatory drugs and immobilization with or without steroid injections.1,9,14 In recalcitrant cases requiring surgical intervention, there remains a lack of outcome data despite the variety of described operative techniques,1,6,9,14 -17 especially in elite athletes. Additional prospective outcome data are needed to further elucidate optimal treatment approaches in elite athletes as there are unique considerations in these patients regarding return to play. A radially based ER sling method was previously described to treat ECU subsheath insufficiency, but without any described outcomes.18 -20 We believe this approach to ECU subsheath reconstruction is effective at improving function and allows for simultaneous treatment of concurrent ulnocarpal compartment injuries while limiting complications such as ECU stenosing tenosynovitis. Our recently accepted case series consisted of both nonathletes and elite athletes undergoing radially based ER sling ECU subsheath reconstruction, examining surgical outcomes and concurrent wrist injuries without stratifying for elite athletes.
In this case series of 14 patients, we demonstrate that the radially based ER sling is a safe and effective reconstructive strategy to treat both acute and chronic ECU subsheath injuries particularly in elite athletes. In addition, we catalog and characterize the prevalence of concurrent wrist pathologies in elite athletes with ECU subsheath injuries, with specific subgroup analysis of hockey players. We hypothesize that our radially based ER sling approach will result in significant improvement in functional outcomes with minimal complications and expedited return to sport in elite athletes with ECU subsheath injuries.
Materials and Methods
Ethical Approval
Our study was approved by the institutional review board at Newton-Wellesley Hospital. We retrospectively chart reviewed our hand center experience of 14 elite athletes (8 men; 6 women) who prospectively and consecutively underwent a radially based ER sling ECU subsheath reconstruction by 3 hand surgery-fellowship-trained surgeons from April 2010 to April 2021. Seven cases each were performed by 1 surgeon, 5 cases by another, and 2 cases by the final surgeon using an identical surgical technique. There were no exclusion criteria for this study. Independent variables addressed were age, sex, time to presentation/surgery, attempt at conservative management, preoperative imaging, presence of ECU snapping or apprehension with provocation (flexion, hypersupination, and ulnar deviation), and concurrent wrist injuries. Dependent variables addressed were grip strength (in kg), range of motion values such as flexion-extension arc (in degrees) and pronation-supination arc (in degrees), return to sport, and surgical complications.
Patients
Eight men and 6 women with a mean age at surgery of 21.3 years (range, 18-34 years) were included in the study. All 14 patients (100%) were elite professional or collegiate athletes. Eight patients (57.1%) played hockey, 2 lacrosse (14.3%), 1 tennis (7.1%), 1 softball, 1 rowing, and 1 volleyball. Eight patients had surgeries on their dominant wrist, and surgery was performed on the right wrist in 6 (42.9%) patients and the left wrist in 8 (57.1%) patients.
On examination, there was frank snapping of the ECU in 7 patients (50%), apprehension with ECU provocation in 5 patients (35.7%), and ECU tenderness to palpation in 2 patients (14.3%). Preoperative imaging included magnetic resonance imaging (MRI) in all 14 patients (100%), plain-film radiographs in 8 patients (57.1%), and ultrasound in 3 patients (21.4%). Magnetic resonance imaging findings in chronic ECU subsheath tears are described in Figure 2. All 14 patients (100%) had MRI findings of ECU subsheath injury, while all 6 TFCC tears identified intraoperatively were also seen on MRI. Nine patients (64.3%) were treated conservatively before undergoing surgical intervention, whereas 5 patients (35.7%) with acute injuries (defined as less than 2 weeks) and severe pain elected for early surgical intervention despite being informed of nonoperative treatment options. Nonoperative management included anti-inflammatory medications, forearm immobilization in pronation with the wrist immobilized in a position of extension, and radial deviation for 4 to 6 weeks. For persistent painful snapping of the ECU, the use of cortisone injections to attempt to achieve painless snapping until repair/reconstruction is often attempted, especially for in-season athletes. Seven of the 9 patients treated conservatively also received steroid injections (78%). Surgical treatment was indicated in refractory cases. The mean time from symptom onset to presentation was 31 ± 45.5 days, and the mean time from symptom onset to surgery was 102.1 ± 110.7 days. Wrist arthroscopy was performed on 12 patients (85.7%). The indication for concomitant wrist arthroscopy was foveal tenderness in combination with MRI findings of TFCC pathology (Table 1).
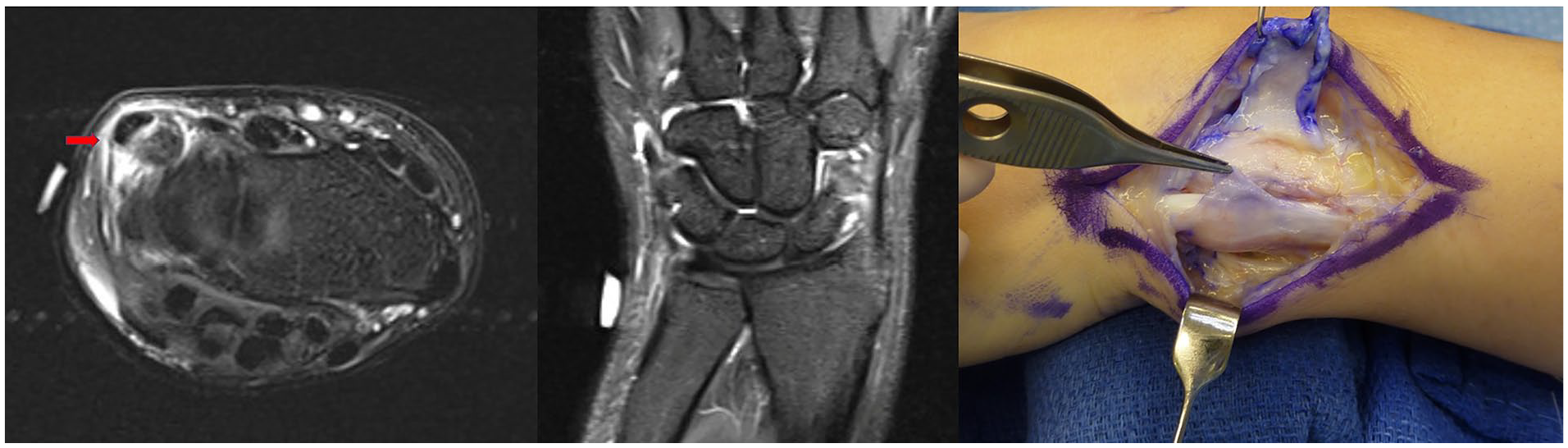
Magnetic resonance imaging and intraoperative findings showing a chronically attenuated Inoue and Tamura type C (Allende and Le Viet type B) extensor carpi ulnaris subsheath injury with concurrent extensor carpi ulnaris tenosynovitis.
Patient Demographics, Clinical Findings, and Surgical Outcomes.
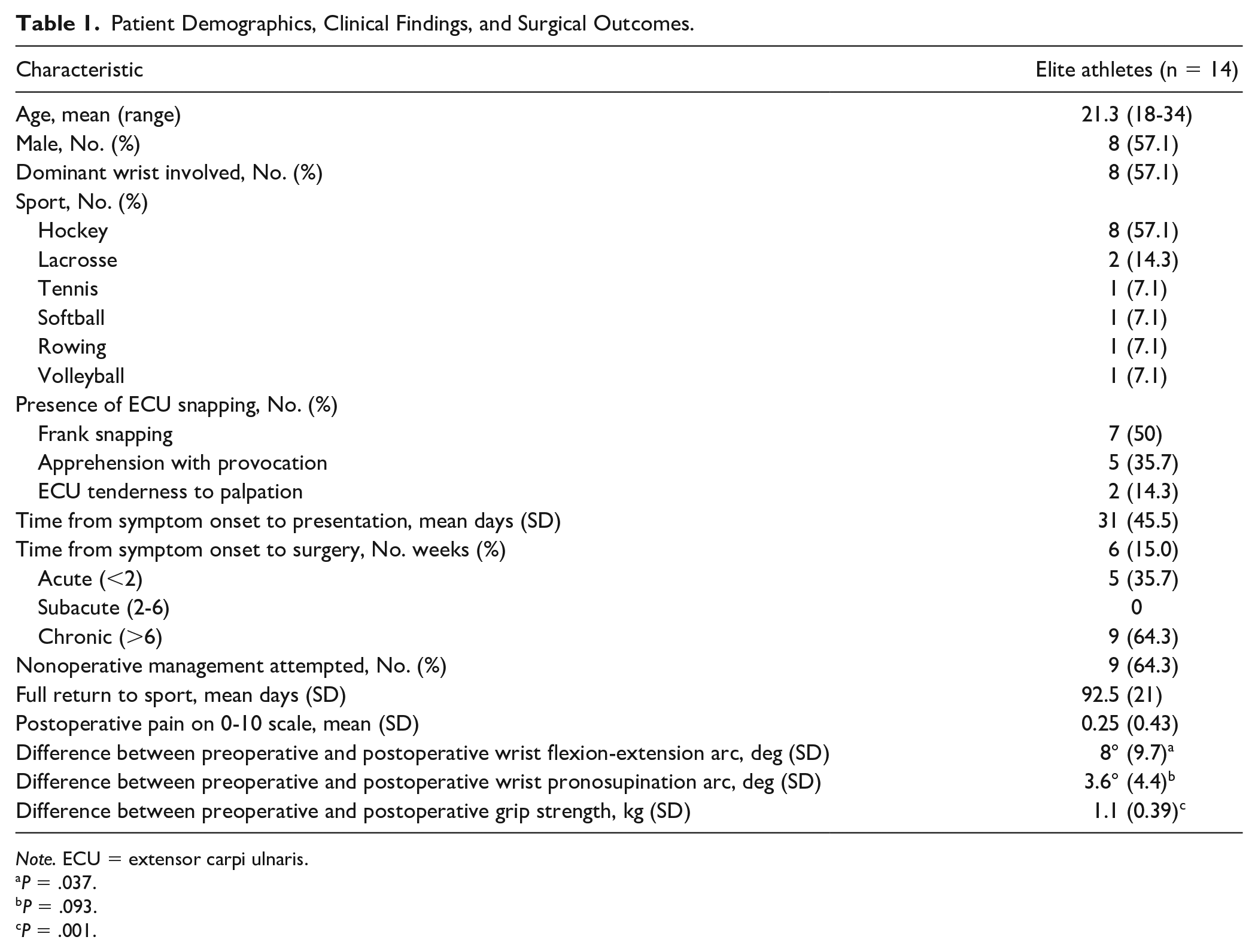
Note. ECU = extensor carpi ulnaris.
P = .037.
P = .093.
P = .001.
Preoperative and postoperative grip strength and wrist range of motion measurements for flexion-extension arc and pronosupination arc were recorded by the hand therapist. Statistical analysis was conducted via a 2-tailed paired t test. Triangular fibrocartilage complex tears were graded according to the Palmer classification, and scapholunate interosseous ligament tears were graded according to the Geissler classification.
Surgical Technique
We previously described our surgical technique.18 -20 A radially based ER sling is designed along the distal portion of the ER (Figure 3). The retinacular flap is elevated as a separate layer from the ECU fibro-osseous sheath to the level of the extensor digiti quinti (EDQ) within the fifth extensor compartment. The underlying ECU subsheath is then inspected. The ECU is translocated dorsal-radial during the nonanatomical sling reconstruction, and then, the native volar-based fibro-osseous subsheath is approximated anatomically to the dorsal periosteum with buried interrupted sutures (3-0 undyed absorbable monofilament). This serves as a smooth interposed bed on which the sling and ECU can glide during pronosupination (Supplemental Figure 1). The ER sling is then passed volar to the ECU and then secured with multiple interrupted 2-0 absorbable monofilament suture to the native retinaculum about the fifth extensor compartment (Figure 3, Supplemental Figure 1). Through a full range of pronosupination, the ECU is confirmed to track smoothly along the dorsal ulna without any snapping or subluxation (Figure 3).
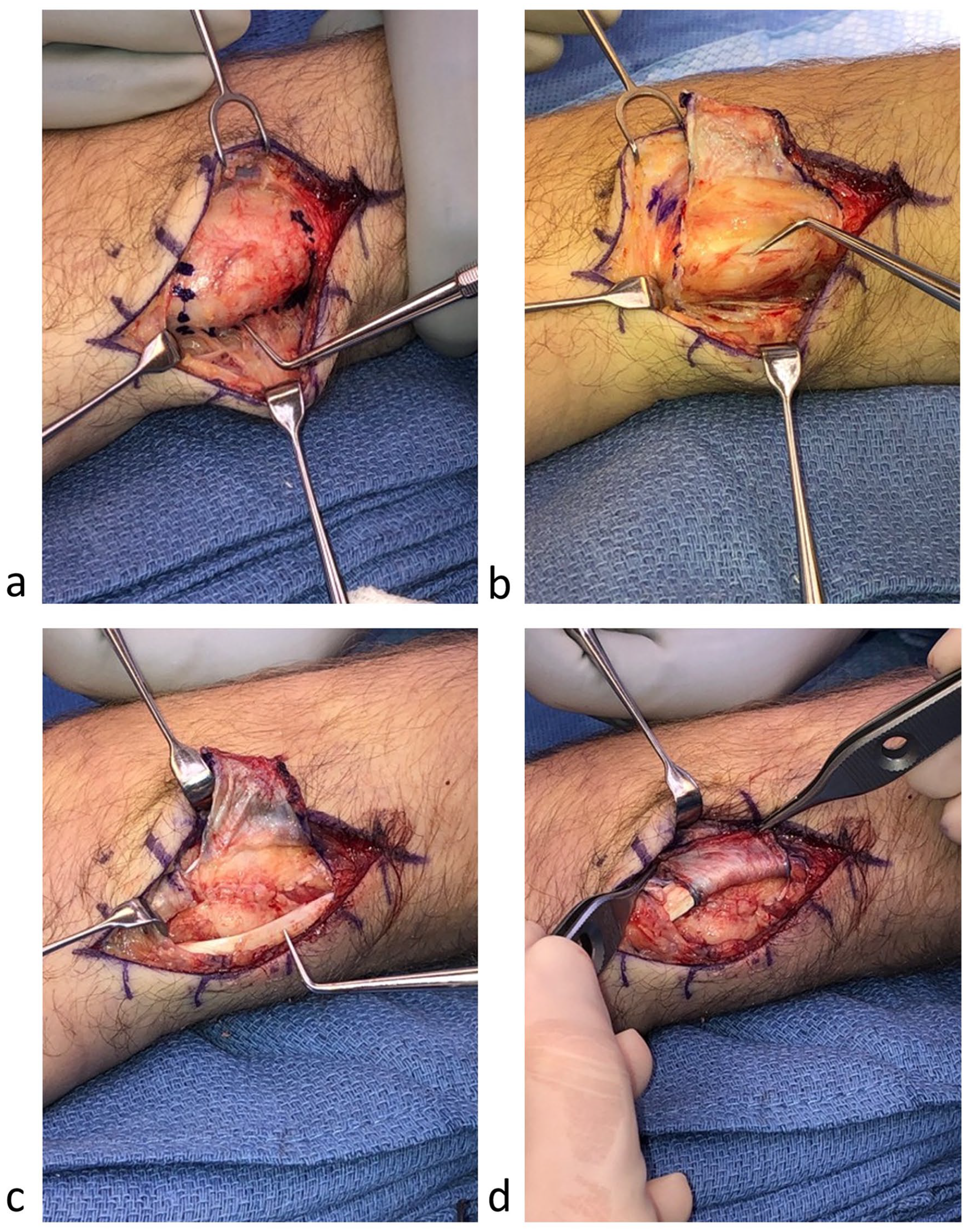
(a) Radially based extensor retinacular flap. (b) After retinacular sling elevation, the acute tear of the fibrocartilaginous subsheath is seen with resultant extensor carpi ulnaris instability. (c) The dorsal-radial lip of the native osseous sulcus is coplaned flush with the floor of the sulcus to allow for smooth transitioning of the extensor carpi ulnaris during wrist and forearm motion. (d) Retinacular sheath reconstruction completed with smooth gliding and excursion of the extensor carpi ulnaris during pronosupination.
Postoperative Follow-up
After skin closure, a sugar tong long-arm orthosis with the elbow flexed and the forearm in pronation and the wrist extended was applied. This long-arm orthosis or a Muenster orthosis was used until approximately 4 weeks after surgery. At 4 weeks postoperatively, active and active-assisted motion of the wrist and forearm is initiated and the athlete is transitioned into a forearm-based orthosis. The forearm-based orthosis is weaned between 6 and 8 weeks postoperatively. If there is persistent stiffness at 6 weeks, gentle passive motion is added to the rehabilitation protocol. No patients required static progressive splinting. Strengthening was initiated between 8 and 10 weeks after surgery. Sport-specific activities are allowed between 3 and 4 months after surgery in most cases.
Results
In our prospective consecutive cohort, there were no cases of recurrent ECU subsheath insufficiency or apprehension with provocation on clinical examination, and there were no major or minor complications after surgery. One elite athlete required secondary surgery for a recurrent grade 1B TFCC tear 7 months postoperatively, but their ECU remained stable. There was a statistically significant increase in grip strength from 39.8 to 40.9 kg (P = .001) and wrist flexion-extension arc from 140.5° ± 16.3° to 148.5° ± 11.8° (P = .037) after surgery, but not in pronosupination arc from 155° ± 4.4° to 158.6° ± 4.4° (P = .093) after surgery. There was no recorded preoperative Visual Analog Scale (VAS) pain score; however, postoperative VAS pain was 0.25 ± 0.43 (Table 1). All patients made a full return to sport to the same or higher level of competitiveness in 92.5 ± 21 days. Mean follow-up was 4.3 ± 1.8 months.
Classifications of ECU subsheath injuries by Inoue and Tamura 4 and Allende and Le Viet 5 are described in Table 2. Concurrent wrist pathologies found on either preoperative imaging or wrist arthroscopy were also cataloged. Inoue and Tamura type C and Allende and Le Viet type B ECU subsheath injuries were most prevalent in our cohort (78.6%). Extensor carpi ulnaris tenosynovitis, ulnocarpal synovitis, and/or TFCC pathology were present in most patients in our cohort.
Concurrent Wrist Injuries Presenting in Elite Athletes With Extensor Carpi Ulnaris Subsheath Injuries.
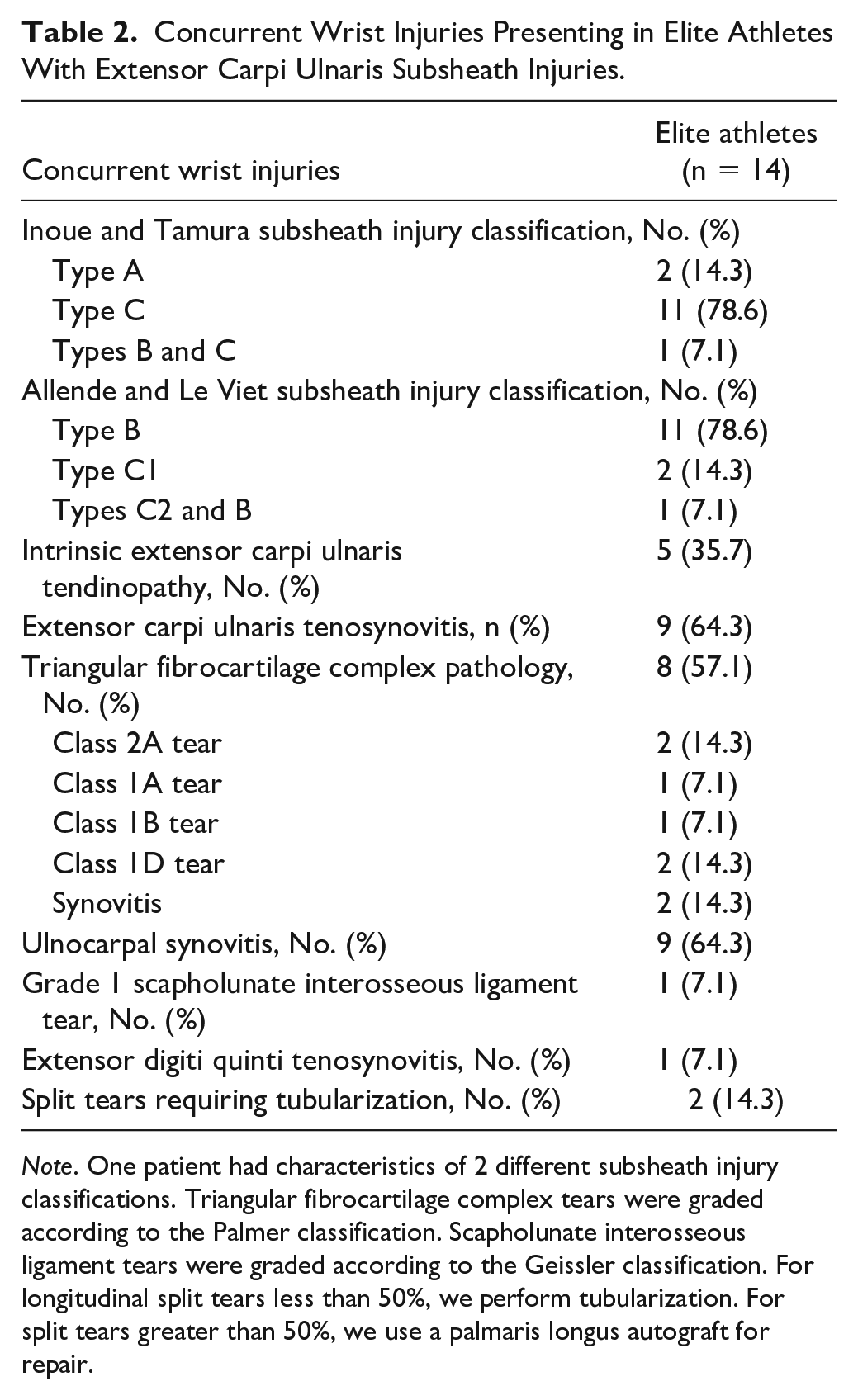
Note. One patient had characteristics of 2 different subsheath injury classifications. Triangular fibrocartilage complex tears were graded according to the Palmer classification. Scapholunate interosseous ligament tears were graded according to the Geissler classification. For longitudinal split tears less than 50%, we perform tubularization. For split tears greater than 50%, we use a palmaris longus autograft for repair.
Subgroup analysis of the 5 acute subsheath injuries in our elite athlete cohort revealed 4 patients were hockey players and 1 tennis player. Clinically relevant demographic, examination findings, injury classifications, and surgical outcomes in patients with acute subsheath injuries are reported in Table 3. All patients with acute injuries underwent an MRI, 3 had plain-film radiographs (60%), and 2 underwent ultrasound evaluation (40%). Mean time from symptom onset to presentation was 4.6 ± 2.2 days. Wrist arthroscopy was performed in 4 patients (80%). Three patients had TFCC tears (1 was a grade 2A tear, 1 was a grade 1A tear, and 1 was a grade 1D tear).
Subgroup Analysis of Elite Athletes With Acute Subsheath Injuries and Hockey Players in Our Cohort.
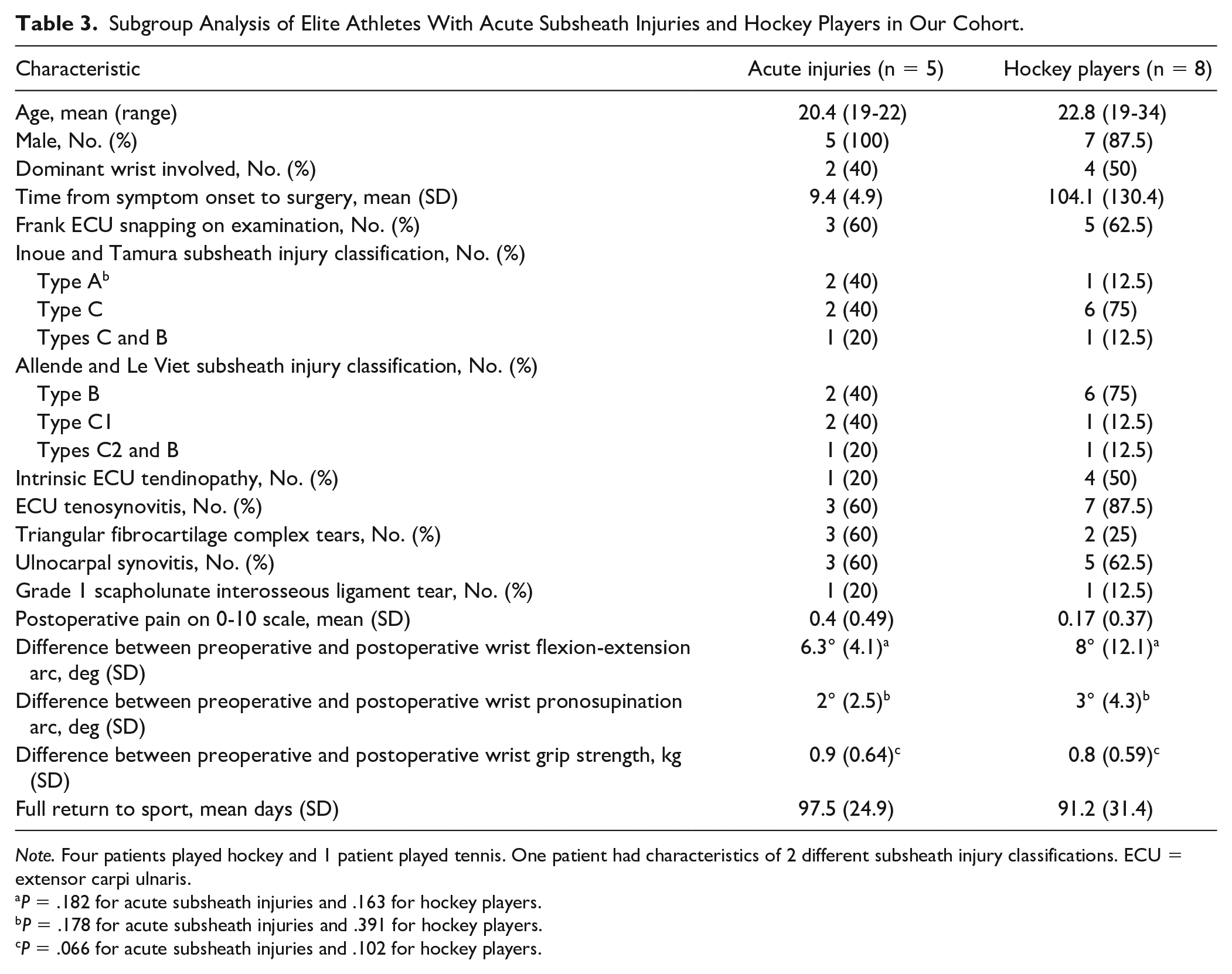
Note. Four patients played hockey and 1 patient played tennis. One patient had characteristics of 2 different subsheath injury classifications. ECU = extensor carpi ulnaris.
P = .182 for acute subsheath injuries and .163 for hockey players.
P = .178 for acute subsheath injuries and .391 for hockey players.
P = .066 for acute subsheath injuries and .102 for hockey players.
Subgroup analysis of all 8 hockey players was also performed (Table 3). All patients with acute injuries underwent an MRI, 4 had plain-film radiographs (50%), and 1 had ultrasound (12.5%). Mean time from symptom onset to presentation was 13.1 ± 15 days. Wrist arthroscopy was performed in 4 patients (80%). Two patients (25%) had TFCC tears (1 was grade 2A and 1 was grade 1D)
Discussion
There have been a number of described operative techniques for the treatment of ECU subsheath injuries; however, there is a lack of reported surgical outcomes, especially in elite athletes, making it difficult to determine the optimal surgical approach in this unique patient population. We present the largest prospective consecutive cohort analysis in elite athletes to date, and our radially based ER sling approach to ECU subsheath reconstruction in 14 patients resulted in significant functional improvement, expedited return to sport, and no complications. Grip strength and wrist flexion-extension and pronosupination arcs showed excellent recovery postoperatively, and postoperative pain was minimal in our cohort. The elite athletes in our study were able to make a full return to sport without restrictions and at the same or higher level of competition at approximately 3 months postoperatively, without any recurrence of ECU subsheath insufficiency.
Our secondary objective was to characterize the prevalence of concurrent wrist pathologies in our cohort. Previous studies have not highlighted the coincidence of concurrent wrist pathologies in elite athletes, with only Montalvan et al 11 finding a high coincidence of ECU tenosynovitis with instability in their case series. In our experience, ECU subsheath injuries most commonly presented with other ulnocarpal compartmental injuries, with only one case (7.1%) of isolated ECU insufficiency. Extensor carpi ulnaris tenosynovitis, ulnocarpal synovitis, and/or TFCC pathology were present in most patients in our cohort as outlined in Table 2. We identified 6 (42.9%) TFCC tears and found that most TFCC tears in our cohort were traumatic class 1 tears, which differs from our findings in nonathletes where 85.7% of patients had chronic degenerative class 2 tears (Table 4).
Concurrent Wrist Injuries in Nonathletes Presenting With Extensor Carpi Ulnaris Subsheath Injuries.
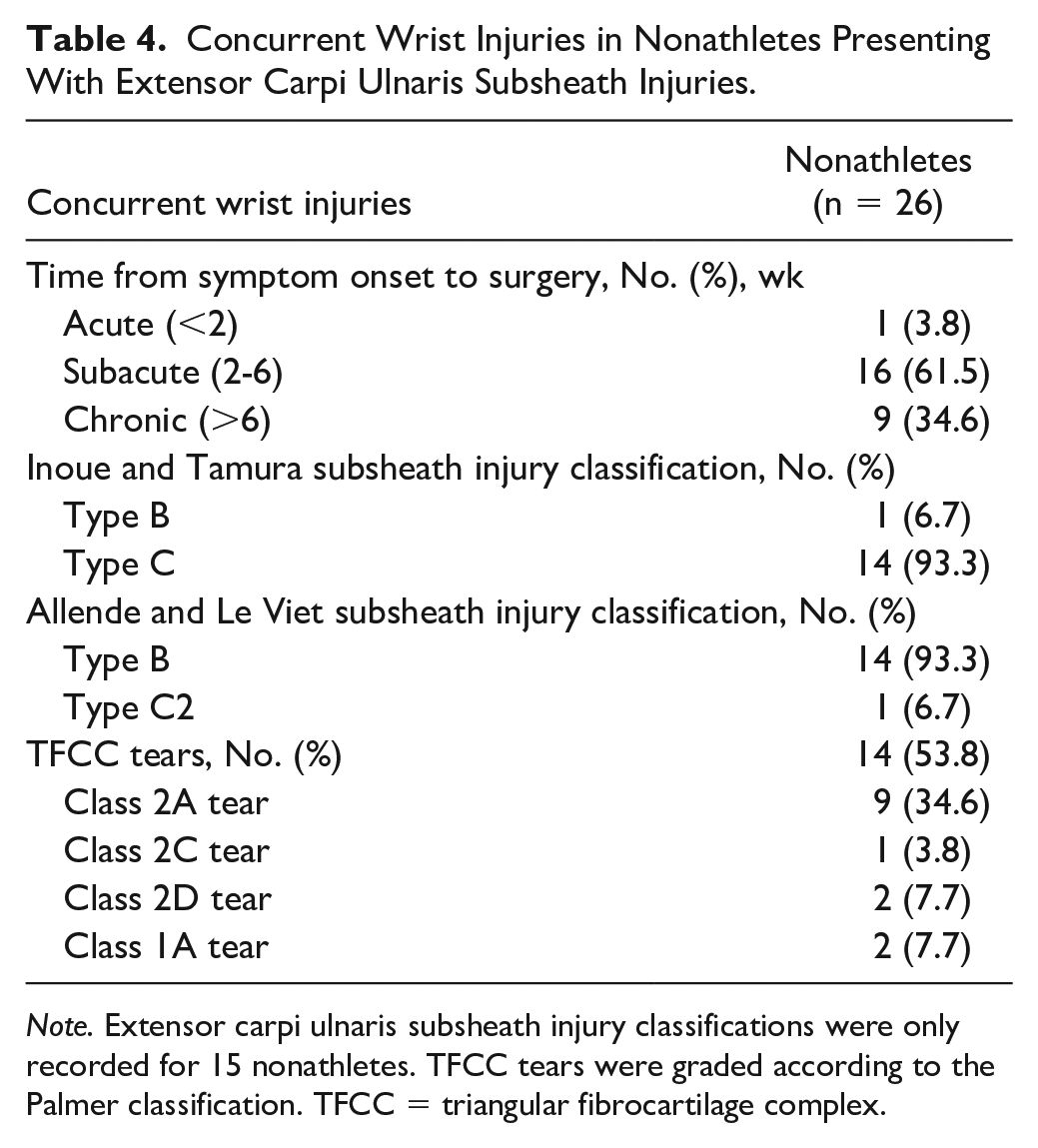
Note. Extensor carpi ulnaris subsheath injury classifications were only recorded for 15 nonathletes. TFCC tears were graded according to the Palmer classification. TFCC = triangular fibrocartilage complex.
Consistent with these findings, our subgroup analysis of 5 elite athletes with acute subsheath injuries identified 2 Inoue and Tamura type A injuries (40% of acute injuries), a similar proportion found in Jeantroux et al 21 which attributed their higher proportion of Inoue and Tamura type A injuries to the relatively early presentation compared with other studies. 9 Nonathletes at our hand center have almost always presented with subacute or chronic subsheath injuries, and our results suggest that the vast majority of subsheath injuries in this nonathlete cohort were consistent with Inoue and Tamura type C injuries. 20 Altogether, these findings suggest that timing from injury to presentation plays a role in the classification of ECU subsheath injuries and that athletes are more likely to present with acute subsheath and concurrent traumatic TFCC tears.
Given the coincidence of ECU subsheath pathology and ulnocarpal compartment injuries, we frequently perform wrist arthroscopy before ECU reconstruction for both diagnostic purposes and treatment of ulnocarpal lesions such as TFCC injuries. The 6R or 6U portal site(s) may be incorporated into the lazy-S incision used for ECU subsheath reconstruction. Although 2 patients had no snapping or apprehension with provocation on examination, they all had subacute or chronic subsheath tears with clear findings of ECU tenderness on palpation in combination with MRI evidence of subsheath insufficiency and disruption. This was confirmed on intraoperative examination. Two patients also did not receive wrist arthroscopy because they had no signs of TFCC or distal radioulnar joint pathology on examination or imaging, but one had intrinsic tendon pathology and tenosynovitis and the remaining patient had a rare isolated ECU subsheath tear and no concurrent injury. Our approach facilitates treatment of concurrent ECU tenosynovitis or longitudinal split tears, with elevation of the ER allowing for inspection and treatment of ECU tendon pathology while limiting the potential for stenosing tenosynovitis seen in primary subsheath repair.
Although it may be difficult to determine whether ECU subsheath injury is the sole and principal cause of pain, ECU tendon instability is a well-documented source of ulnar-sided wrist pain,7,8,11,15 and chronic ECU subsheath attrition and instability lead to symptomatic tenosynovitis and tendon tears that often require surgical correction.7,8,11 Sato et al 22 and Montalvan et al 11 illustrated how provocative examination maneuvers are not always definitive, with ECU snapping being less prominent in the nonacute setting. Jeantroux et al 21 treated 16 suspected acute ECU subsheath injuries with immobilization but only described radiographic outcomes. All patients had a persistently capacious ECU subsheath on subsequent appointments up to 3.5 months from injury with one patient having a recurrence of their subsheath injury.
After initial splinting with the elbow left free and the wrist pronated and slightly extended, Montalvan et al 11 left their elite tennis players immobilized until monthly MRIs and ultrasounds demonstrated subsheath reinsertion onto the ulnar head. In their experience, returning to sport too early generated recurring pain secondary to the force of their double-handed backhand, with 3 athletes treated nonoperatively for chronic attrition injuries returning to play 4 months from injury. 11 Moreover, Montalvan et al 11 identified 2 professional tennis players who were initially treated nonoperatively and then later developed a complete tendon rupture, effectively ending their playing careers. The authors also described nonoperative management in 5 tennis players with frank instability, noting tendinopathic features on advanced imaging. Nonoperative treatment led to return to sport between 5 and 6 months in these athletes, significantly longer than what was found in our cohort, although we only treated 1 tennis player who returned to play in 3.3 months.
Subgroup analysis of elite hockey players also characterized ECU subsheath and concurrent wrist injuries in these athletes. While previous studies have described the prevalence of ECU subsheath injuries in tennis and golf players,8,10,12 there has been only one case report reporting this injury in a competitive hockey player. 13 In a study of symptomatic tennis players, 11 42% of patients had ECU instability and 50% of patients had ECU tenosynovitis or tendinopathy. In our subgroup analysis of elite hockey players with ECU subsheath injuries, they had a higher proportion of concurrent ECU tenosynovitis (87.5%) and tendinopathy (50%) and a lower proportion of TFCC tears (25%) compared with the remainder of our cohort. Altogether, our findings may suggest that while stick athletes are at high risk of ECU subsheath injuries, differences in sport-specific mechanisms and biomechanical stress on the subsheath may predispose to different injury patterns and ulnocarpal compartment pathologies.
Previous studies describing surgical outcomes in athletes with ECU subsheath injuries are lacking. Allende and Le Viet 5 used the subsheath injury classification to guide their surgical approach and had 10 pro athletes (7 tennis, 1 golf, 1 basketball, and 1 judoka) in their case series. Reported outcome data were limited, but they found a return to previous level of sport by 8 months, far longer than observed in our cohort. Fram et al 16 used a similar ER sling approach to ours in 3 elite athletes and showed excellent improvement in pain and patient-reported outcomes with a return to sport at approximately 3 months. In addition to our larger sample size, restoration of grip strength, range of motion, and function in our series supports that radially based ER sling reconstruction facilitates recovery from ECU subsheath insufficiency. We also found a similar time to unrestricted return to sport in the athletes in our study, further illustrating that the radially based ER sling approach is effective in high-level athletes and affords reproducible results among different hand centers.
We propose a modified treatment algorithm in elite stick athletes, with surgical reconstruction as an acceptable alternative to nonoperative management, although this warrants further study and remains a multifactorial decision-making process that intimately involves the athlete/patient. Our radially based ER sling facilitates treatment of concurrent ECU tenosynovitis or longitudinal split tears, with elevation of the ER allowing for inspection and treatment of ECU tendon pathology while limiting the potential for stenosing tenosynovitis seen in primary subsheath repair for acute injuries. 10 Together, this approach allows for treatment of concurrent wrist injuries and may explain the lack of secondary surgeries, overall functional improvement, and faster return to sport in our cohort.
There are several limitations to our prospective study. It is a single-center study without a comparison cohort. A lack of patient-reported outcomes before surgery limited our ability to report on additional subjective outcomes, although anecdotally these outcomes seem to improve markedly. Variable time to presentation and postoperative follow-up may also contribute to our findings, given that athletes had unrestricted return to sport and their respective teams while being instructed to return if symptoms reoccurred. Depending on the sport, treatment and immobilization considerations may differ based on the stresses placed on the ECU subsheath during play and warrant further sport-specific outcome research. Despite these limitations, we believe this study contributes substantially to the current understanding of the surgical treatment of ECU subsheath insufficiency in elite athletes and believe future studies should continue to focus on surgical outcome reporting and subgroup analyses in this unique patient population.
In conclusion, radially based extensor retinacular sling ECU subsheath reconstruction resulted in functional improvement in this elite athlete cohort. The prevalence of concurrent wrist injuries with ECU subsheath insufficiency was cataloged and subgroup analysis was used to characterize these injuries in elite hockey players. Overall, our findings suggest that surgical management of ECU subsheath injuries is a predictable option in both the acute and chronic setting in elite athletes and may be favorable compared with nonoperative management.
Supplemental Material
sj-docx-1-han-10.1177_15589447231151433 – Supplemental material for Radially Based Extensor Retinacular Sling Reconstruction for Extensor Carpi Ulnaris Subsheath Injuries in Elite Athletes
Supplemental material, sj-docx-1-han-10.1177_15589447231151433 for Radially Based Extensor Retinacular Sling Reconstruction for Extensor Carpi Ulnaris Subsheath Injuries in Elite Athletes by Michael A. Mastroianni, Matthew Leibman, Mark Belsky, Mark A. Vitale and David E. Ruchelsman in HAND
Supplemental Material
sj-jpg-2-han-10.1177_15589447231151433 – Supplemental material for Radially Based Extensor Retinacular Sling Reconstruction for Extensor Carpi Ulnaris Subsheath Injuries in Elite Athletes
Supplemental material, sj-jpg-2-han-10.1177_15589447231151433 for Radially Based Extensor Retinacular Sling Reconstruction for Extensor Carpi Ulnaris Subsheath Injuries in Elite Athletes by Michael A. Mastroianni, Matthew Leibman, Mark Belsky, Mark A. Vitale and David E. Ruchelsman in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental materialis available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.