
Abstract
Background:
The human peripheral nervous system embodies anatomical, physiologic, and diagnostic perplexities that remain unexplained. Yet in the course of human history, there are no mechanisms, such as computed tomography (CT) or radiography, by which to image the peripheral nervous system in vivo using a contrast agent that is identified by ionizing radiation, which would aid in surgical navigation, diagnostic radiology, and basic science thereof.
Methods:
A novel class of contrast was created by linking iodine to lidocaine. The radiodensity of 0.5% experimental contrast molecule was compared with a control of 1% lidocaine by placing 1.5-mL aliquots of each liquid into centrifuge tubes and performing micro–computed tomography (micro-CT) synchronously under identical settings. Physiologic binding to the sciatic nerve was evaluated by injecting 10 mg of the experimental contrast and 10 mg of the control into the contralateral sciatic nerve, and documenting loss of hindlimb function and recovery. In vivo visualization of the sciatic nerve was evaluated by injecting 10 mg of experimental contrast or control into either sciatic nerve and imaging the hindlimbs under identical conditions using micro-CT.
Results:
The mean Hounsfield unit of the contrast was 56.09 compared with −0.48 for control (116-fold increase, P = .0001). Hindlimb paresis revealed similar degree of paresis, baseline recovery, and time to recovery. In vivo enhancement between the contralateral sciatic nerves was similar.
Conclusion:
Iodinated lidocaine offers a viable mechanism for in vivo peripheral nerve imaging using CT; however, it requires modification to improve in vivo radiodensity.
Background
Human peripheral nerve anatomy and function have a high degree of anatomical, functional, and diagnostic obscurity, which impedes our collective understanding and amelioration of peripheral nerve diseases.1 -3 Current methods of imaging the human peripheral nervous system include magnetic resonance imaging, ultrasound, and of late amino acid fluorescence.4 -6 The former is limited by motion artifact due to the need for patients to lie exceedingly still for long periods of time, limited cross-sectional thickness, and limited contrast from the surrounding soft tissues. Ultrasound is limited by user-dependent variability, limited depth of imaging, lack of contrast, and inability to render a composite view of the global (or regional) peripheral nervous system in the same image.
Therefore, what is needed is a mechanism to view the global peripheral nervous system in an expedient high-resolution manner that provides contrast between the surrounding tissues and minimizes human variability. Mammalian axons ubiquitously express sodium-gated ion channel (NaV) for the conduction of electrical impulses and are obligatory for neuronal function. 7 Lidocaine is a commonly used anesthetic that binds solely to the NaV. 8 The lidocaine molecule contains 3 components: a tertiary amine, amide, and aromatic ring group. The tertiary amine is critical to NaV channel binding, the amide functions as a linking agent to the aromatic ring, and the aromatic ring serves as a stable R-group with a diminutive role. Computed tomography angiography (CTA) contrast (eg, Omnipaque; GE Healthcare, Chicago, Illinois, USA) is made possible by the addition of 3 iodine groups on an aromatic ring (Figure 1). Thus, a novel class of compounds to permit visualization of the peripheral nervous system using CT has been created by linking iodine to the aromatic ring of the lidocaine molecule.
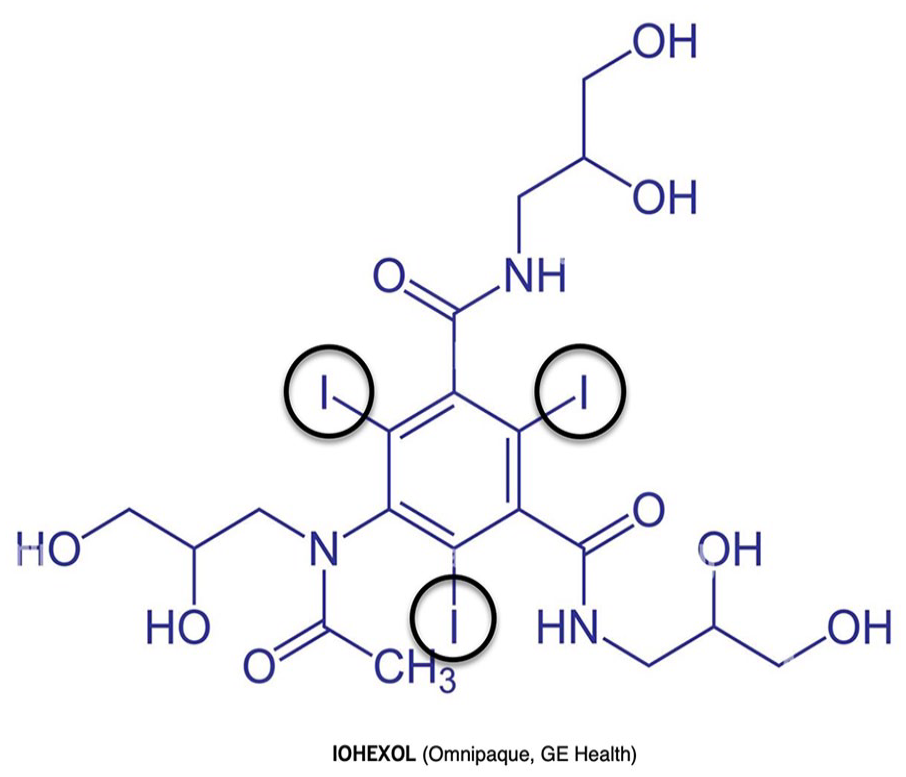
Iohexol (Omnipaque; GE Healthcare).
Methods
A proprietary synthesis reaction was used to link an iodine atom to the meta position on the benzene ring of a lidocaine molecule creating N-(4-iodo-2,6-dimethylphenyl)-(diethylamino)acetamide (Figure 2) and formulated to a 0.5% (5 mg/mL) concentration.
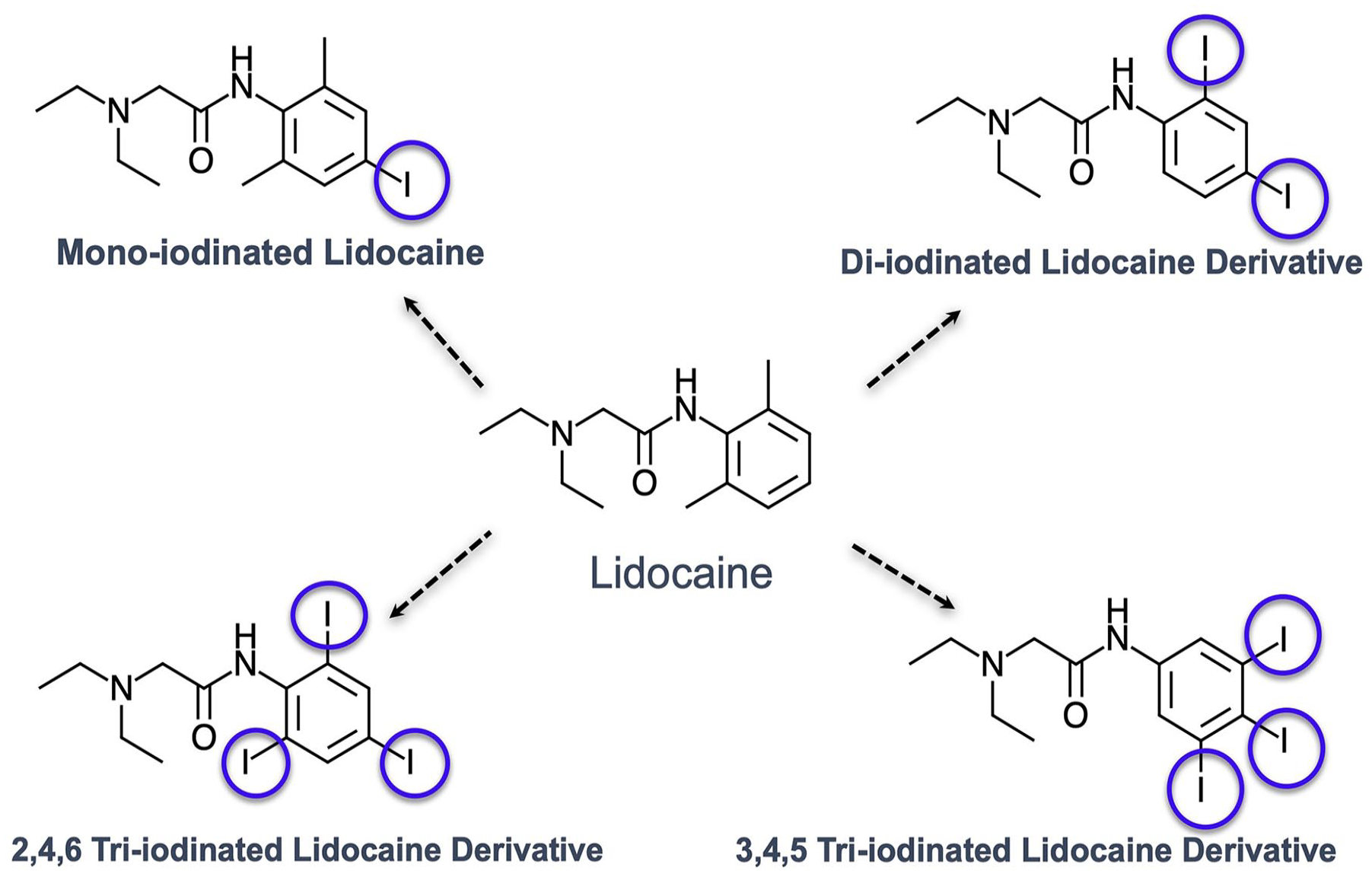
Experimental contrast representing an iodinated version of lidocaine.
Radiodensity of Experimental Contrast
The radiodensity of 0.5% experimental contrast molecule was compared with a control of 1% (10 mg/mL) lidocaine by placing a 1.5-mL aliquot of each liquid into polypropylene centrifuge tubes (Eppendorf, Hamburg, Germany) and performing micro–computed tomography (micro-CT) (Quantum GX2; PerkinElmer, Waltham, Massachusetts) at the same time under identical settings (70 kV, 88 µA, field of view [FOV] 72 mm, scan time 4 minutes). The average, minimum, and maximum Hounsfield units were then measured under identical regions of interest. The difference in means was analyzed using a paired Student t test with statistical significance at P < .05. The solid state of the compound was imaged using a GE C-arm, and its Hounsfield units were measured.
Physiologic Binding of Experimental Contrast
To assess the physiologic binding of the molecule to the mammalian nervous system, 10 mg of the experimental molecule was injected into the left hindlimb of an 8-week-old Wistar rat (Cambridge, Massachusetts) weighing 250 g, while the contralateral right hindlimb sciatic nerve was injected with 10 mg of lidocaine. Injection to the sciatic nerve was achieved by anesthetizing the rat using sevoflurane and then placing it into the supine position. The greater trochanter and ischial tuberosity were then palpated, and a visualized line from the greater trochanter to the ischial tuberosity was noted. In the region immediately caudal to the greater trochanter, a 27-gauge needle was advanced and either solution was slowly injected. On wakening from anesthesia, the duration of gross impaired gait (total active range of motion) was observed and recorded for each hindlimb every 5 minutes until equivalent.
Radiographic Binding of Experimental Contrast
To evaluate the radiographic binding of the molecule to the mammalian peripheral nerve, a separate Wistar rat of similar age and weight to the gait analysis was anesthetized and the sciatic nerve in the left hindlimb was injected with 10 mg of the experimental contrast, while the right hindlimb was injected with 10 mg of lidocaine as previously described. The rat was then imaged after waiting 20 minutes using micro-CT (70 kV, 88 µA, FOV 72 mm, scan time 4 minutes). As an internal control, 10 mg of the experimental contrast was injected into the subcutaneous tissue of the anterior abdomen, which was imaged at the same time as the hindlimbs.
Results
Radiodensity
The mean Hounsfield unit of the control was −0.48 (min, −73.53; max, 66.47; SD, 27.67) and of the contrast was +56.09 (min, −5.30; max, 120.59; SD, 22.57; Figure 3, P = .0001). The Hounsfield unit of the solid compound state was 3,058 (Figure 4).
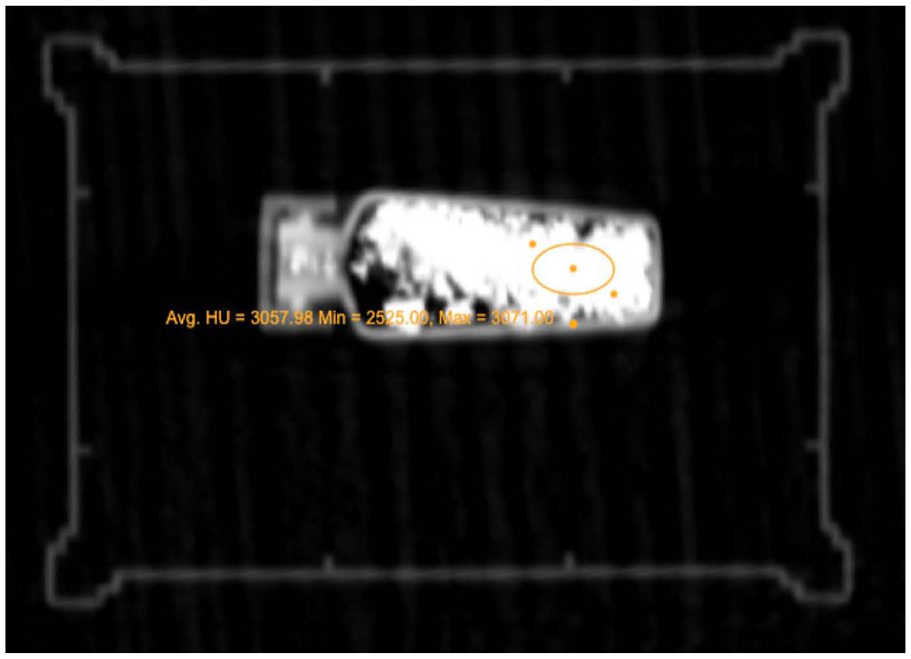
Computed tomographic density of the solid form of experimental contrast.
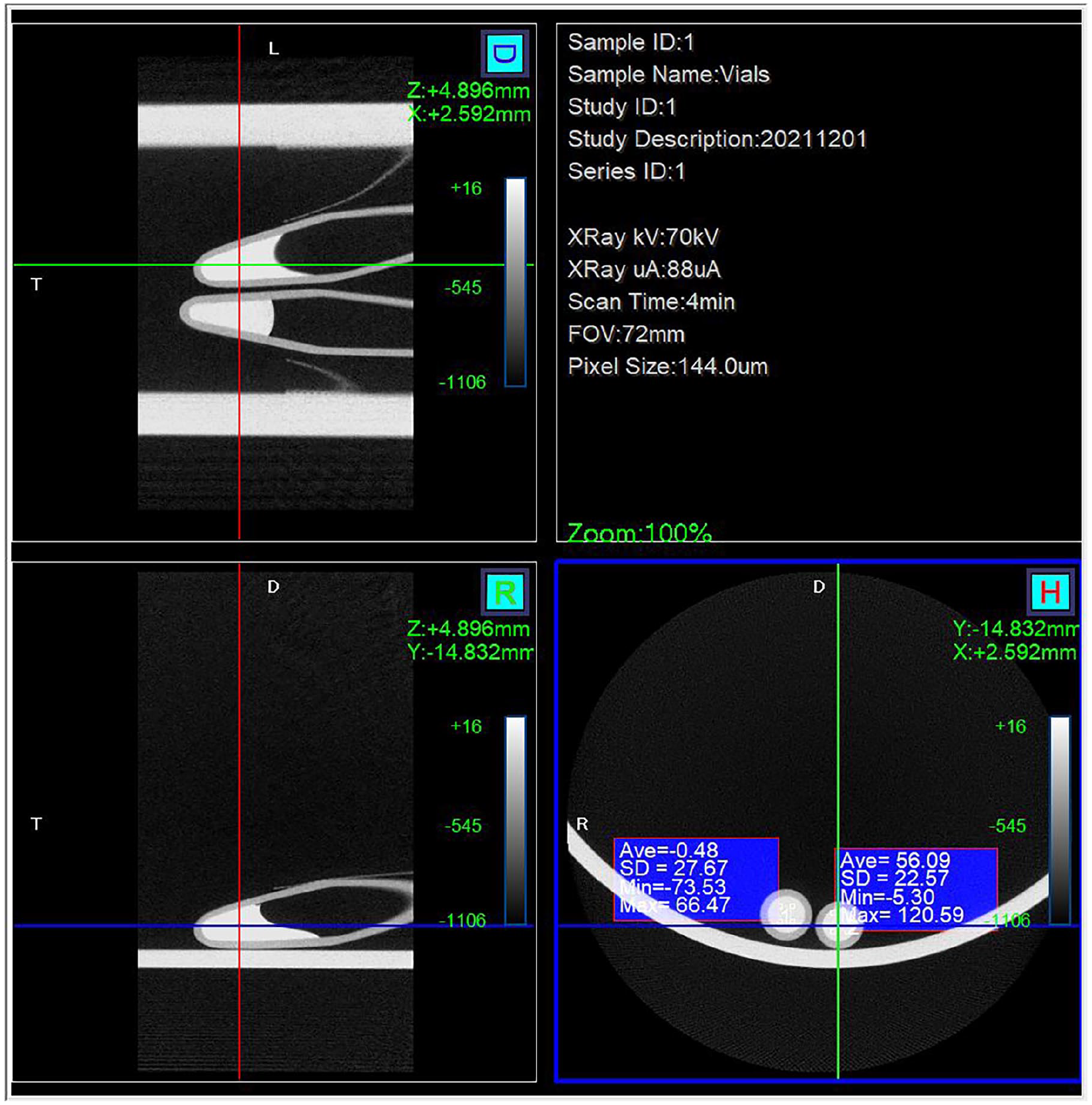
1% lidocaine on left with 0.5% contrast (experiment) on right.
Physiologic Binding of Experimental Contrast
A dense paresis of both hindlimbs was observed within 60 seconds of injection into either limb with the control and contrast, respectively. The rat at this time demonstrated dependent forelimb gait with dragging of the hindlimbs in a symmetrical manner. The gross percentage of normal active range of motion for each limb displayed similar rates of normalization (Figure 5).
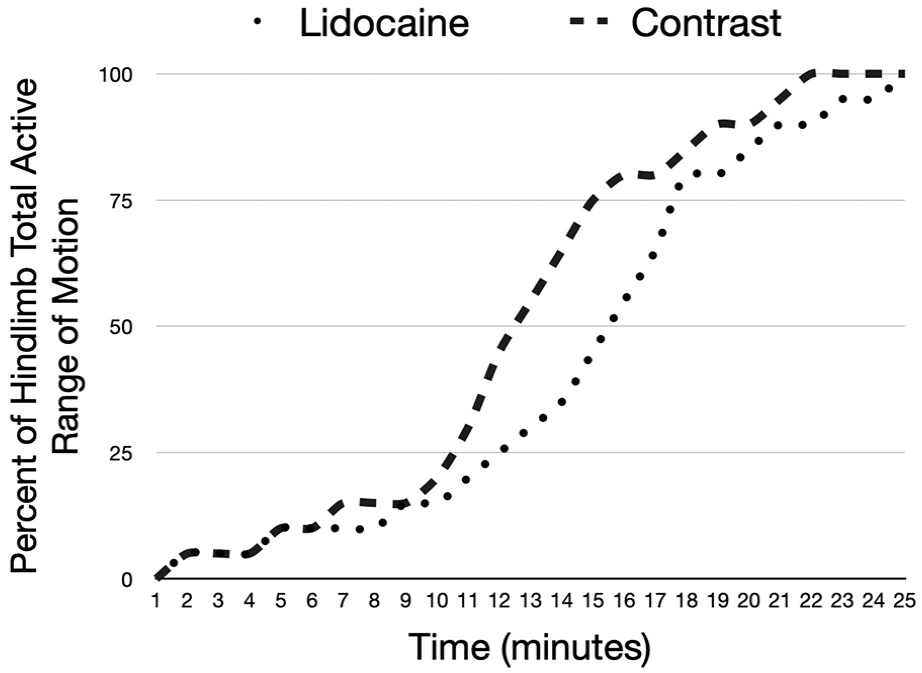
Physiologic effect of 0.5% contrast (experiment) and 1% lidocaine.
Radiographic Binding of Experimental Contrast
The experimental and control limb demonstrated symmetric lack of contrast within the sciatic nerve, with the absence of contrast enhancement within the subcutaneous tissues of abdomen on 3-dimensional reformatting and cross-sectional micro-CT (Figure 6).

Three-dimensional axial images demonstrating isometric enhancement of the sciatic nerve.
Discussion
Santiago Ramon y Cajal and Camillo Golgi provided humanity with the fundamental layout of neuronal anatomy through the development of silver staining technique and in vitro investigations for which they shared the first Nobel Prize in Medicine in 1906. The visualization of neuroanatomy provided a framework for developing theories to advance the understanding of its function and teleology. Toward this end, a contrast agent that localizes to neurons in vivo provides a mechanism to further refine our collective understanding of neuronal form and function, both clinically and in basic sciences.
The neuronal contrast agent presented in this pilot study incorporates 2 well-known, and importantly safe, chemical moieties: lidocaine and iodine. Lidocaine specifically binds to the NaV without other known ligand receptors. Iodine has been used in a host of CT angiogram agents, with more being added yearly. Except for allergic reactions, it is well tolerated. Thus, the combination of these 2 elements demonstrates a logical standing. The statistically significant difference in Hounsfield units (a marker of density) between the contrast and control refutes the null hypothesis of these 2 compounds having the same density. Additional iodine groups within the aromatic ring and alterations in the formulation to obtain a greater concentration are anticipated to provide greater Hounsfield unit values, which have been designed (Figure 1) with plans to execute additional studies.
Given the pilot study nature of this experiment, we sought to answer whether the contrast agent would produce any evidence of physiologic blockade using the total active range of motion compared with baseline assessment. The assessment was based on visual assessment in contrast to a goniometer or electromyogram/nerve conduction study, which was beyond the scope of this study. The 2 curves approximated each closely, with 1% lidocaine having a slightly denser paresis, with longer time until reaching full total active range of motion. It is unclear whether this was a function of bone fide differences in how the experimental and control arms bind to the NaV, or how much agent is injected to the actual sciatic nerve, or a combination of both phenomena. To provide greater clarity about the physiologic binding and visual enhancement of the contrast, future studies have been designed.
Conclusion
An original contrast agent has been created based on the combination of a well-known anesthetic and the functional group (iodine) of commonly used contrast agents. This experimental nerve-specific contrast demonstrates favorable ionizing contrast with CT and physiologic binding to mammalian nerves, although insufficient in vivo enhancement in its current structure and concentration is to be visualized through soft tissues.
Footnotes
Acknowledgements
The authors wish to acknowledge Jenna Steiner for her overwhelming technical support without which this work could not have been completed.
Ethical Approval
Institutional Review Board and Institutional Animal Care and Use Committee approval were obtained prior to animal experiments.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant provided by the UCHealth Northern Colorado Foundation.