
Abstract
Background:
As health care costs in the United States continue to rise, there is increasing attention on cost-saving measures. One area of investigation is the utility of pathologic examination of specimens from routine procedures with a suspected benign pathology. We assessed the utility and cost of routine pathologic analysis for wrist ganglion cyst excision.
Methods:
A retrospective cohort study of all wrist ganglion cyst excisions performed by seven hand surgeons was conducted from 2015 to 2019 at Penn State Hershey Medical Center. Preoperative and intraoperative diagnoses, pathologic diagnosis, and pathology cost were assessed.
Results:
A total of 407 patients underwent ganglion cyst excision, with 318 (78.1%) specimens sent for pathologic review. Of the 318, 317 (99.6%) specimens were concordant with the preoperative or intraoperative diagnosis of ganglion cyst. One specimen (0.3%) resulted as a benign cystic vascular malformation. The charge per specimen was $258, totaling $81,786 spent confirming benign pathology that was clinically correctly diagnosed by the operating surgeon in 99.6% of cases.
Conclusions:
Routine pathologic analysis is not indicated in cases in which surgeons have a high clinical suspicion for ganglion cyst based on preoperative and intraoperative findings. Pathologic review should be reserved for cases with atypical presentations or intraoperative findings.
Keywords
Introduction
At 18% of its gross domestic product, the United States spends more money on health care than any other nation. 1 Estimates predict one third of all health care spending is wasteful in the form of overtreatment, fraud, administrative complexity, and failure of care delivery and coordination.2,3 In a Journal of the American Medical Association review based on US population-based publications from 2012 to 2019, low-value testing, defined as “services that provide no or minimal benefit to a patient in a specific clinical situation,” was estimated to cost between 17 and 28 billion dollars annually. 2 Increasing attention is being placed on cost-benefit analyses as health care costs are projected to grow an average of 5.4% per year to reach $6.2 trillion by 2028. 4
The College of American Pathologist’s statement on surgical specimen pathologic evaluation recommends that institutions create policies based on the likelihood of significant findings in a given clinical situation. However, they do not suggest considering the incidence of malignancy in the analysis of routine benign pathologies. 5 Studies have questioned the need for routine pathologic examination in a variety of tissues, including tonsils and adenoids, 6 hernia sacs,7,8 gallbladders, 9 appendixes, 9 intervertebral disks, 10 ankle arthroscopy tissue, 11 and mastectomy scars following implant-based breast reconstruction. 12
In line with other surgical specialties, data have emerged in hand surgery over the past 15 years questioning the necessity of routine specimen pathology. There is an approximately 2% risk of a lesion being malignant in the upper extremity. 13 Furthermore, when soft tissue masses are evaluated by hand surgeons, the rate of discrepant diagnosis requiring change in treatment algorithm is low. 14 Due to the rare incidence of malignant tumors and high pretest probability of a benign lesion being concordant with preoperative diagnosis, the cost-effectiveness of a routine histologic analysis in upper extremity tumors has been questioned.14,15 Despite mounting evidence questioning the necessity, 69% of nonmalignant upper extremity specimens are sent for pathologic analysis in a national database study including over 200,000 patients. 16
Ganglion cysts are the most common tumor of the hand and represent 50% to 70% of all benign upper extremity tumors. 17 Given their characteristic location, appearance, and transillumination, experienced practitioners make preoperative diagnoses concordant with the pathologic analysis in 98% to 100% of cases.18,19 Thus the routine pathologic evaluation of ganglion cysts may be unnecessary considering the high pretest probability of a concordant diagnosis. The purpose of this study was to determine the submission rate, discordant rate of preoperative and intraoperative diagnoses with routine pathologic analysis of ganglion cysts, and cost associated with pathologic evaluation of wrist ganglion cysts.
Materials and Methods
A retrospective cohort study was performed at Penn State Health Milton S. Hershey Medical Center with institutional review board approval (study # 00013069). Coding records were queried for all patients who underwent ganglion cyst excision (Table 1) from 2015 to 2019 by seven fellowship-trained hand surgeons. Whether or not the ganglion cyst was sent for pathology was the decision of the operating surgeon. At our institution, it is not standard practice to send patients with clinically diagnosed ganglion cysts for imaging. Furthermore, ultrasound is not available for use in a clinical setting. Inclusion criteria included any patient who underwent primary or recurrent ganglion cyst excision of the wrist. Exclusion criteria included patients younger than 18 years or with incomplete surgical, clinical, or pathologic documentation. Identified records were reviewed for preoperative diagnosis, procedural diagnosis, intraoperative pathologic diagnosis, and pathology charges.
CPT Codes for Ganglion Cyst Excision Utilized to Identify Patients.
Note. CPT = Current Procedural Terminology.
Results
A total of 407 patients underwent ganglion cyst excision. Of those patients, 318 cases (78.1%) had a surgical specimen sent for pathologic review, and 89 cases (21.9%) did not send the specimen for pathology. Of the patients who had a specimen sent for pathology, 286 (89.9%) were definitively diagnosed with a ganglion cyst preoperatively. All these patients demonstrated concordant pathologic diagnoses of a ganglion cyst. Thirty-two patients (10.1%) carried an equivocal diagnosis that was not definitively a ganglion cyst preoperatively. Thirty-one of these patients had the diagnosis of ganglion cyst confirmed based on intraoperative inspection. The remaining 1 patient (0.3% of all specimens) was diagnosed with a cystic vascular malformation on pathologic evaluation (Figure 1). This diagnosis did not alter the clinical course of management and did not require further treatment. All reviewed specimens were associated with a “Level 3 Surgical Pathology” and “Tissue Exam Level 3” billing code, which corresponded to a billing charge of $258, totaling a cost of $81 786 over 5 years.
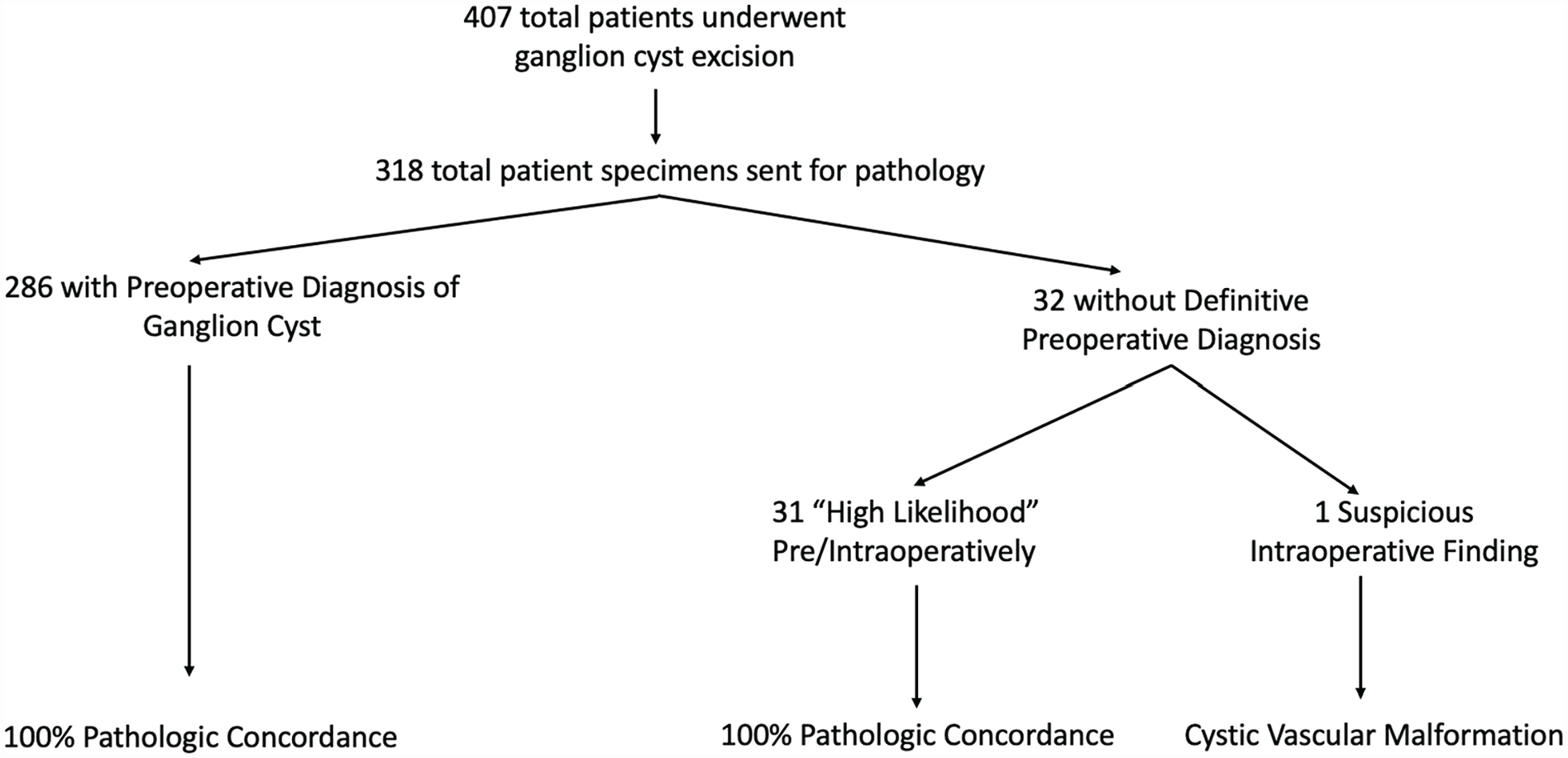
Pathologic concordance in the context of preoperative and intraoperative diagnoses.
Discussion
The estimated annual cost of routine pathologic evaluation of benign upper extremity specimens in the United States is five million dollars. 16 When questioning the cost-effectiveness of any medical test, the benefit of financial savings must be weighed against the risk of lack of diagnostic information. Even within the context of routine histopathology, a theoretical risk that a clinically significant disease remains undetected still exists. Although the cost society places on disease detection is an imperfect and ever-changing science, Raab 15 created a theoretical model of the cost-effectiveness of routine histologic specimen evaluation that accounts for cost and life expectancy gains from a discordant diagnosis detected by histopathology. This model suggests that to justify the associated cost, one of every 2000 specimens would have to be discordant with the preoperative diagnosis and clinically significant in that the treatment would alter expected life years. 15
In addition to the present study, two additional studies published comparable findings on excision of wrist ganglion cysts; their results are summarized in Table 2. Taken together, a total of 902 pathologic specimens were analyzed. Of those samples diagnosed preoperatively as a ganglion cyst, 99.4% had a concordant pathology. Of the 0.6% of specimens diagnosed as ganglion cyst preoperatively with a discordant pathologic diagnosis, all alternative diagnoses were benign. Five patients had equivocal preoperative or intraoperative diagnoses, 100% of which were discordant with benign masses other than a ganglion cyst on pathology. In total, independent of certainty of preoperative diagnosis, 10 of 907 (1.1%) patients who underwent wrist ganglion cyst excision ultimately had a discordant pathologic diagnosis. None of these manifested a clinically significant diagnosis that changed the course of treatment or altered expected life years. One can speculate that if a provider has any inclination that a mass could be a ganglion cyst, it likely has a benign clinical course and physical examination findings similar to those of a ganglion cyst, accounting for the complete lack of discordant malignant diagnoses. A discordant diagnosis is significantly more likely if the preoperative or intraoperative diagnosis is equivocal, with a 0.6% discordant diagnosis rate if there is high preoperative suspicion of a ganglion cyst versus 100% if the preoperative or intraoperative diagnosis is equivocal.
Data From Present Study and Two Previously Published Studies Investigating Concordant and Discordant Ganglion Cyst Pathologic Diagnoses.
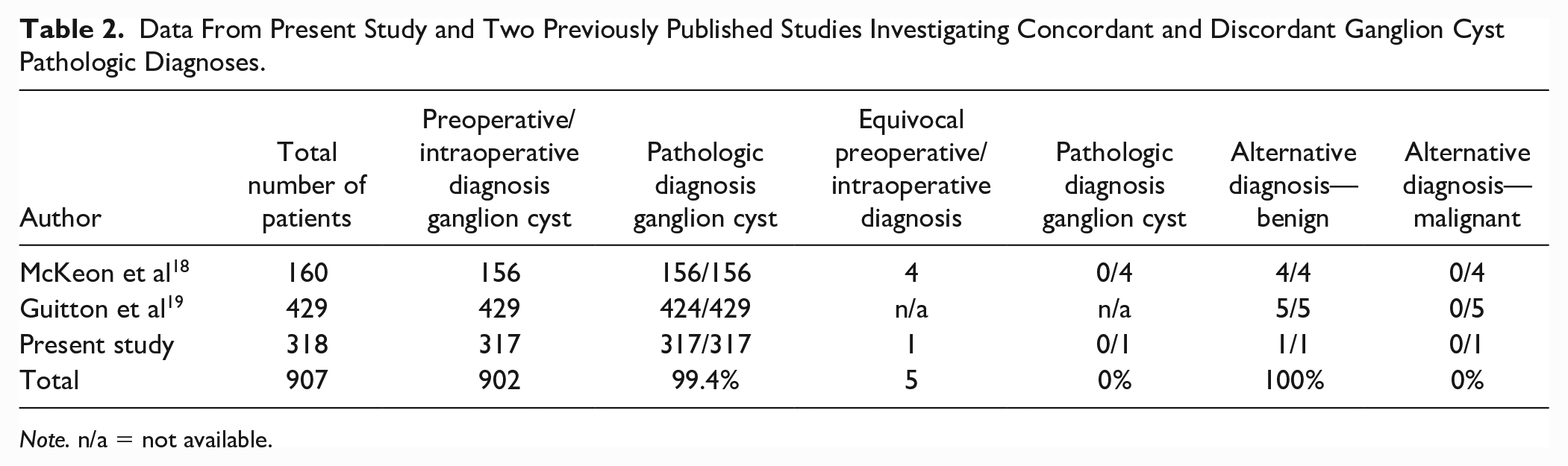
Note. n/a = not available.
This study demonstrates that, when the suspicion for a ganglion cyst by a fellowship-trained hand surgeon is high preoperatively and intraoperatively, the likelihood of a discordant diagnosis is exceedingly low. However, when the preoperative or intraoperative diagnosis is equivocal, the rate of discordance is high. It is important to note that a discordant malignant diagnosis resulting in a change in clinical course has not been recorded in the literature to date. These findings suggest that when preoperative or intraoperative suspicion for ganglion cyst is high, the routine pathologic analysis can likely be waived.
The primary limitation of this study is its retrospective nature. Given the decision to send specimens was that of multiple attending surgeons, this may introduce sampling bias into the study population. This study does not include information on preoperative imaging, which may influence the decision to send or not send a specimen and is also important to consider in an overall cost analysis. It is possible that other Current Procedural Terminology codes were used in cases in which ganglion cysts were excised, such as those for “mass excision.” However, the purpose of this study was to identify cases in which the operating surgeon diagnosed the mass as a ganglion cyst. As such, although this study may not include every confirmed ganglion cyst excised during the study years, we excluded undifferentiated codes as to avoid cases in which the preoperative diagnosis was equivocal. Finally, the sum total of published ganglion cyst pathologic findings is less than the most current calculation for cost justification, which recommends 2000 specimens without diagnostic discordance that decreases expected life years. 15 Future directions include additional studies to allow the field to reach that goal; however, all studies to date agree that when it comes to the routine pathologic diagnosis of wrist ganglion cysts, the cost is not justified.
Conclusion
Routine pathologic analysis is not indicated in cases in which the hand surgeon has a high clinical suspicion for a ganglion cyst based on preoperative and intraoperative findings. Pathologic review should be reserved for cases with atypical presentations or intraoperative findings.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This research did not involve experimentation on human or animal subjects.
Statement of Informed Consent
Given the retrospective nature of this research, informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.