
Abstract
Background:
Intramedullary screw fixation of the proximal ulna can be used for fixation of the ulnar component in total elbow arthroplasty. Our purpose was to use computed tomography (CT) to characterize proximal ulna anatomy with respect to intramedullary screw fixation, and then to validate this templating process by inserting intramedullary screws into 3-dimensional (3D)-printed models.
Methods:
Thirty elbow CT scans were reformatted in the axis of the proximal ulna. Screw placement was templated by fixing a length at 78 mm distal to the centerline of ulnohumeral rotation and measuring diameter, and then fixing the screw pitch diameter to 5.5 mm and measuring length. Three-dimensional models were printed for 5 patients, and intramedullary screws were advanced as distal as possible until endosteal fit was achieved.
Results:
All patients had an anatomic limit for intramedullary screw fixation, due to dorsal angulation, varus angulation, or both. At 78 mm distal to the centerline of rotation, mean screw diameter was 5.4 mm (range, 3.2-8.0). When fixing screw diameter to 5.5 mm, the mean screw length was 79.9 mm (range, 64.2-107.9). All intramedullary screws were placed in the 3D models within 3 mm of the templated length, with correlation coefficient 0.992.
Conclusion:
This study characterized proximal ulna anatomy in the context of intramedullary screw fixation. Templating allows surgeons to predict intramedullary screw sizing, and a broad range of screw lengths and diameters is required when attempting intramedullary screw fixation for placement of the ulnar component in uncemented total elbow arthroplasty.
Introduction
The anatomy of the proximal ulna has been characterized in both advanced imaging and cadaveric studies to give insight for total elbow arthroplasty implant design and olecranon fracture fixation.1-3 The proximal ulna generally exhibits a dorsal and varus angulation, with a fairly variable intramedullary canal diameter.1-3 Intramedullary olecranon screws provide reliable perpendicular compression at the fracture site and achieve rigid fixation via the proximal screw head, the screw shaft at the proximal ulnar bow, and through distal endosteal thread contact.4-7 In addition to fixation of proximal ulna fractures, it can be used for fixation of an uncemented ulnar component in total elbow arthroplasty. 8 Cementation of total elbow arthroplasty stems is the only available method of fixation and may risk osteonecrosis to the humerus and ulna. 9 Avoiding cemented fixation requires “off label” press fitting of the stem, and yet survivorship is poor with cemented ulnar components performing better than that of press fit uncemented ulnar components. 10
To avoid cement, an intramedullary screw construct was designed that pulls the implant into a cavity that is created for the body component within the olecranon. Intramedullary screw fixation aims for endosteal screw thread purchase and can achieve a high pullout strength. 11 Initial cadaver and Sawbones implantation efforts of this implant demonstrated that ulnar intramedullary fixation employed 1/4-20, 5/16-18, and 3/8-16 threaded screws. 8 A 1/4-20 screw has a 1/4″ diameter (6.35 mm outer diameter, 5.5 mm pitch diameter) with 20 threads per inch. All screws are available in 3 lengths. A better understanding of proximal ulnar anatomy in the context of intramedullary screw fixation may aid in selecting appropriate size screws. The purpose of this study was to use computed tomography (CT) to characterize proximal ulna anatomy and identify which screw diameter and length achieve thread purchase along the longest length of engagement within the intramedullary canal. Templating the screw that can be used for this process is the purpose of this research, and we will validate these results by inserting the recommended intramedullary screws into 5 randomly chosen 3-dimensional (3D)-printed models of the proximal ulna.
Materials and Methods
This study was approved by our institutional review board (STUDY20070308). We retrospectively identified 30 consecutive patients who underwent a CT scan of the elbow between November 1, 2018, and November 1, 2021. Patients were included if their ulnar diaphysis and olecranon were intact and they were over the age of 18. Patients were excluded if a fracture or hardware was present or if an incomplete portion of the ulna was captured. Computed tomography scans with 0.625 mm cuts were exported for analysis to VitreaCore Version 6.9.87.1 (Vital Images, Inc., Minnetonka, Minnesota). Three-dimensional ulnar reconstructions were reformatted to create sagittal and coronal reconstructions along the axis of the proximal ulnar intramedullary canal.
All measurements were made with respect to the centerline of ulnohumeral rotation, which was created by ensuring that medial and lateral, and dorsal and volar canal space was identical relative to this axis in the reformatted coronal and sagittal CT reconstructions. The first step measured the distance at which this line within the center of the intramedullary canal intersected with either the dorsal or lateral ulnar cortex (Figure 1).
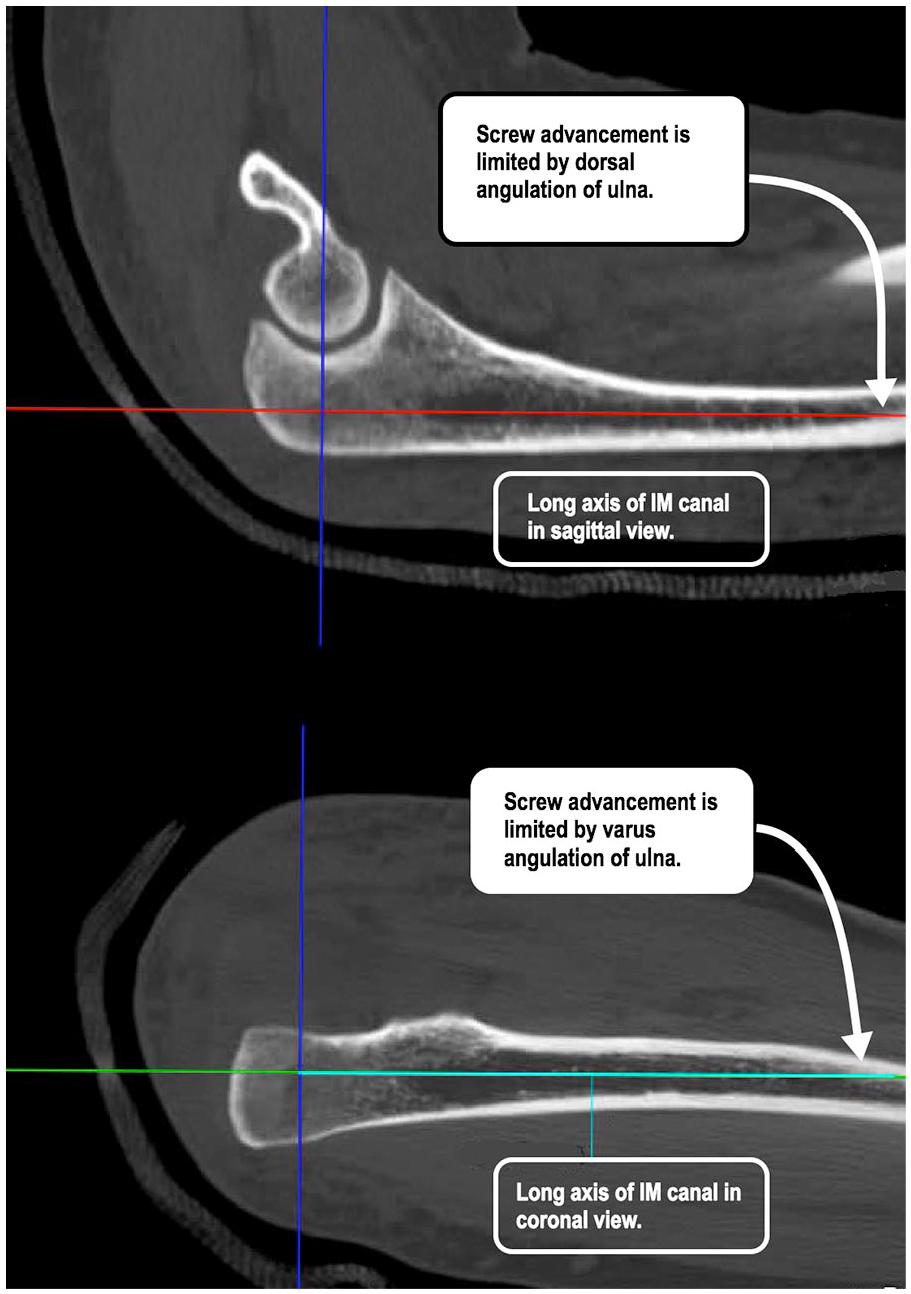
Determining the anatomic limit of IM fixation in the coronal and sagittal plane.
Two screw templating approaches were then employed with the first maintaining a constant screw length and the second maintaining a constant diameter. The screw location was referenced from the centerline of ulnohumeral rotation in the sagittal plane as this location is crucial when implanting the ulnar component of a total elbow arthroplasty system (Supplemental Figure 1). The fixed length approach was based on a dimension (78 mm) that corresponded to the distance along the intramedullary axis of the ulna between centerline of ulnohumeral rotation and the distal extent of a small 5/16-18 screw (Figure 2). Once this dimension was employed for each scan, the largest possible distance between the inner cortices of the intramedullary canal in the sagittal and coronal planes was recorded. The smaller of these 2 measurements determined the intramedullary screw diameter that would fit into the canal. The second templating approach employed the pitch diameter (5.5 mm) of a 1/4-20 screw (6.35 mm outer diameter) and translated this diameter as distally as possible in the coronal and sagittal reconstruction planes until it abutted the inner cortices (Figure 3). The length that made contact with the inside of the intramedullary canal in the coronal and sagittal planes was recorded and the smaller of the 2 measurements determined the screw length.
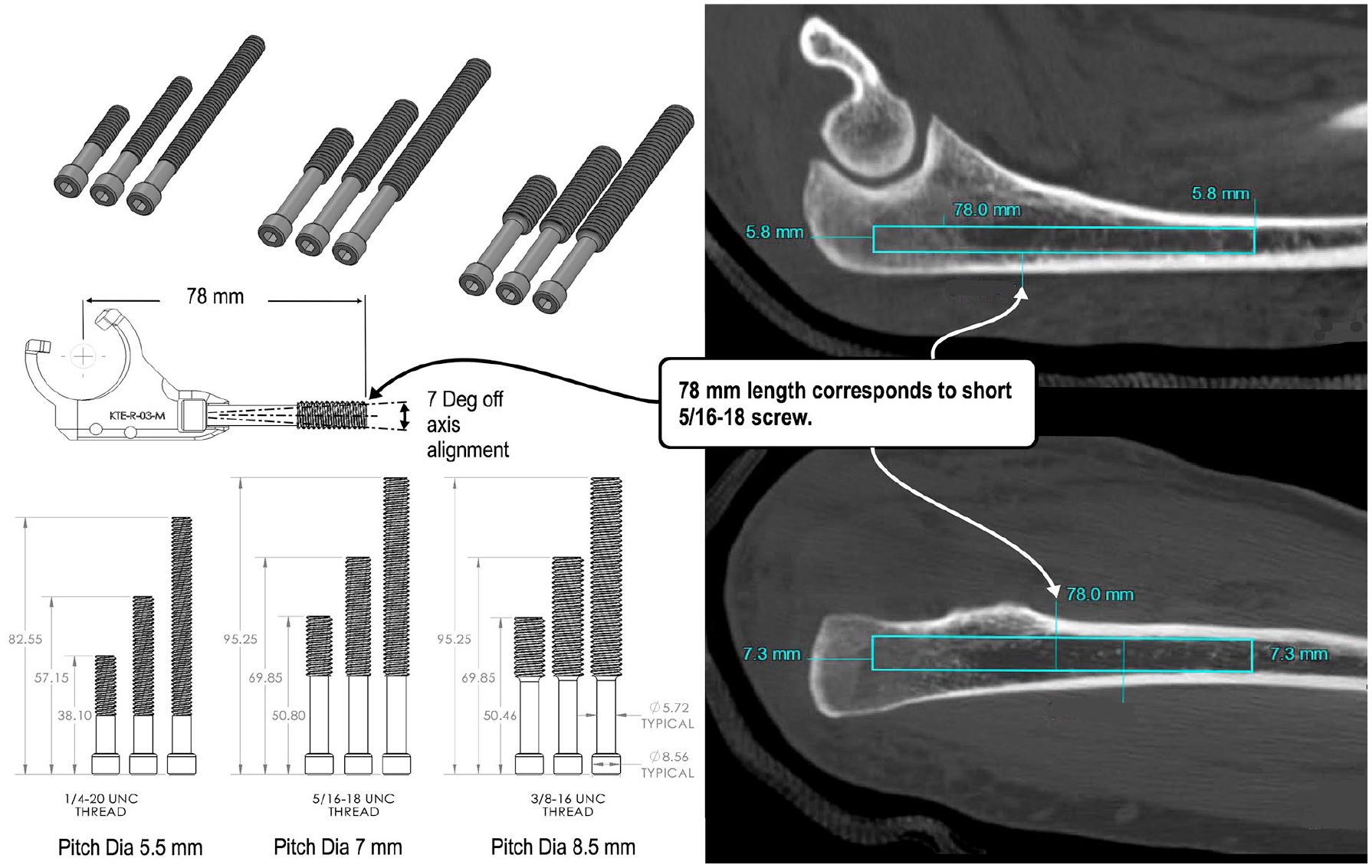
Templating intramedullary screw fixation, fixing length to 78 mm distal to the centerline of rotation and determining diameter. A 5/16-18 short length screw measures 78 mm when measured from the centerline of ulnohumeral rotation of a medium-sized ulnar body component to the end of the screw. A 7° wobbliness is designed into the connection between the implant body component and the intramedullary screw, which allows for off-axis alignment.
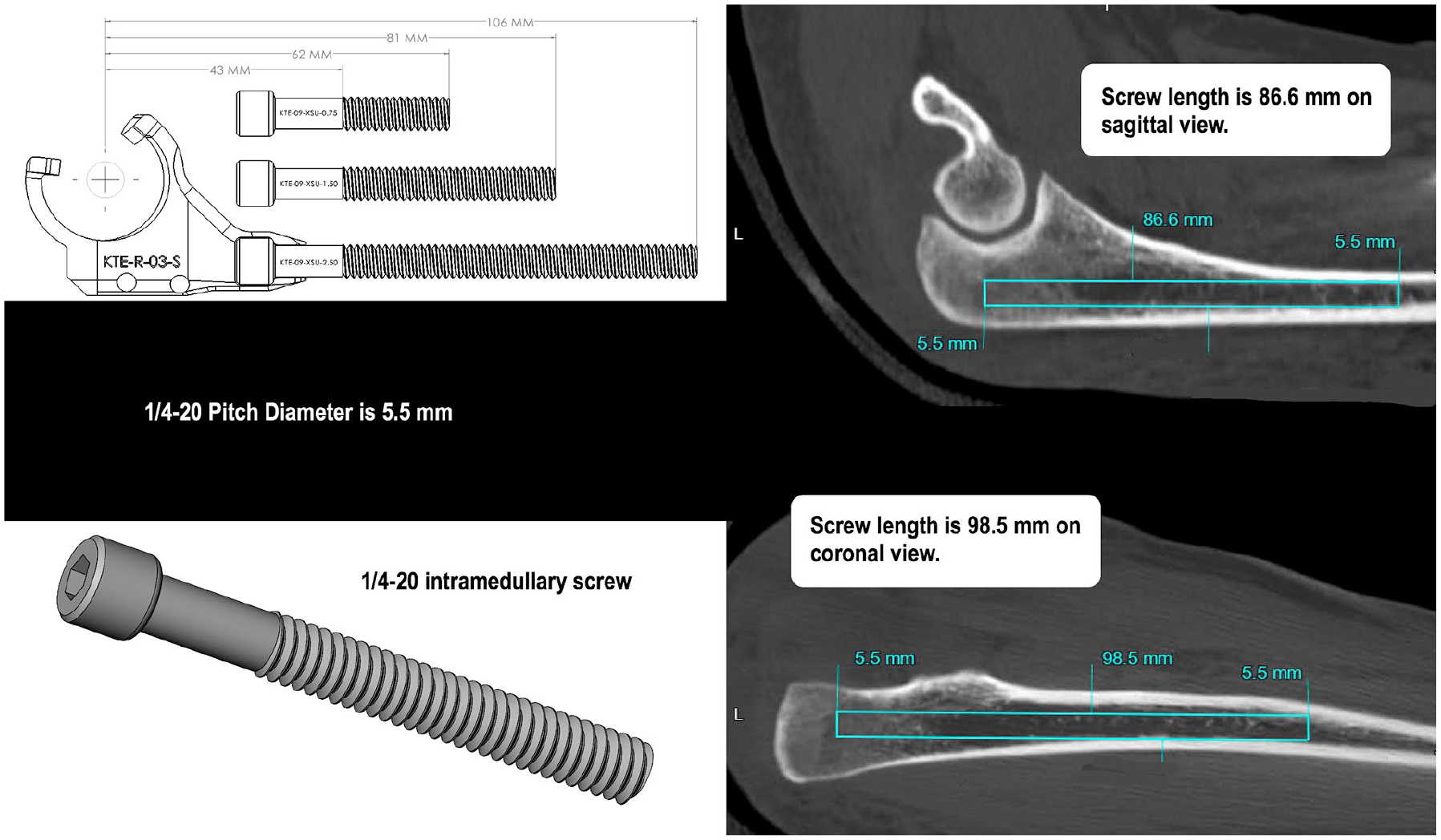
Templating intramedullary screw fixation, fixing diameter to 5.5 mm and measuring length. A 1/4-20 short length screw measures 62 mm when measured from the centerline of ulnohumeral rotation in a small ulnar body component to the end of the screw.
To validate the CT templating process, 5 patient-specific 3D models were generated from thinslice CT imaging using Mimics Medical (Materialise NV, Belgium) and then 3D printed with a Form 3 stereolithography 3D printer (Formlabs, Somerville, Massachusetts) using a clear, methacrylate-based resin. These 5 patients were randomly selected. Models were prepared, printed, and post-processed according to printer manufacturer specifications. Burr and broaches were used to create the opening within the proximal ulna to allow for screw passage within the intramedullary canal. The canal was subsequently drilled with a 5.1-mm drill bit and tapped with a 6.35-mm tap. A custom screw with 6.35 mm outer diameter and 5.5 mm pitch diameter was inserted as distal as possible until endosteal fit was achieved. Endosteal fit was determined once the screw could no longer be advanced by hand within the model. This depth was measured with relation to the centerline of rotation and compared with the templated depth determined on CT scans. Statistical analysis was performed using statistical software. Pearson correlation coefficient was calculated between depth of screw placement as templated by the CT scan and physical placement in the 3D models.
Results
A total of 30 patients’ CT scans were analyzed. The mean patient age at the time of CT scan was 45.5 years (range, 20-75 years). Sixteen patients (53.3%) were women. Indications for the CT scans included distal humerus fracture, coronoid tip fracture, radial head fracture, elbow instability, elbow mass, elbow infection, and nonspecific elbow pain. Of the patients for whom the 3D models were created, the mean patient age at the time of the CT scan was 55.2 years (range, 39-68 years), and 3 patients (60.0%) were women.
In determining the anatomic limits of intramedullary screw placement, a line drawn down the center of the intramedullary canal in the sagittal plane intersected the dorsal cortex in 11 patients (36.7%), at a mean of 99.6 mm distal to the centerline of rotation (Table 1). In the coronal plane, a line drawn down the center of the intramedullary canal intersected the lateral cortex in 26 patients (86.7%), at a mean of 95.0 mm distal to the centerline of rotation. All patients had an anatomic limit for intramedullary fixation, whether in the coronal plane, sagittal plane, or both.
Anatomic Limitation in Intramedullary Screw Placement.
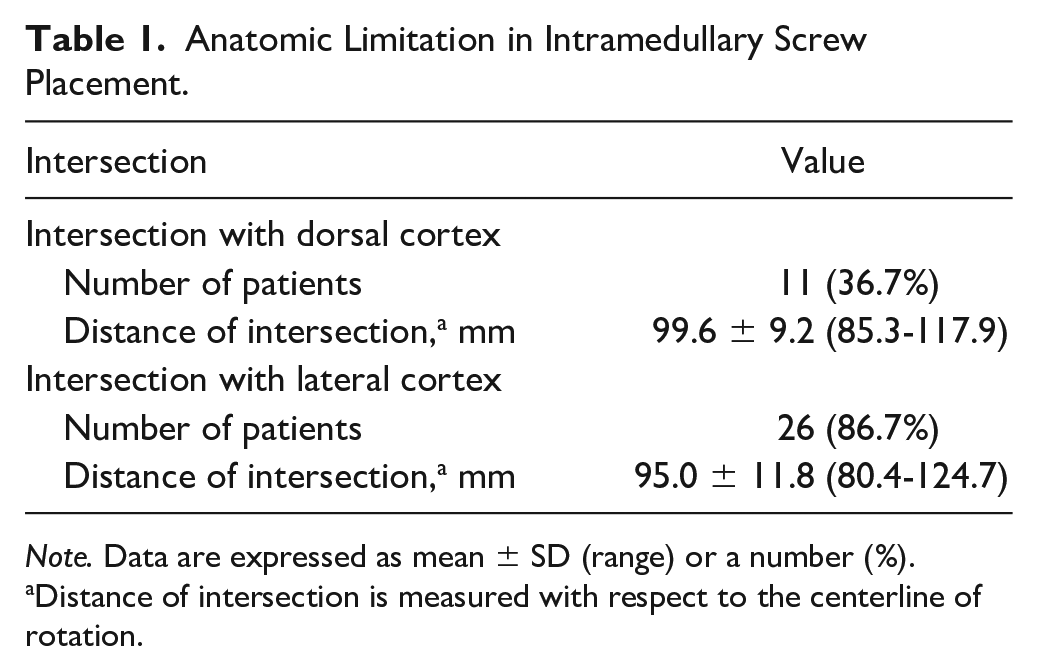
Note. Data are expressed as mean ± SD (range) or a number (%).
Distance of intersection is measured with respect to the centerline of rotation.
In templating screw placement and fixing the length to 78 mm distal to the centerline of rotation, the mean screw diameter was 5.4 ± 1.0 mm (range, 3.2-8) (Figure 4). In templating screw placement and fixing the screw diameter to 5.5 mm, the mean screw length was 79.9 ± 12.0 mm (range, 64.2-107.9) (Figure 4).
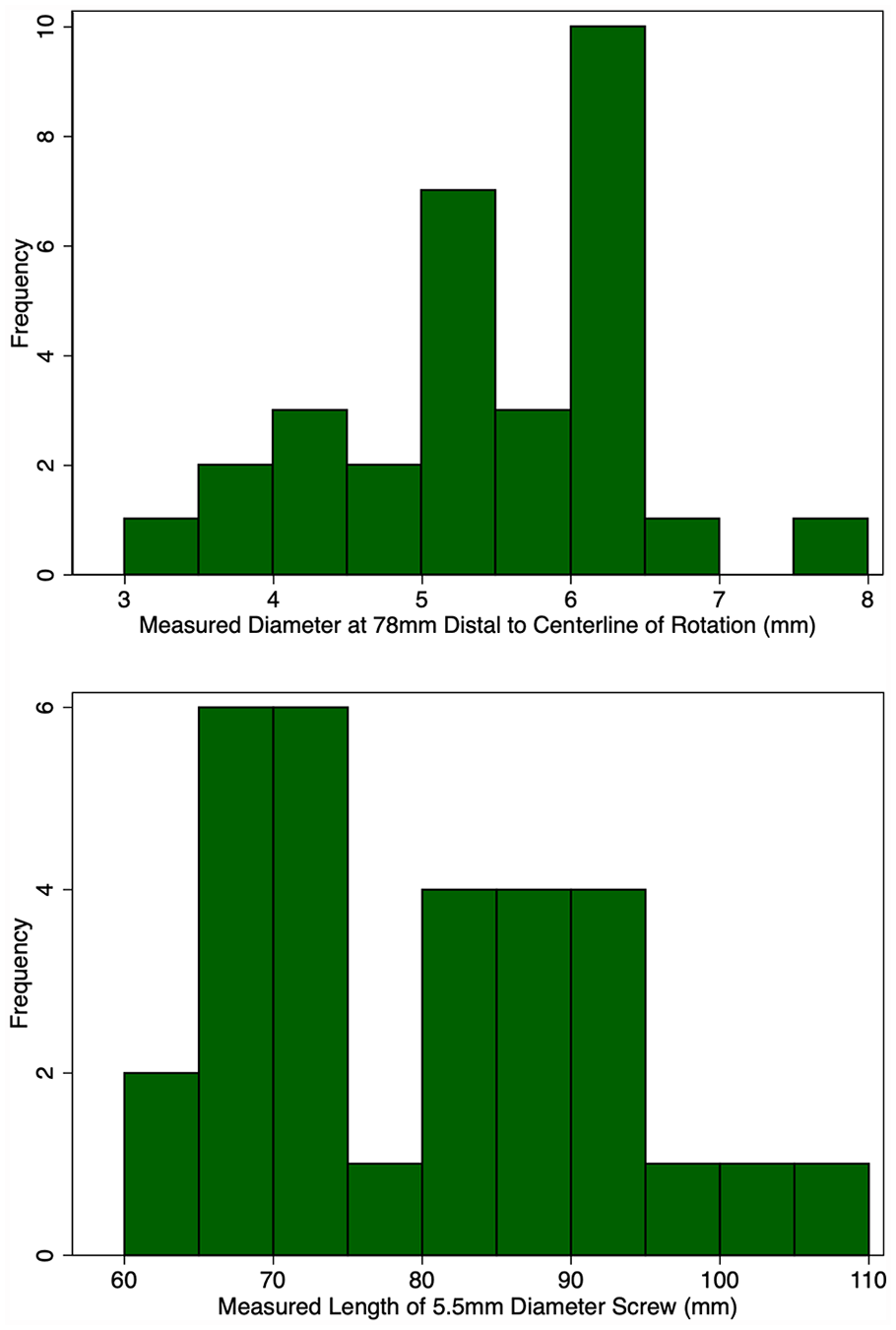
Screw templating, fixing length, and then fixing diameter.
When attempting to place the 6.35-mm custom screws (dimension of the 1/4-20 screw with 5.5 mm pitch diameter) in the five 3D-printed models, all screws were placed within 3 mm of the templated length (Table 2, Figure 5). The correlation coefficient between screw depth measured on CT and placed in 3D models was 0.992.
Depth of Screw Placement on CT Scan and in 3D Model (mm).
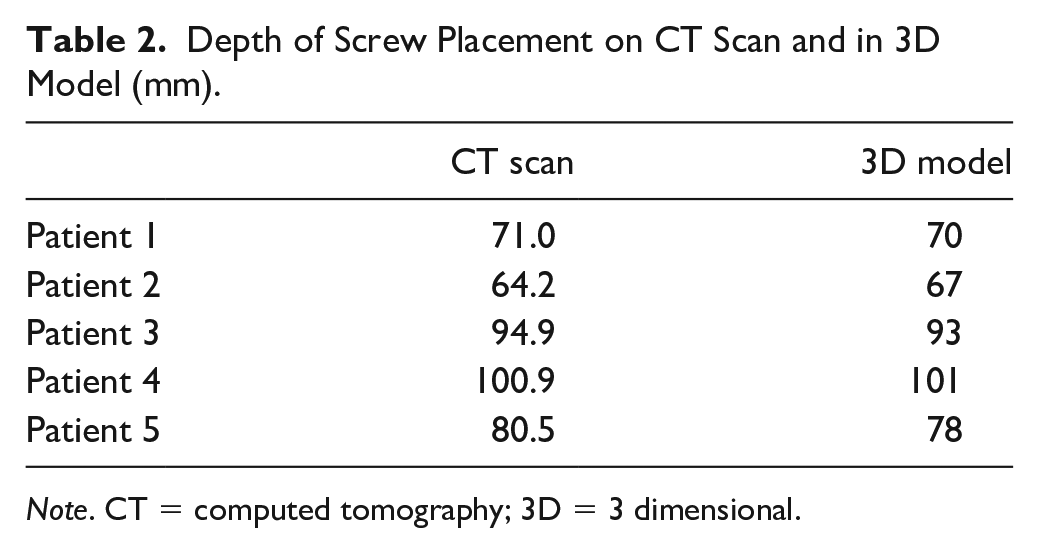
Note. CT = computed tomography; 3D = 3 dimensional.
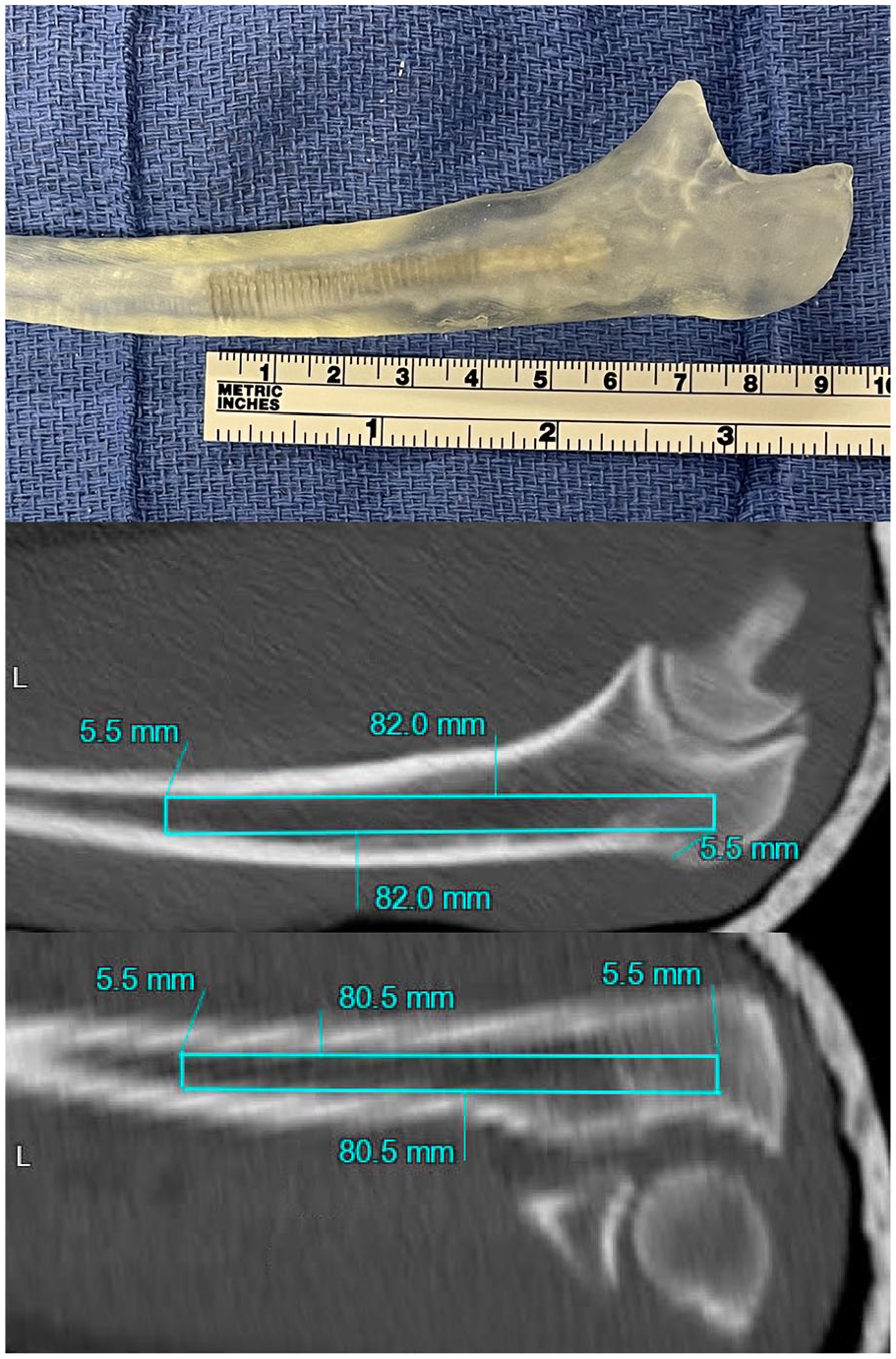
Templated screw on computed tomography scan and in 3-dimensional model.
Discussion
Intramedullary screw fixation of the proximal ulna has been used for olecranon fracture fixation and is the method of implant fixation for a novel total elbow arthroplasty system currently in development. Axial sections of the ulna have demonstrated that both the canal diameter and cortical thickness decrease distally in a uniform fashion, 1 and in this study, we sought to template intramedullary screw fixation to achieve a better understanding of proximal ulnar anatomy in the context of intramedullary screw fixation.
Regarding the proximal ulna dorsal angulation and varus angulation, we found that a line drawn along the intramedullary canal intersected with the dorsal cortex in 37% of patients at a mean of 99.6 mm distal to the centerline of rotation and with the lateral cortex in 87% of patients at a mean of 95.0 mm distal to the centerline of rotation. Wang et al 3 dissected 39 cadavers in an anatomic study, noting distance from the triceps insertion to the ulnar varus angle as 76 mm on average with a range of 65 to 90 mm. Hopf et al 2 analyzed 100 CT scans, and noted the proximal ulna dorsal angulation to have an apex located at 58.9 mm from the olecranon tip (range, 0-140.1 mm) and varus angulation apex at 47.8 mm from the olecranon tip (range, 23.7-71 mm). The location of the dorsal and varus angulation in these studies was determined to be much more proximal than our study. The reason for this difference is the method by which the location of the angulation was determined. In the previously mentioned studies, the point of angulation was determined from the outer cortex, drawing a line along the outer cortex on the proximal and distal segments and seeing where they intersected. Our study sought to define how far a line could be carried within the intramedullary canal until it hit a cortex. While this distance is affected by the overall angulation, it would be expected to be more distal within the canal than the outer apex as there is still room within the intramedullary canal beyond the outer apex.
Templating intramedullary screws showed variability, both when fixing screw length and fixing diameter. At 78 mm distal to the centerline of rotation, the mean screw diameter was 5.4 mm (range, 3.2-8). Fixing screw diameter to 5.5 mm, the mean screw length was 79.9 mm (range, 64.2-107.9). Wang et al 3 noted the mean intramedullary canal diameter at the ulnar angle level to be 7.1 mm in the medial-lateral direction and 7.4 mm in the dorsal-volar direction, with ranges of 4.2 to 12.5 mm and 5.0 to 12.4 mm, respectively. At 80 mm distal to the olecranon tip, Hopf et al 2 determined the median intramedullary canal diameter to be slightly above 6 mm with a range from just under 4 mm to just under 10 mm according to their boxplot diagram. Goldberg et al 1 dissected 27 cadavers and noted the ulnar intramedullary canal diameter 75 mm from the olecranon to be 7.5 mm (SD, 1.2) in male and 6.0 mm (SD, 1.0) in female patients. Of note, the above studies measured canal diameter at a point referenced from the olecranon, whereas in this study, we reference from the centerline of ulnohumeral rotation given its importance in total elbow arthroplasty. To place our measurements in the context of the literature, we determined the mean distance from the olecranon to the centerline of rotation to be 1.62 cm (range, 1.45-1.73 cm). Adding this measurement to the results referenced from the centerline of rotation allows for comparison with prior studies. Therefore, at a measurement of 94 mm distal to the olecranon, the mean screw diameter was 5.4 mm (range, 3.2-8). Our findings are similar to those of Hopf et al, 2 based on their boxplot diagram showing the median intramedullary canal diameter to be slightly below 6 mm between 90 and 100 mm distal to the olecranon. All studies demonstrate significant variability in the size of the intramedullary canal. The implication of this is that total elbow arthroplasty systems using intramedullary fixation should have a broad inventory of screw sizes to intraoperatively attain good endosteal fit.
In our 3D models, we were able to place 6.35 mm outer diameter screws (5.5 mm pitch diameter) within 3 mm of the templated length on CT scan based on a 5.5 mm measurement. We chose to template screws based on pitch diameter, anticipating that we would want screw threads to engage the inner cortex to provide a good bone purchase.
This study has several limitations. An initial source of error is that the centerline of the intramedullary canal is determined by the operator based on 2-dimensional coronal and sagittal planes. This approach is only valid if one assumes that the centerlines are generally colinear, which presupposes that the intramedullary canal is circular. Although the canal is not truly circular in its cross section, 2 studies that characterizes the anatomy of this canal measured its circular diameter.1,2
Another limitation is the use of 3D-printed models rather than actual bone. Although we were able to insert all screws within 3 mm of the templated length, it is possible that actual bone, especially in rheumatoid or osteoporotic patients, may be weaker than this resin, which may have led to bone fracture once the templated length was achieved. The methacrylate-based material that was used for templating has been validated for effectively simulating the drilling of bone. 12 Another limitation stems from the fact that we had analyzed CT scans of elbows rather than CT forearms. This image typically truncated the ulna near the middle or proximal third of the ulna. In all cases, there was enough of the ulna visualized to template appropriate screws for this study, but it is possible that more patients had an anatomic limit to intramedullary screw placement than was found if that anatomic limit was more distal. However, we found all patients to have some sort of anatomic limit, whether in the coronal plane, sagittal plane, or both. Accordingly, the potential error of having a secondary anatomic limit more distal would not necessarily have a clinical implication in the context of this study. Another limitation is that only 5 CT scan–based 3D-printed models were used, and, yet, the templated screws were all placed within 3 mm of the templated size, and additional specimens would likely not have changed our findings. Although we randomly chose the CT scans to make a model, we did have knowledge of what screw we had templated, which may have led to bias regarding the placement of this screw into the printed CT scan model. Consistent implantation steps were followed that employed custom-designed smooth drill bits that engage the intramedullary canal in a nonaggressive manner, which makes it difficult to force a drill bit into the canal of rigid methacrylate resin. 12 Another source of error is that the 3D-printed models were only visually inspected after axial screw placement was measured and not imaged or sectioned to determine wall thickness surrounding the screw. No perforation was identified and, yet, thin cortical walls may have been present, which can lead to a stress riser or fracture.
This study characterized proximal ulna anatomy in the context of intramedullary screw fixation. Each patient had an anatomic limit for intramedullary fixation, either due to the varus or dorsal bow, or both. At 78 mm distal to the centerline of rotation, the mean screw diameter was 5.4 mm (range, 3.2-8). In templating screw placement and fixing the screw diameter to 5.5 mm, the mean screw length was 79.9 mm (range, 64.2-107.9). Surgeons should have access to a broad inventory in attempting intramedullary fixation of the proximal ulna.
Supplemental Material
sj-docx-1-han-10.1177_15589447231184894 – Supplemental material for Computed Tomography–Based Templating of Proximal Ulna Intramedullary Screw Fixation
Supplemental material, sj-docx-1-han-10.1177_15589447231184894 for Computed Tomography–Based Templating of Proximal Ulna Intramedullary Screw Fixation by Nitin Goyal, Dominic Coutinho, Anish Ghodadra, Mark E. Baratz and Robert A. Kaufmann in HAND
Supplemental Material
sj-jpg-2-han-10.1177_15589447231184894 – Supplemental material for Computed Tomography–Based Templating of Proximal Ulna Intramedullary Screw Fixation
Supplemental material, sj-jpg-2-han-10.1177_15589447231184894 for Computed Tomography–Based Templating of Proximal Ulna Intramedullary Screw Fixation by Nitin Goyal, Dominic Coutinho, Anish Ghodadra, Mark E. Baratz and Robert A. Kaufmann in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
The institutional review board approved a waiver of informed consent.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A.K. is the owner of Arrch Orthopedics. Arrch is developing a novel total elbow arthroplasty.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.