
Abstract
Background:
There is increased interest in ultrasound (US) for the diagnosis of cubital tunnel syndrome (CuTS). We hypothesize that ulnar nerve cross-sectional area (CSA) correlates with disease severity and electrodiagnostic studies (EDX).
Methods:
ARetrospective review was performed at a tertiary medical center. One hundred seventeen patients (166 ulnar nerves) were evaluated. Maximum CSA at 3 points around the elbow (proximal, groove, and distal) and EDX results (American Board of Electrodiagnostic Medicine-certified physiatrist’s interpretations) were collected.
Results:
US was positive (CSA > 0.1 cm2) in 95/117 cases (81.20%) versus 84/117 (71.79%) positive for EDX. CuTS patients treated surgically had significantly greater (0.13 cm2, standard deviation [SD] 0.038) preoperative CSA than non-operative patients (0.10 cm2, SD 0.033) (p = .003). CSA increased as EDX increased in severity; mild (0.116 cm2, SD 0.031), moderate (0.121 cm2, SD 0.035), and severe (0.163 cm2, SD 0.047) with a significant difference between the mild and severe groups (P = .001) and between the moderate and severe groups (p = .01). Significant differences were seen between patients with positive US and EDX studies compared to those with negative US and EDX in the average physical function scores (57.26, SD 8.57 versus 43.18, SD 7.70; p < .001); average sleep scores (50.14, SD 9.53 versus 56.62, SD 7.31; p = .02); average physical function scores (43.04, SD 8.68 versus 57.08, SD 6.34; p < .001) and average depression scores (49.10, SD 10.88 versus 45.043, SD 7.06; p = .02).
Conclusions:
US is a reliable tool for diagnosis and surgical decision-making for CuTS.
Type of Study/Level of Evidence:
Diagnostic/III.
Keywords
Introduction
Cubital tunnel syndrome (CuTS) or ulnar nerve entrapment (UNE) is the second most common nerve compression syndrome behind carpal tunnel syndrome. In 2013, there were roughly 72 000 cases a year in the United States, 1 with more recent studies suggesting that these numbers may be even higher with nearly equal prevalence to carpal tunnel syndrome. 2 Furthermore, the rate of surgical management of CuTS has increased in the United States and even doubled in Britain from 31% to 67% in the past few years. 1
The current gold standard methods used for upper-extremity compressive neuropathy diagnosis are nerve conduction studies (NCS) and electromyography (EMG). However, the specificity and sensitivity of NCS and EMG in the diagnosis of CuTS, in particular, have been notoriously poor. While the sensitivity of NCS for carpal tunnel syndrome is around 85% to 90%,3,4 the sensitivity of electrodiagnostic testing for UNE has been found to range from 37% to 86%, 5 making NCS far from an ideal diagnostic tool. It is subject to variable technique and diagnostic thresholds, which might contribute to the problem, while the choice of sites for measuring nerve conduction as well as differential techniques for attaining values (the choice of using abductor digiti minimi, first dorsal interosseous, or both) may influence the sensitivity. In addition, even though the American Association of Electrodiagnostic Medicine offers a set of values to set thresholds around, individual practices may use more- or less-stringent criteria. 6
Given the issues associated with electrodiagnostic testing, there has been an increased interest in exploring other diagnostic modalities for UNE. A recent meta-analysis of the United States for carpal tunnel syndrome showed that ultrasound (US) appeared to be a good alternative for diagnosis with high sensitivity and specificity. 7 This catalyzed interest in exploiting this modality in the diagnosis of CuTS as well, which can now be imaged with excellent resolution. Ultrasound has potential as a sensitive and specific modality in detecting UNE while having a lower patient impact profile, being both painless and noninvasive. In addition, US is more likely to reveal the site of compression, as well as potential anatomic pathology causing UNE, such as a muscle, ganglion, and nerve dislocation, 8 which currently cannot be determined by electrodiagnostic studies (EDX). The purpose of this study is to determine the agreement of EDX and US in the diagnosis of UNE and to elucidate the correlations of each diagnostic modality with patients’ symptoms.
Materials and Methods
Institutional review board approval was obtained prior to the initiation of this study. A retrospective review of patients presenting to a single tertiary academic medical center with symptoms of CuTS between January 1, 2018, and January 1, 2022, was performed. Patients were identified by International Classification of Diseases, Tenth Revision, codes for ulnar neuropathy (G56.21, G56.22, and G56.20) and Current Procedural Terminology codes (76882) for EDX and US evaluation. Only patients that had both EDX and US measurements of the affected ulnar nerve were included, whereas patients with traumatic injury resulting in neuropathy or undergoing revision surgery were excluded.
The maximum cross-sectional area (CSA) at 3 standardized points around the elbow (proximal [3 cm proximal], groove, distal [3 cm distal]) was measured (Figure 1). The maximum CSA was determined by an American Board of Electrodiagnostic Medicine (ABEM)-certified physiatrist using previously described methodology and the widely accepted cutoff of 10 cm2 to define CuTS. 9 In addition, EDX results (ABEM-certified physiatrist’s interpretations), patient-reported outcome score measures (PROMIS), and surgical intervention were noted for each subject. Patient-reported outcome measures data were collected for the following variables: upper-extremity score, anxiety score, sleep disturbance score, pain interference score, and depression score.
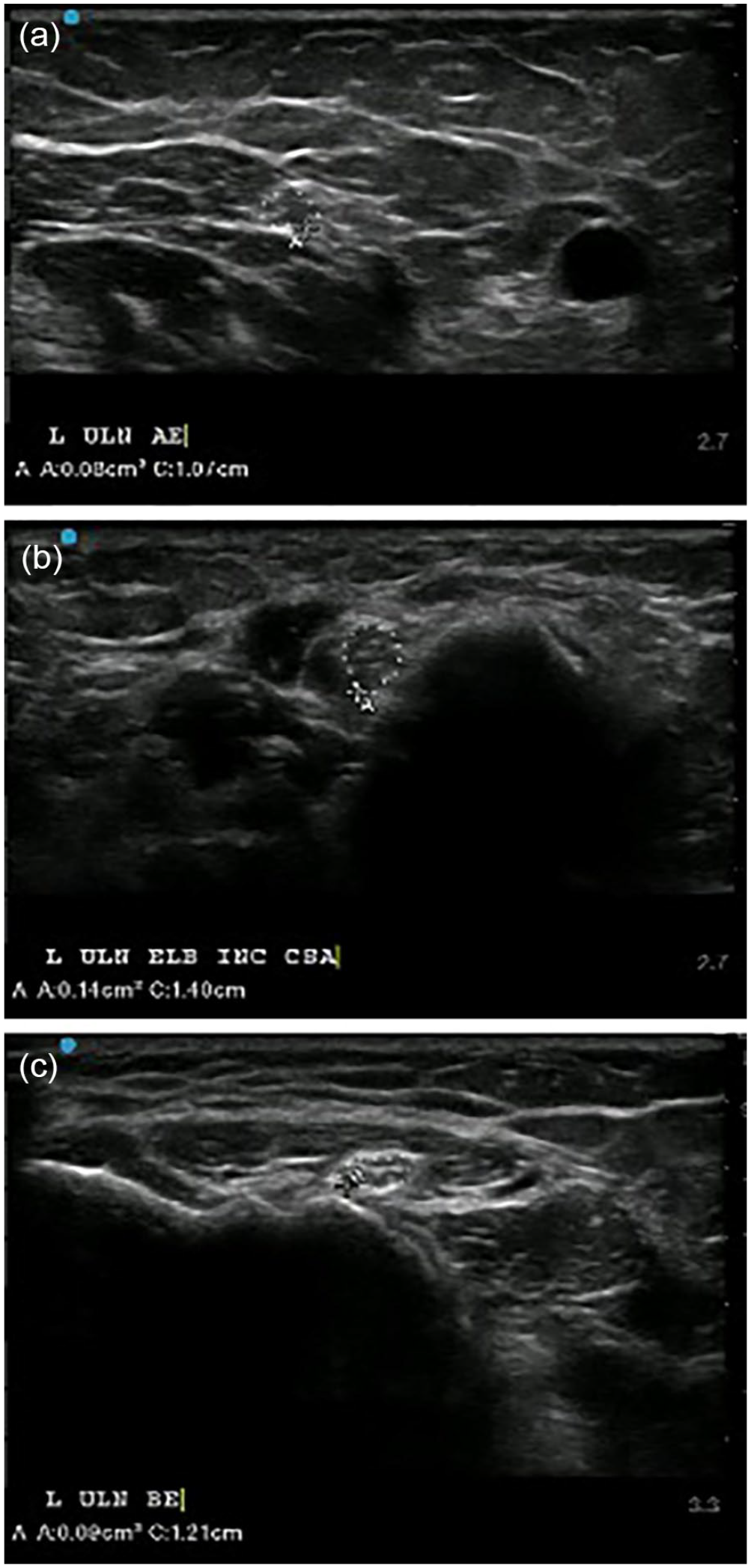
Ulnar nerve ultrasound of a patient with cubital tunnel syndrome. (a) UN proximal to the elbow (3 cm proximal), (b) at the elbow, and (c) distal to the elbow (3 cm distal).
The maximum CSA value was then compared with the aforementioned PROMIS scores. Each PROMIS category was compared with maximum CSA values, and correlation coefficients were generated for each subcategory as it related to the CSA value. Patient-reported outcome measures data were also analyzed between patients with positive versus negative US, patients with positive versus negative EDX, and patients with positive US versus positive EDX. Continuous data were calculated using nonpaired t-tests. The agreement between testing modalities (EDX and CSA) and the location of maximum CSA (proximal, groove, distal) were evaluated.
Finally, EDX results and their corresponding maximum CSA on US were categorized into mild, moderate, and severe based on the interpretation of an ABEM-certified physiatrist from a single group in a university practice. The 3 groups were compared using nonpaired t-tests between mild versus moderate, moderate versus severe, and mild versus severe.
Results
A total of 120 patients were initially identified as having EDX; US and PROMIS data available. After exclusion criteria were applied, 117 patients (166 ulnar nerves) were evaluated. Patient characteristics are listed in Table 1. In patients with a clinical diagnosis of CuTS, ulnar nerve US was positive (CSA > 0.1 cm2) in 95 of 117 cases (81.20%) compared with 84 of 117 (71.79%) who were positive by EDX. Agreement of EDX and US in diagnosing UNE was present in 64 of 117 cases (54.7%) (mild 78.78%, moderate 88.24%, and severe 100% agreement when separated by EMG severity). The maximal CSA was most often observed at the ulnar groove (65.1%) compared with the proximal (12.6%) or distal (22.3%) sites. Patients with CuTS who went on to have cubital tunnel release had significantly greater (0.13 cm2, SD 0.038) preoperative CSA than patients who did not (0.10 cm2, SD 0.033) (P = .003) (Figure 2). Of the operative group, 96.96% had positive US versus 67.65% that had positive EMG. The CSA increased in size as EDX increased in severity; mild (0.116 cm2, SD 0.031), moderate (0.121 cm2, SD 0.035), and severe (0.163 cm2, SD 0.047), and there was a significant difference in nerve CSA between the mild and severe groups (P = .001) and the moderate and severe groups (P = .01) (Figure 3). No statistical difference was observed between the mild and moderate groups (P = .66).
Patient Characteristics.
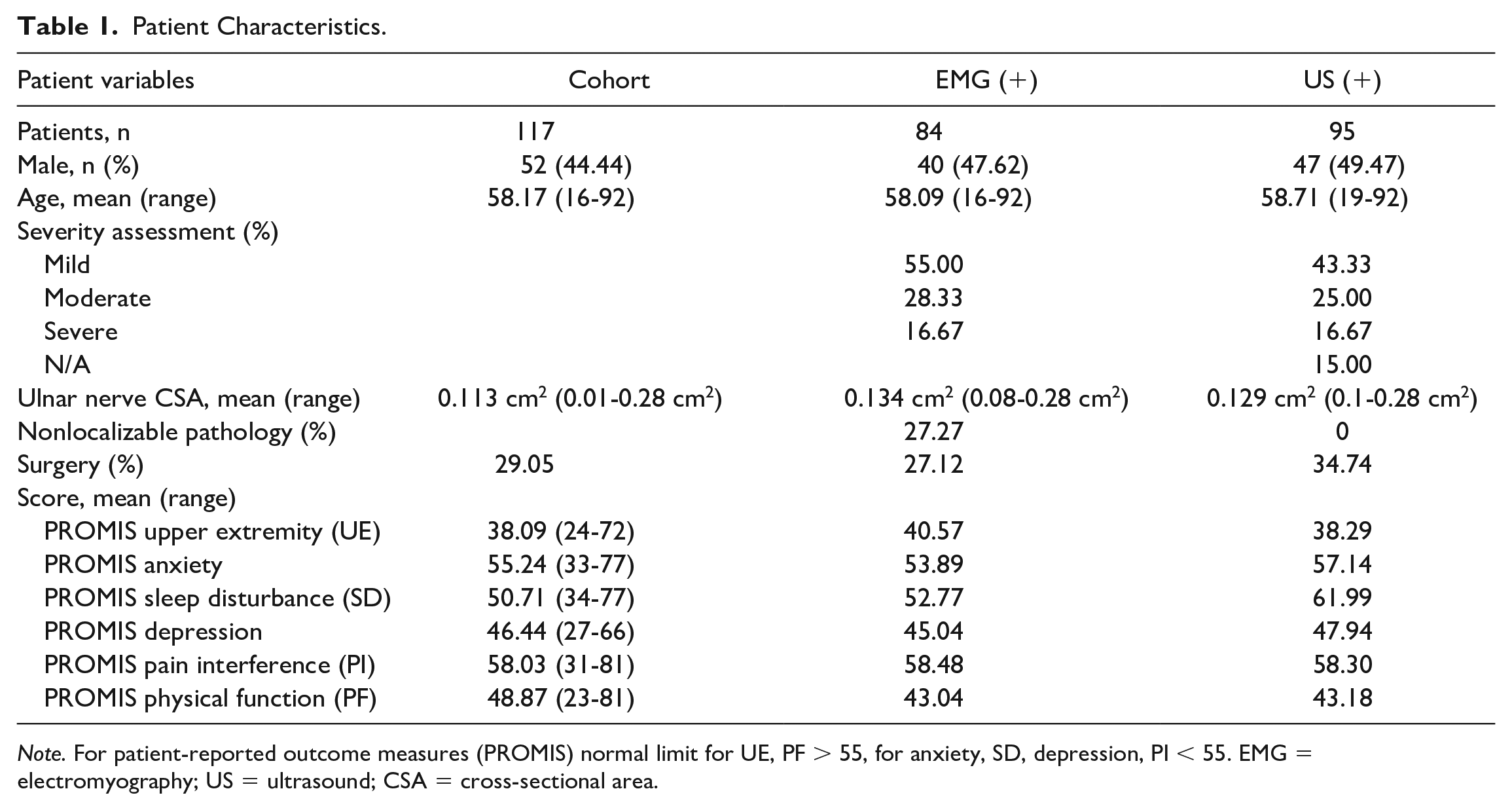
Note. For patient-reported outcome measures (PROMIS) normal limit for UE, PF > 55, for anxiety, SD, depression, PI < 55. EMG = electromyography; US = ultrasound; CSA = cross-sectional area.
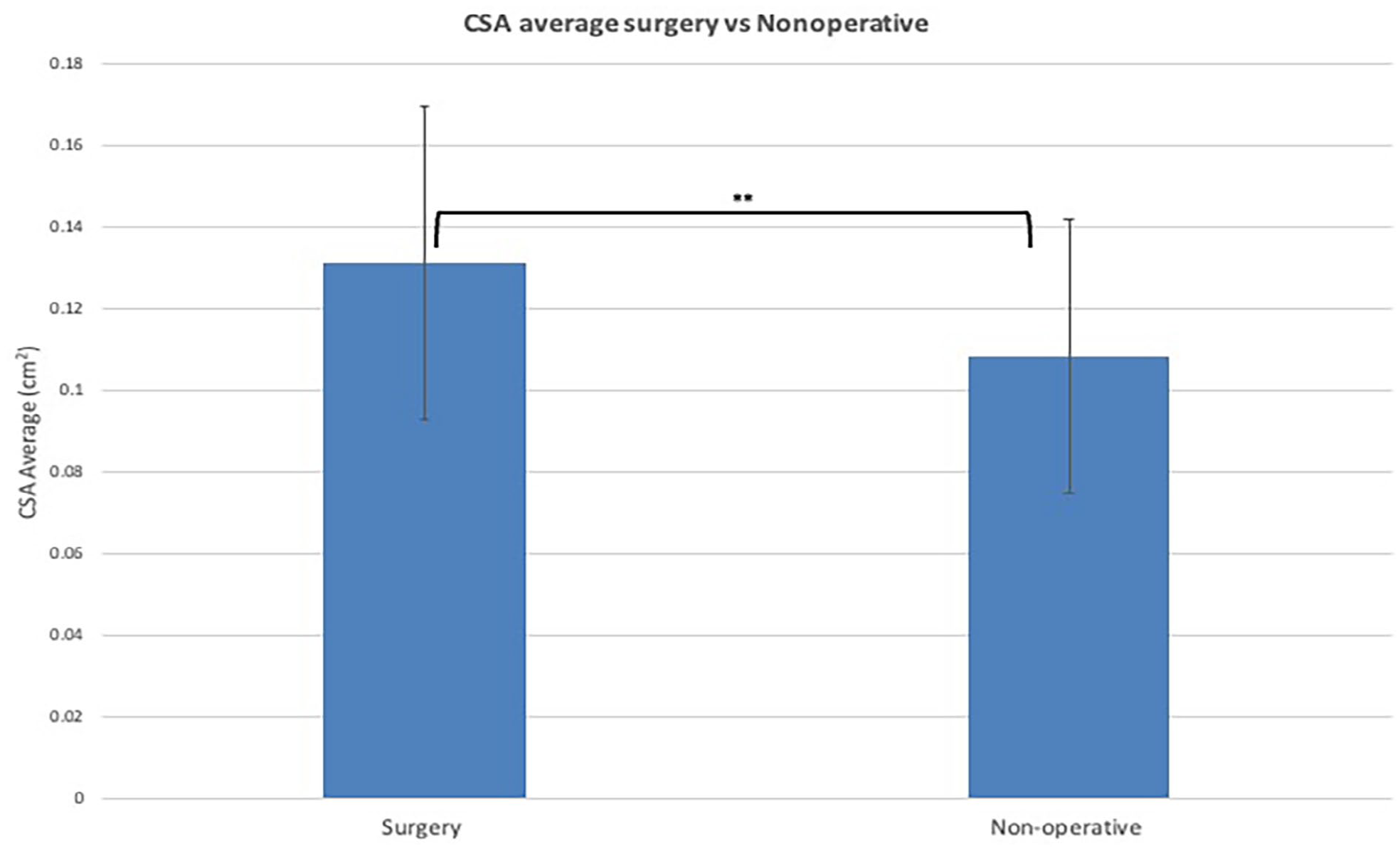
CSA average in operative versus nonoperative patients.
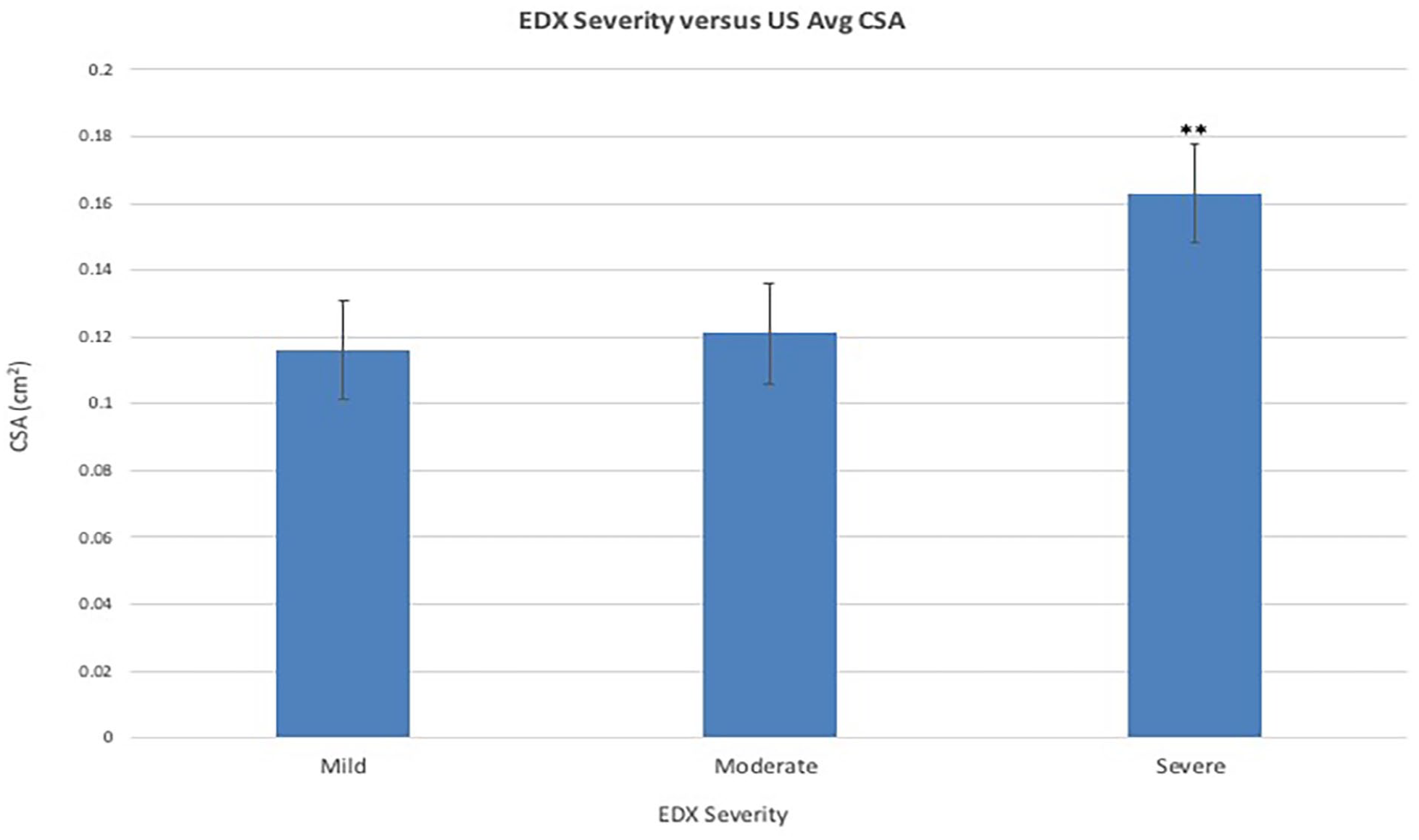
EDX severity versus average US CSA: Bonferroni P value correction .017.
There were no statistically significant differences in the average PROMIS scores of patients diagnosed based on CSA versus EDX. However, within each testing modality subgroup, there was a significant difference in the average physical function scores (57.26 [SD 8.57] vs 43.18 [SD 7.70]; P < .001) and average sleep scores (50.14 [SD 9.53] vs 56.62 [SD 7.31]; P = .02) in patients with positive versus negative US (Figure 4). In addition, there were significant differences in average physical function scores (43.04 [SD 8.68] vs 57.08 [SD 6.34]; P < .001) and average depression scores (49.10 [SD 10.88] vs 45.043 [SD 7.06]; P = .02) in patients with positive versus negative EDX studies (Figure 5). Finally, of the 117 patients analyzed, 25 patients (21.36%) had abnormal EDX studies with a nonlocalizable site of compression that were all successfully identified by US. The average CSA in this group of patients was 0.135 cm2.
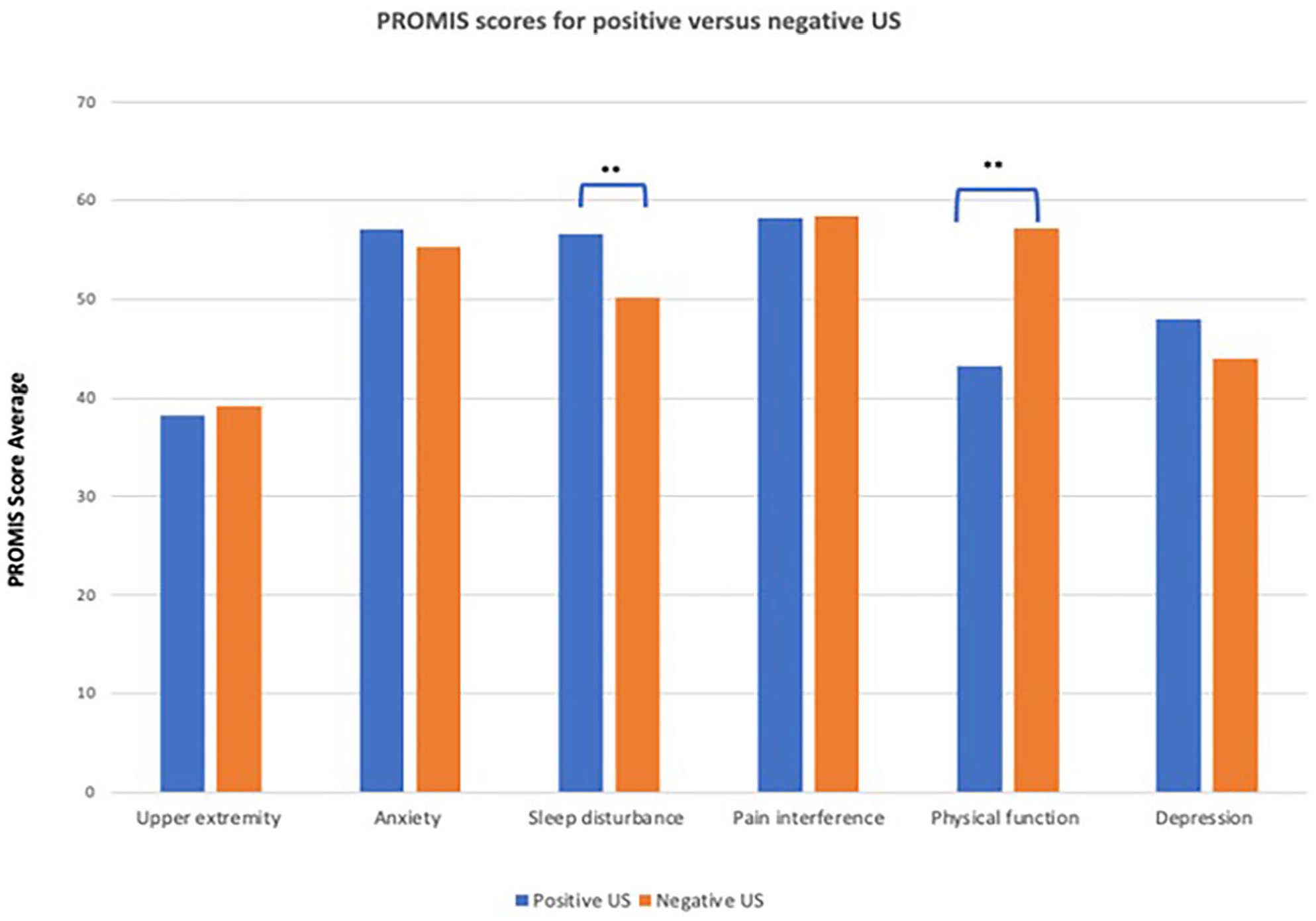
PROMIS scores for positive versus negative US. Normal limits listed for each category.
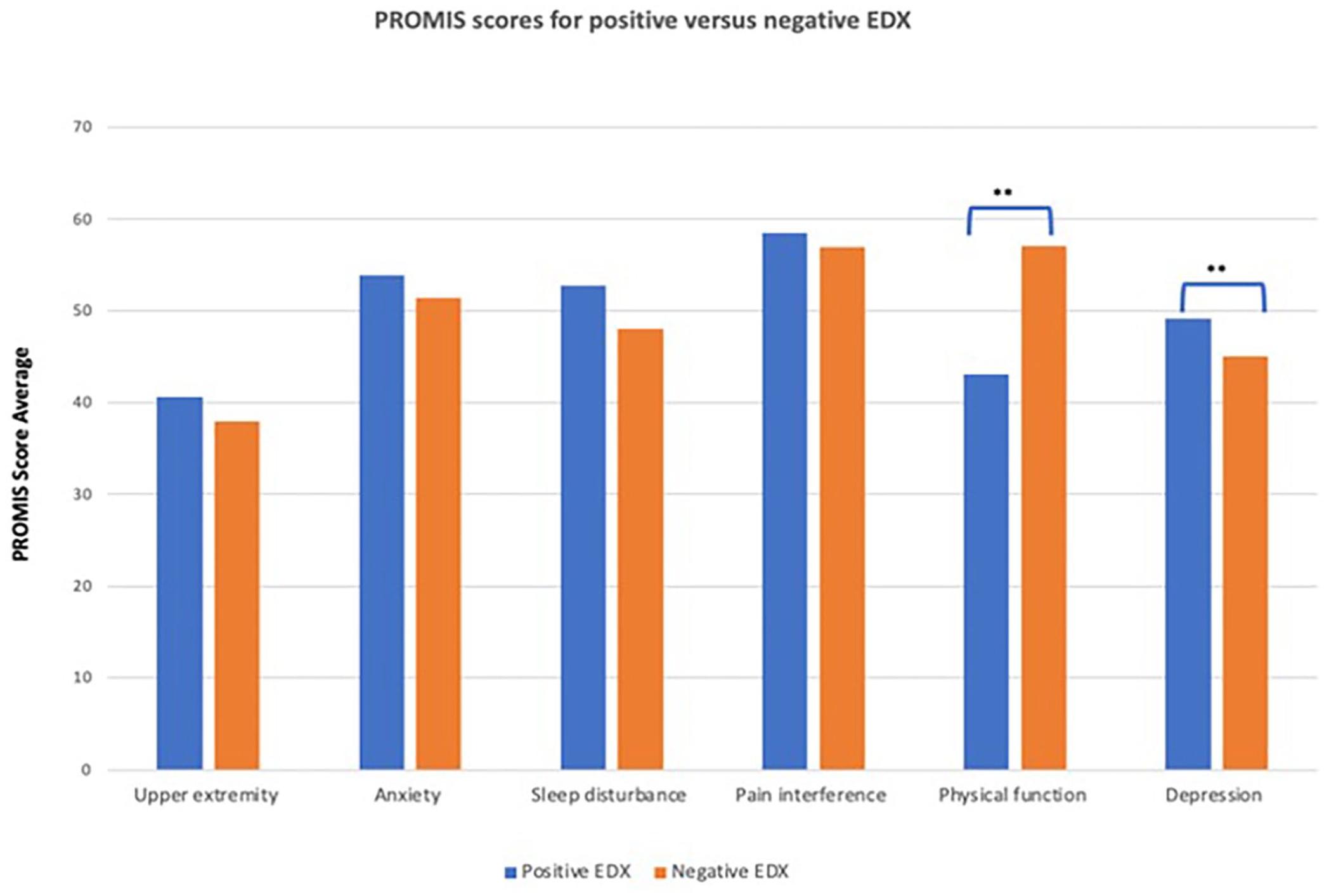
PROMIS scores for positive versus negative EDX. Normal limits listed for each category.
Discussion
Compressive neuropathy of the upper extremity is an extremely pervasive clinical entity that is steadily becoming more prevalent. 10 It is therefore crucial to have reliable, efficient, and accurate diagnostic modalities for the common compressive neuropathies: median nerve compression (carpal tunnel syndrome) and ulnar neuropathy (CuTS). Even though the sensitivity of EDX, the current gold standard, for carpal tunnel syndrome is reported to range from 80% to 90%, 4 the sensitivity for UNE has been found to range from 37% to 86%, 5 which remains suboptimal. There is extensive literature demonstrating the value of US in carpal tunnel syndrome; however, there is a relative dearth of data regarding its utility in the diagnosis of UNE.
In our cohort of patients that presented with CuTS, US was positive (>0.10 cm2) in 89% of cases compared with 51% that were positive by EDX, with US and EDX congruent in diagnosing UNE in 64 of 117 cases (54.7%). Forty-one of the patients had a positive US and negative EMG. Of these, 11 underwent ulnar nerve decompression with an average CSA of 0.127 cm2 (range 0.10-0.18 cm2), and 30 were treated conservatively with an average CSA of 0.117 cm2 (range 0.06-0.17 cm2). Given that these are all patients that presented with clinical symptoms consistent with CuTS and were indicated for EDX/US testing, US appears to have better agreement with the clinical diagnosis than EDX. Overall, 9.4% of the total cohort were patients undergoing surgery based on a clinical diagnosis supported by US with negative EDX, indicating that US may have a higher sensitivity and the potential of identifying surgical candidates that EDX may fail to diagnose. On the other hand, 11 patients with a negative US had a positive EMG. The average CSA in this group was 0.074 cm2 (0.06-0.09 cm2), with 9 of these patients characterized as having mild and 2 as moderate ulnar neuropathy. Only one patient underwent surgery with a positive EMG and negative US, but interestingly, this was a patient with only mild neuropathy.
Across the whole cohort, CSA of the ulnar nerve increased with increasing EDX severity. The average CSA in our study was 0.11 cm2, which is consistent with previously reported CSA in patients with CuTS due to upstream ulnar nerve swelling.11-14 Letissier et al 15 in a study of 50 patients (100 ulnar nerves) found 0.10 cm2 as the upper limit of normal for the CSA of a nonpathologic ulnar nerve, which is in line with what was found in our cohort. The ulnar groove was most commonly the point of maximal nerve CSA, which was also previously demonstrated by Beekman et al 16 in their cohort of 102 patients with ulnar neuropathy. 1
Patients who went on to have surgery had a significantly greater CSA than patients treated nonoperatively, indicating that US may better correlate with severity of symptoms and subsequent decision for surgery. The average CSA of patients who underwent ulnar nerve release was 0.131 cm2 (range 0.11-0.28 cm2, SD 0.38 cm2), whereas the average of the nonoperative group was 0.108 cm2 (range 0.07-0.17 cm2, SD 0.33 cm2). Of those with a positive US that underwent release, 32.35% had negative EDX, indicating that there is a subgroup of patients that are electrodiagnostically negative with severe enough clinical symptoms to be indicated for surgery and can be objectively diagnosed by the increased CSA. In comparison, in the same cohort of patients who underwent release, 2.9% had a positive EMG and negative US. Overall 34.74% of the patients who were US positive went on to surgery versus 27.12% of patients who were EMG positive. Of the total number of people who went on to have surgery, 96.96% had a positive US versus 67.65% with a positive EMG (Table 1). These data may support that US could be the preferred modality as an indicator of patients’ experience of symptoms and eventual progression to surgery.
Overall, US has a number of potential advantages over EDX. While EDX remains the gold standard, obtaining the study can be painful and more time-consuming than US.17-20 It also requires a separate visit with a physiatrist, which might delay diagnosis and time to treatment. Given its portability, US can potentially also be used as a point-of-care testing modality. Not only is US accessible, but Garcia-Santibanez et al 21 demonstrated that providers can achieve high levels of interrater reliability with approximately only 2 months of training. Decreasing the number of visits and time to diagnosis can also mean decreased health care costs and time away from work. Perhaps, however, one of the most valuable advantages of US is the ability to identify the specific location of the affected nerve especially when EDX fails to localize the pathology. 15 This was exemplified in our study since about 20% of our patients fell in this category, all of which were successfully localized by US. Identification of the exact sites of compression can be vital in guiding surgical decision-making and in ensuring that the appropriate sites are decompressed.
Finally, patients with a positive US or positive EMG were found to have significantly worse scores in physical function, which could reflect the patients’ symptoms of weak grip, clumsiness, and difficulty manipulating objects. Sleep and depression measures were also significantly worse in patients with positive US and EMG, respectively. Early CuTS symptoms are known to get worse at night since many patients tend to sleep with their elbows bent while the fluid is redistributed without an active muscle pump, resulting in sleep disruption.22,23 More severe CuTS can not only disrupt sleep but also become disabling and contribute to depression. Importantly, there was no significant difference in patient reported outcomes in patients with positive US versus positive EDX.
In summary, US is a viable modality for the diagnosis of UNE, and it is an important compliment to EDX. Increased CSA on US may be more sensitive in detecting patients with early CuTS and shows good correlation to patients that may eventually necessitate surgical release. Ultrasonography is noninvasive and less painful for patients than EDX and can be performed in the clinic. It also has the ability to potentially localize the point of compression when EDX yields nonlocalizable pathology, and the degree of the nerve enlargement can also provide information on the severity of compression. More studies are needed to further define the role of US in the diagnosis of UNE as this has the potential to detect earlier pathology, shorten the length of time to treatment, decrease the number of office visits, and improve patient satisfaction.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was waived due to this study being a retrospective chart review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.