
Abstract
Background:
While complexity of distal radius fractures varies, volar plating is the most prevalent surgical option in adult injuries. The time between date of injury and surgical intervention varies according to several factors, including the timing of presentation and the surgeon’s availability. This study aims to understand the impact of a delay in surgical intervention on operative time, patient-reported outcomes, and reoperation rates.
Methods:
A retrospective review was performed on patients treated with volar plating of distal radius fractures from 2017 to 2020 at a single institution by multiple surgeons. Perioperative medical records were reviewed. Patients were divided into 2 groups using a cut-off date of surgery performed 12 days after injury. Descriptive analyses were used to compare demographics, fracture characteristics, operative information, and outcome data including postoperative Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores and reoperation rates between groups.
Results:
A total of 257 patients were included. There was no difference in age, gender, smoking status, fracture type, or postoperative QuickDASH scores between groups. Patients fixed at 12 days or more after injury had a higher rate of reoperation, higher American Society of Anesthesiologists scores, and more surgeon experience.
Conclusions:
Volar distal radius fixation at 12 or more days after injury had no discernible differences with fracture type, operative time, or tourniquet time; however, a higher rate of reoperation was found in this group compared to earlier intervention. These data may provide important prognostic information that can be used to educate patients who present in a delayed fashion.
Keywords
Introduction
Distal radius fractures are considered one of the most common orthopedic injuries, accounting for an estimated 17% of long bone fractures seen in the emergency room setting.1 -3 Volar plating has become the most prevalent surgical technique implemented in adult injuries and can be used in a variety of fracture patterns. 3 When considering treatment of these injuries, the time between the date of injury and surgery varies significantly among patients for a variety of reasons such as patient factors, timing of presentation, and operative availability. 4 Issues related to required testing and vaccination status for COVID-19 may also create delays in outpatient evaluation and surgical scheduling. 5 Despite limited evidence in the literature regarding timing and operative fixation of these fractures, prior studies have demonstrated that delayed surgery may affect surgical difficulty and quality of reduction, postoperative motion, and functional outcomes.4,6,7
Overall, there is a paucity in the literature and limited consensus regarding the timing of volar plating of distal radius fractures and its effect on patient outcomes. This study aims to evaluate the impact of a delayed surgical intervention on operative time, tourniquet time, patient-reported outcomes, and incidence of reoperation in patients with both intra-articular and extra-articular fractures of the distal radius. We hypothesized that delayed surgical fixation would be associated with increased operative and tourniquet time and an increased rate of reoperations.
Materials and Methods
Patients above 18 years of age who underwent open reduction and internal fixation (ORIF) with a volar locking plate for distal radius fractures at a single, academic medical center from 2017 to 2020 were identified. All procedures were performed by fellowship-trained orthopedic hand surgeons. Patients were excluded if they had open fractures, insufficient data for chart review, lack of a postoperative follow-up visit, or treatment by means other than a volar distal radius locking plate. All patients were offered formal physical therapy by a certified hand therapist following surgery.
Demographics were retrospectively reviewed, and characteristics identified from the medical record included: age, gender, smoking status, American Society of Anesthesiologists (ASA) classification score, postoperative QuickDASH (the Quick Disabilities, Arm, Shoulder, and Hand) score, and type of fracture. Radiographs were reviewed by fellowship-trained hand surgeons to define fractures based on AO Classification and ulnar styloid fracture type. 8 Surgical characteristics were also obtained from chart review including surgeon experience, operative time, and tourniquet time. Reoperations were also obtained from the medical record, which were defined as unplanned reoperation. Institutional review board approval was obtained prior to beginning this study.
Patients were then divided into 2 groups: patients who underwent surgery less than 12 days from injury and those who underwent surgery 12 days or more from time of injury. The optimal cut-point value for timing of surgery that would best predict reoperation rate was determined using a receiver operating curve (ROC) analysis. The area under the curve (AUC) was calculated to determine the accuracy and generalizability of the optimal cut-point. Patient demographics and surgical characteristics are represented by either mean or counts with percentages and respective 95% confidence interval (CI). Using descriptive statistics, odds ratios and 95% CIs were calculated and provided to evaluate the probable effect size of variables between the early and delayed surgery groups, given the relatively small sample size. Statistical analyses were performed with R Studio software (R Foundation for Statistical Computing).
Results
Two hundred and fifty-seven patients were included in the final statistical analysis with mean follow-up of 23.9 weeks. Median age of patients in the less-than-12-day group was 59 (95% CI: [56.0, 62.0]) and 60 (95% CI: [56.0, 66.0]) in the 12-days-or-greater group. Median time to surgery for the less-than-12-day group was 6 days (interquartile range (IQR): 4-8 days) versus 15 days in the delayed group (IQR: 13-19 days). Most fractures were C1 (31.4% vs 30%), C2 (31.4% vs 26%), or C3 (10.6% vs 12%) AO classification for the early and delayed groups, respectively. No differences were found with regards to age, gender, smoking status, percentage of concomitant procedures, AO classification, or ulnar styloid fracture type between groups. Both groups had a similar tourniquet time, operative time, or postoperative QuickDASH scores collected at a mean follow-up of 74.3 days postoperatively.
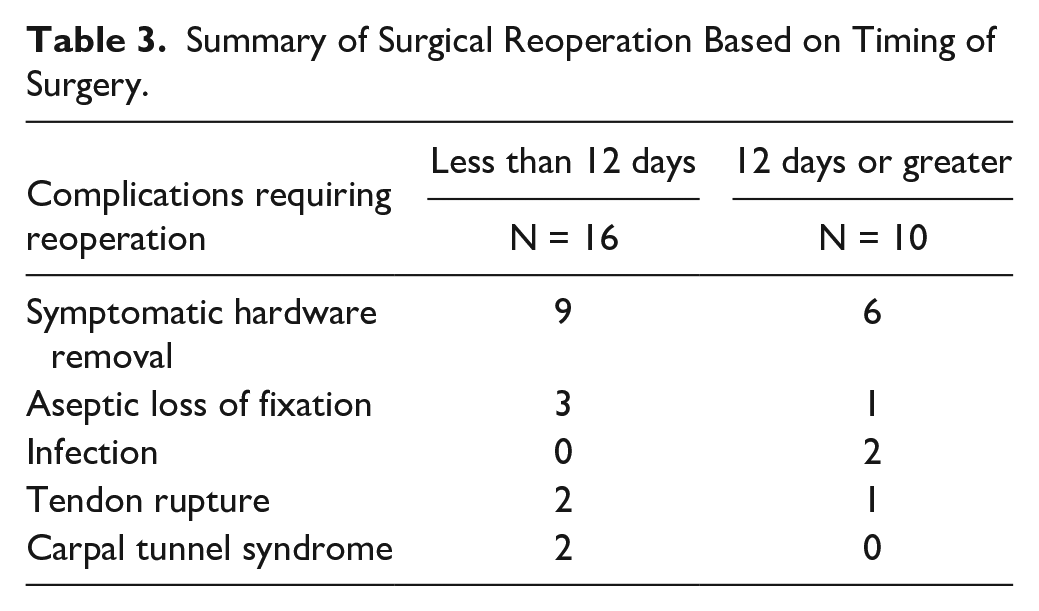
Furthermore, the delayed group had a higher rate of reoperation (7.7% vs 20.0%, OR 2.98; 95% CI: [1.21, 7.03]), patients with an ASA of 3 (OR 6.04; 95% CI: [1.58, 43.3]) and more surgeon experience in years (OR: 10 [8.0, 22.0]) when compared to the early group (Tables 1 and 2). The AUC curve was 0.62 (95% CI: [0.49, 0.74]) with an optimal cutoff of 12 days. When excluding symptomatic hardware removal, there was a similar reoperation rate between the 2 groups, 40% compared to 43.8% in the delayed and early group, respectively. In addition, when evaluating various cutoffs for delayed surgery, patients who had surgery 7 days or greater from injury had a reoperation rate of 13.4% compared to 6.09% (OR 2.34 (95% CI: [0.98, 6.28]). Patients who underwent surgery 21 days or more from injury had a reoperation rate of 22.2% compared to 9.68% (OR 2.78; 95% CI: [0.36, 12.7]). Reasons for reoperation included symptomatic hardware removal, revision ORIF, infection, tendon rupture, and delayed carpal tunnel syndrome requiring surgical release. In addition, patients underwent hardware removal for one of the following reasons: hardware prominence, wrist stiffness, tendon irritation, pain and swelling overlying the plate and pain with weightbearing. In the early surgery group, 9 patients underwent removal of hardware and 3 required revision ORIF for loss of fixation. The 2 patients who underwent carpal tunnel release additionally underwent a concomitant flexor tenosynovectomy or wrist/finger manipulation at 106 days and 61 days after the index surgery, respectively. In the delayed group, 6 patients underwent removal of hardware, 2 patients underwent irrigation and debridement for deep infection, and 1 patient had a revision ORIF for loss of fixation. Overall, 3 patients had a reported tendon rupture: 2 extensor pollicis longus ruptures in the early surgery group compared to 1 flexor pollicis longus rupture in the delayed surgery group (Table 3). Furthermore, in the early group, no patients required an osteotomy in contrast to the delayed group where 7 patients were reported to have undergone an osteotomy during initial fixation at an average of 29.1 days from injury.
Summary of Patient and Fracture Characteristics.
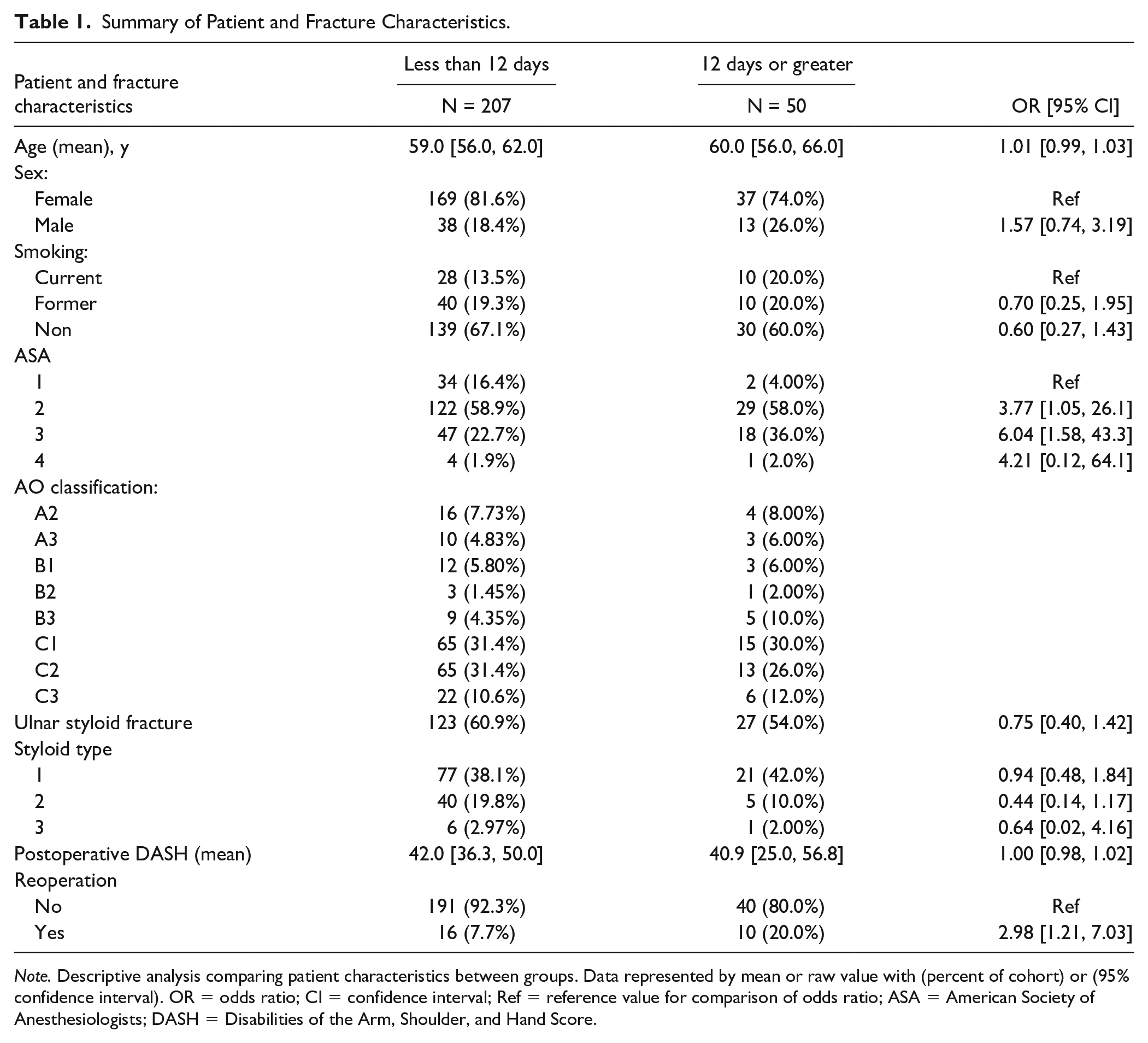
Note. Descriptive analysis comparing patient characteristics between groups. Data represented by mean or raw value with (percent of cohort) or (95% confidence interval). OR = odds ratio; CI = confidence interval; Ref = reference value for comparison of odds ratio; ASA = American Society of Anesthesiologists; DASH = Disabilities of the Arm, Shoulder, and Hand Score.
Surgical Characteristics.
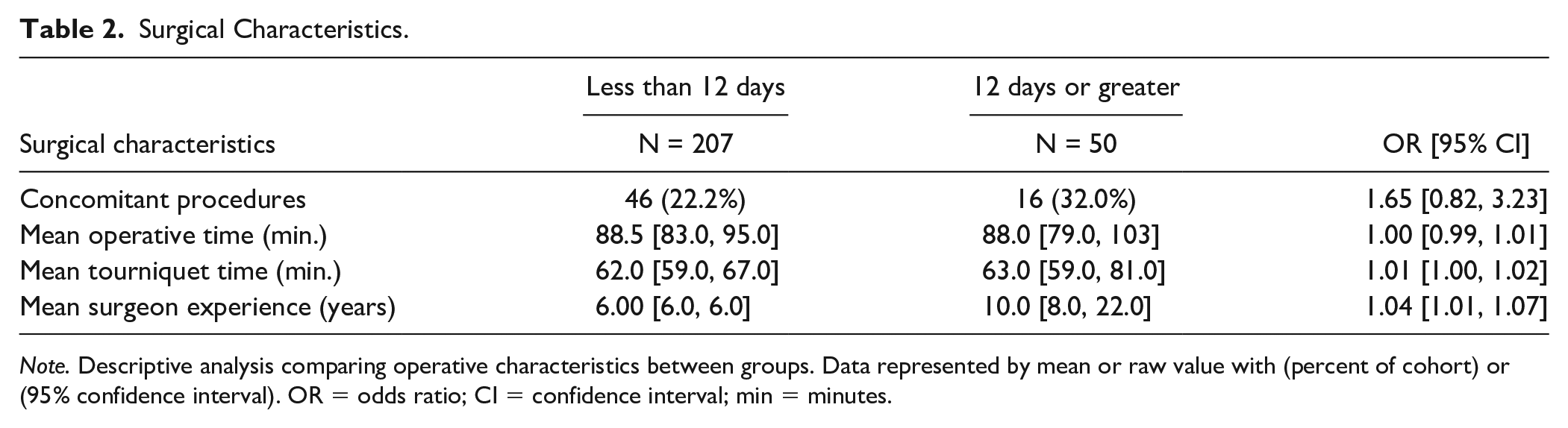
Note. Descriptive analysis comparing operative characteristics between groups. Data represented by mean or raw value with (percent of cohort) or (95% confidence interval). OR = odds ratio; CI = confidence interval; min = minutes.
Summary of Surgical Reoperation Based on Timing of Surgery.
Discussion
Understanding the effect of timing of distal radius fixation on patient outcomes may improve management of these common injuries. Our study found that the timing of volar plate fixation was not associated with differences in postoperative QuickDASH scores, operative time, or tourniquet time. However, in a cohort of mainly AO type C fractures, delay of surgery of 12 or more days after injury was associated with a higher reoperation rate. To our knowledge, this is the largest study to date evaluating the effect of timing of volar plate fixation on reoperation rate compared to previous literature.
While there is no established consensus regarding optimal timing of volar distal radius fixation, prior studies have shown clear advantages to early management of other types of fractures such as hip and proximal humerus fractures.9,10 In addition, many studies have shown a trend toward improved range of motion and upper extremity function with earlier fixation in the short-term postoperative period.6,11 Yamashita et al 11 found that patients with AO type A fractures who underwent volar fixation within 7 days had significantly improved wrist range of motion, grip strength, and QuickDASH scores at early postoperative follow-up, albeit no differences were noted by 48 weeks. In a study performed by Weil et al, 12 no significant difference was found with QuickDASH scores following delayed surgery, after outliers were removed. The results for the short-term QuickDASH scores in our study population were relatively high than prior studies with longer collection times; similarly, no significant differences between the early and delayed groups were encountered. However, these results may be limited due to differences in study population and overall patient compliance with postoperative surveys. While there may be a potential benefit for faster return to daily activities in cases where fixation can be achieved within an earlier timeframe, current evidence has shown limited clinical differences in motion and overall function at long-term follow-up.
Delayed surgical intervention for distal radius fractures is sometimes considered to be more difficult and potentially leads to a longer operative time and tourniquet time. In a retrospective study of isolated distal radius fractures treated with various fixation techniques, Hooper et al 4 reported increased surgeon-perceived difficulty and decreased reduction quality in patients undergoing distal radius fracture fixation greater than 7 days after injury. However, the perceived difficulty and reduction quality improved with the volar plating technique due to the ability to openly debride the fracture site and obtain the reduction under direct visualization. In our study, patients with longer delay to fixation had similar operative and tourniquet time compared to the early fixation group. Given the relatively even distribution of AO injury types and rate of concomitant injuries between groups, it is possible that cases with longer operative time were related to fracture complexity or the need for other concomitant procedures. However, further studies are warranted to elucidate any potential clinical effects associated with longer time spent in the operating room.
Contrary to prior studies evaluating timing of surgery, our results demonstrated a higher reoperation rate in patients undergoing delayed fixation compared to those undergoing early fixation (20% versus 7.7%, respectively, OR: 2.98; 95% CI: [1.21, 7.03]). In comparison, Lee et al 13 found complications in 12% who were fixed 3 to 6 weeks after injury versus 10% in an earlier cohort. Weil et al 12 had only 1 out of 40 patients treated after a minimum of 3 weeks require return to the operating room for prominent hardware. Furthermore, differences in reported reoperation rate in this study compared to prior studies are likely due to the varying patient population cohorts and sample size. Future randomized, controlled, or multicenter studies with larger patient cohorts may be useful to further delineate the complication rate with delayed surgery.
While operative time was similar between both patient groups, there were 7 patients in this group that required osteotomies. Despite similar postoperative QuickDASH scores, it is possible that surgeons may encounter more challenging or complex delayed treatment of distal radius fractures that have developed robust callus or even malunion requiring osteotomy and soft tissue dissection. In a retrospective review evaluating patients with early versus late reconstruction of malunited fractures with osteotomy and bone grafting, the authors suggested that earlier management may allow for easier visibility and the ability to osteotomize directly through the original fracture site. 14 Although the clinical reason for increased reoperation rate after delayed surgery in our group is uncertain, we believe this information can be helpful in counseling patients regarding prognosis of these injuries and encourage efficient patient scheduling for operative treatment when appropriate.
There are many unpredictable variables including patient, surgeon, and scheduling-related factors which also may contribute to delayed management. Our results demonstrated that the delayed group had more patients with an ASA score of 3. These findings may be related to the need for further medical optimization of these patients prior to undergoing surgery. Although previous studies have identified comorbidities and higher ASA scores as risk factors for postoperative complications, there is limited evidence on the effect of comorbidities with delayed surgery and its outcomes.15,16 In addition, the group of patients fixed later in their clinical course was, on average, treated by surgeons with more years of experience. Although unlikely to be clinically significant, this could be related to referral patterns, differences in management protocols, or scheduling practices among surgeons. Overall, further studies with larger sample sizes may be warranted to assess whether these factors have a larger effect on reoperation rates and overall patient outcomes.
There are limitations present in this study. Selection bias and confounders for various indications, patient factors including complexity of fracture fixation, comorbidities, or obstacles encountered for scheduling surgery that may ultimately lead to delaying surgery may affect the overall results and reoperation rate. In addition, postoperative outcome scores were limited secondary to the retrospective nature of this study and patient compliance with surveys. Although the ROC analysis demonstrated that 12 days or greater best predicts reoperation rate in this study, the AUC of 0.62 (95% CI: [0.49, 0.74]) limits the overall generalizability of these results to all patient populations. Therefore, larger study cohorts are needed to further delineate the optimal timing of surgical intervention. Multiple surgeons present within this study does add heterogeneity to the surgical techniques and perioperative protocol, which may be a confounder due to differences in surgeon experience. Although this sample size is larger than prior studies in the literature and a post-hoc power analysis was not performed, the use of odds ratio and CIs allows for overall interpretation of findings for the relative sample size of this study. This is also one of the few studies to investigate the effects of timing on surgical characteristics, patient outcomes, and reoperation rate in patients with distal radius fractures.
In conclusion, our study demonstrates that volar plating of distal radius fractures remains a reliable procedure when performed in a delayed fashion. However, there is some evidence that patients treated 12 days or greater after injury may have a higher rate of requiring return to the operating room. Additional studies are necessary to validate and expand the evidence available to establish a consensus on the most favorable timing of surgery and its effect on outcomes after volar plating of distal radius fractures.
Footnotes
Ethical Approval
This study was approved by our Institutional Review Board.
Statement of Human and Animal Rights
The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 and 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants in this study. All information used is anonymous.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.