
Abstract
Background:
Depression is a known risk factor for inferior outcomes after orthopedic procedures, but its specific relationship with distal radius fractures remains unknown. This study investigates the relationship between preoperative diagnosed depression and common postoperative complications occurring within the first year after open reduction internal fixation (ORIF) for distal radius fractures.
Methods:
This retrospective study used Truven MarketScan database and the Current Procedural Terminology (CPT) codes to identify distal radius fracture patients who underwent ORIF in the United States between January 1, 2009, and December 31, 2019. International Classification of Diseases (ICD) codes were used to identify patients with and without a diagnosis of preoperative depression. Univariate, multivariate, t test, and χ2 analyses were performed to determine the association between preoperative depression and postoperative complications following a distal radius fracture surgery.
Results:
Of the 75 098 eligible patients, 9.9% had at least one ICD code associated with preoperative depression. Preoperative depression was associated with increased odds for surgical site infection (odds ratio [OR] 1.25, confidence interval [CI] 1.14-1.37), emergency department visits for postoperative pain (OR 1.28, CI 1.15-1.36), hardware complication (OR 1.18, CI 1.07-1.30), removal of hardware within 1 year (OR 1.16, CI 1.09-1.27), wound complication (OR 1.17, CI 1.08-1.27), and 30-day readmission (OR 1.21, CI 1.07-1.31).
Conclusions:
Preoperative diagnosed depression is associated with increased complications following distal radius fracture surgery. These results can help guide preoperative and postoperative protocols in these higher risk patients. More research is needed to investigate if depression is a modifiable risk factor, as depression treatment could potentially improve postsurgical outcomes.
Introduction
Distal radius fractures are one of the most common orthopedic injuries encountered by surgeons and comprise nearly 20% of all fractures that are seen in the emergency department (ED). 1 The incidence of distal radius fractures in the United States is 600 000, and as the population ages, the incidence is rising. 2 The costs associated with treating distal radius fractures are significant. Due to the high cost to society and the modern-day shift to value-based reimbursement, it is imperative that surgeons minimize complications and cost associated with this injury.
Providers must be prudent when counseling patients on whether to undergo open reduction internal fixation (ORIF) for their distal radius fracture, considering each patient’s age, activity level, and medical comorbidities. An additional consideration is the presence of diagnosed depression in these patients.
Depression is a common condition, afflicting nearly 265 million people worldwide. The prevalence of depression has continued to grow, particularly since the start of the COVID-19 pandemic.3,4 Depression is diagnosed clinically by assessing patients for 9 symptoms (depressed mood, diminished interest, weight loss, insomnia, psychomotor agitation, fatigue, inappropriate guilt, diminished concentration, suicidal ideation) as listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (DSM-V). 5 Those who have at least 5 of those symptoms are diagnosed with depression. Depression has been shown to be a known risk factor for outcomes after orthopedic procedures6 -8; however, its specific relationship with distal radius fracture outcomes remains unknown.
The purpose of this study was to investigate the relationship between preoperative diagnosed depression and complications such as ED visit for pain, complex regional pain syndrome (CRPS), hardware removal, hardware complication, wound complication, surgical site infection, and readmission following distal radius fracture ORIF.
Materials and Methods
Data Source and Cohort Selection
We performed a retrospective analysis of patients who underwent ORIF of a distal radius fracture in the United States between January 1, 2009, and December 31, 2019. Patients were identified using the IBM MarketScan Commercial Claims and Encounters and Medicare Supplemental and Coordination of benefits databases. This is a private insurance claims database that includes both private insurance and Medicare supplement insurance providers. This database provides inpatient and outpatient records on patient surgical procedures and follow-up care and has been used for clinical and epidemiological studies in the field of orthopedics, including other distal radius fracture studies.6,9 -11
The database was queried for patients who underwent ORIF of a distal radius fracture using the Current Procedural Terminology (CPT) codes 25607, 25608, and 25609 (Table 1). Once identified, patients with less than 6 months of continuous preoperative enrollment, patients without 12 months of continuous postoperative enrollment, and patients younger than 18 years at the time of surgery were exlcluded. For additional exclusions, we queried for International Classification of Diseases (ICD) codes for patients with open fracture(s) and a preoperative diagnosis of CRPS. This search criterion was designed to capture patients with distal radius fractures that had adequate time for a preoperative depression diagnosis and significant follow-up to capture major postoperative complications.
Distal Radius ORIF CPT Codes.
Note. CPT = Current Procedural Terminology; ORIF = open reduction internal fixation.
Baseline Patient Data
We recorded demographic information and comorbidities for identified subjects using ICD codes listed in Supplemental Appendix A. Comorbidities included obesity, osteoporosis, renal disease, hyperlipidemia, hypertension, coronary artery disease, congestive heart failure, rheumatological diseases, and diabetes. We also included tobacco use, alcohol abuse, anxiety, low back pain, and fibromyalgia, assuming that these comorbidities might coincide with depression. 12
We divided the identified patients into 2 groups based on the presence or absence of a preoperative diagnosis of depression. The most common ICD codes were used to identify patients with a depression diagnosis (Table 2). Presence of at least one of these codes categorized patients into the “Depression” group. Patients with none of these ICD codes were categorized into the “No Depression” group.
ICD 9 and 10 Codes Used to Identify Patients With Depression.
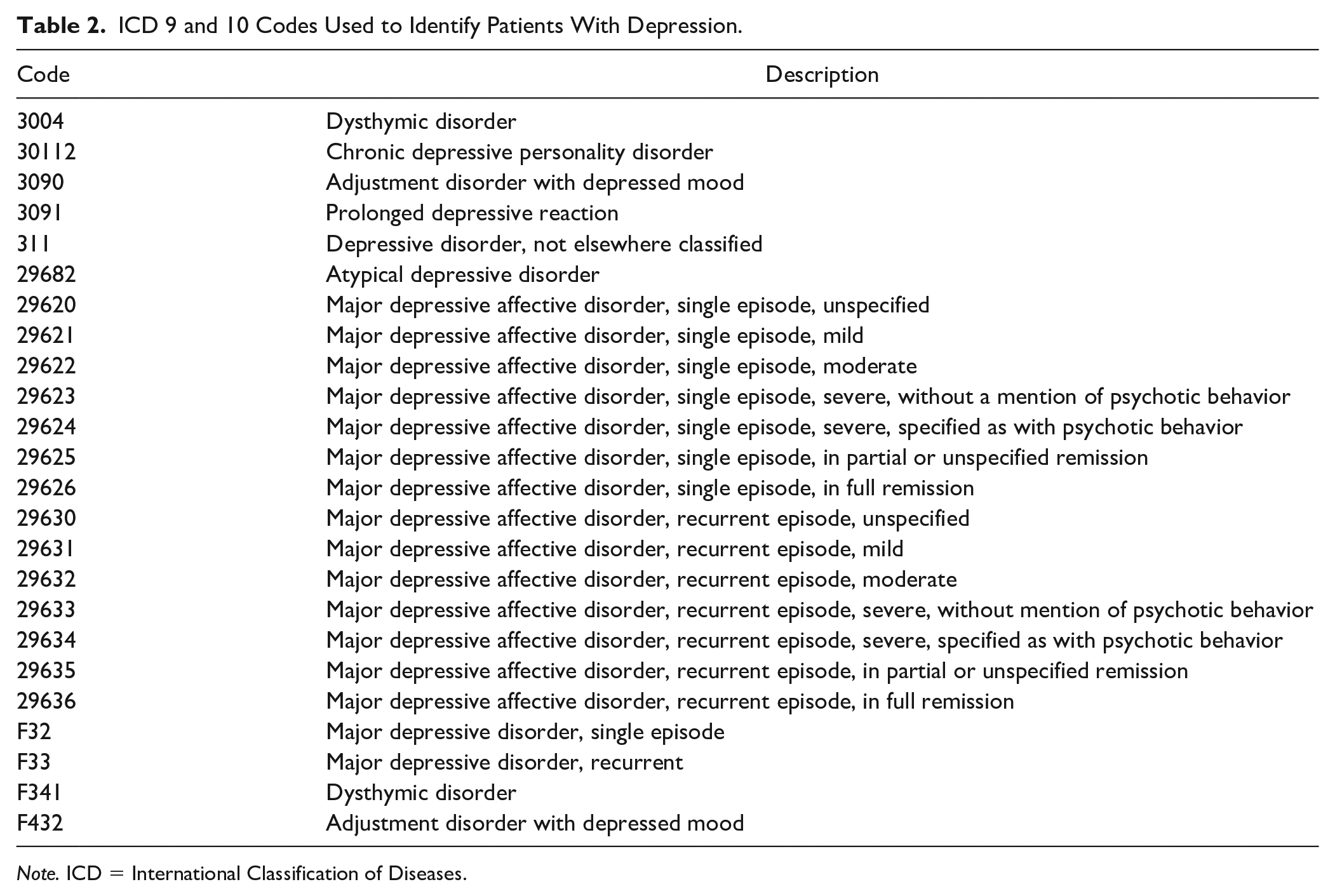
Note. ICD = International Classification of Diseases.
Postoperative Outcomes
The main outcomes of interest in this study were common postoperative complications occurring within 1 postoperative year after the distal radius fracture surgery. These included a return to the ED for treatment of pain, development of CRPS postoperatively, surgical site infection, hardware irritation or failure, removal of hardware (ROH), wound complication (wound dehiscence or fluid collection), 30-day readmission, and 90-day readmission.
Statistical Analysis
We performed a univariate analysis to assess differences of baseline characteristics and comorbidities between the diagnosed depression and no-depression cohorts. For continuous variables, we performed an independent t test, and for categorical variables, we used a χ2 analysis. Subsequently, we performed a univariate analysis to identify differences in principle outcome measures between the two cohorts. Binomial multivariate logistic regression analyses were used to identify if preoperative diagnosed depression is associated with independent complications, while controlling for previously established comorbidities and baseline criteria. We reported all results as odds ratios (OR) with a 95% confidence interval (CI). A P value of less than .05 was considered significant. We performed all statistical analyses using R (R core team 2020) statistical software.
Results
Patient Demographics and Comorbidities
A total of 75 098 patients were included in the analysis. Most of the patients (90.1%) did not have a diagnosis of depression, while 9.9% of patients had at least one ICD code associated with preoperative depression (Table 3). The cohorts were similar in the distribution of sex. Univariate analysis of the baseline characteristics and comorbidities between the groups can be found in Table 3. Univariate analysis of complications between the two cohorts can be found in Table 4.
Baseline Characteristics.
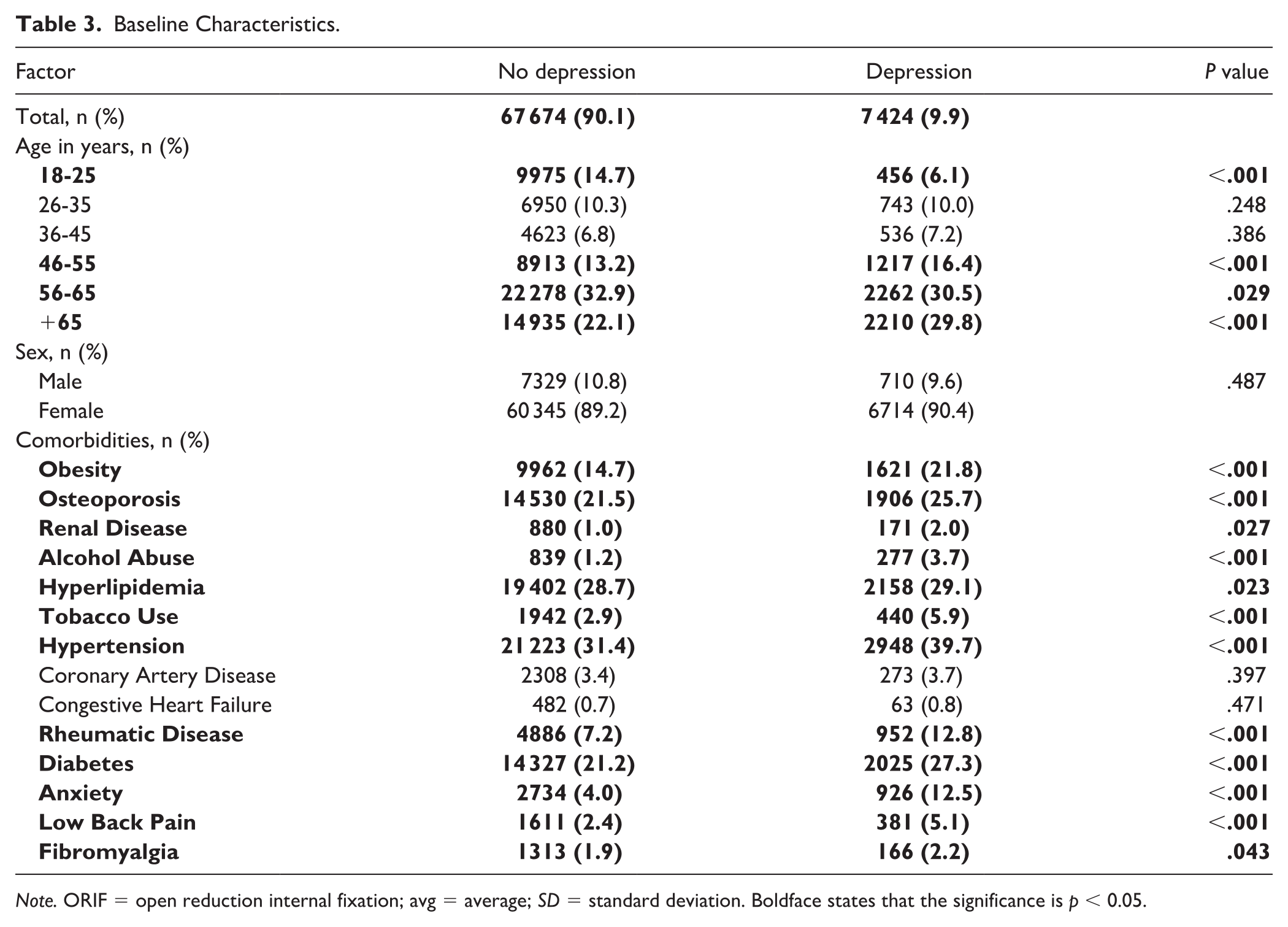
Note. ORIF = open reduction internal fixation; avg = average; SD = standard deviation. Boldface states that the significance is p < 0.05.
Univariate Analysis of Depression and Patient Complications.
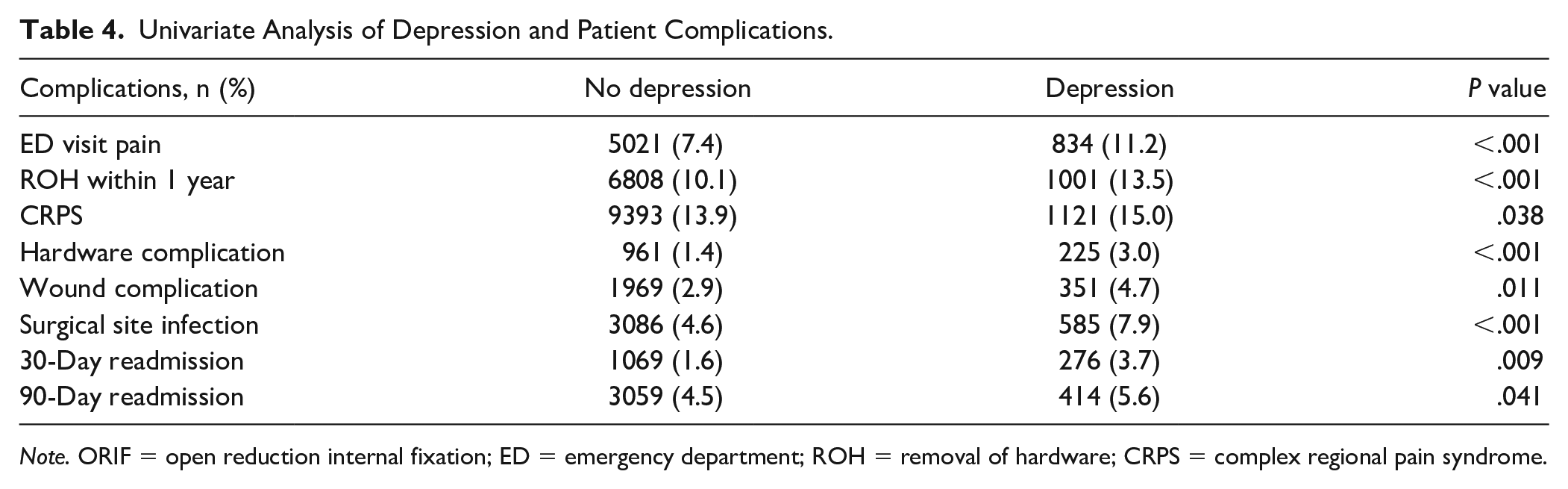
Note. ORIF = open reduction internal fixation; ED = emergency department; ROH = removal of hardware; CRPS = complex regional pain syndrome.
Multivariable analyses were performed to determine which complications were independently associated with a preoperative depression diagnosis (Table 5). Preoperative depression was significantly associated with most complications including ED visits for postoperative pain (OR 1.28, CI 1.15-1.36), ROH within 1 year (OR 1.16, CI 1.09-1.27), hardware complication (OR 1.18, CI 1.07-1.30), wound complication (OR 1.17, CI 1.08-1.27), surgical site infection (OR 1.25, CI 1.14-1.37), and 30-day readmission (OR 1.21, CI 1.07-1.31.
Multivariable Analyses of Depression and Patient Complications.
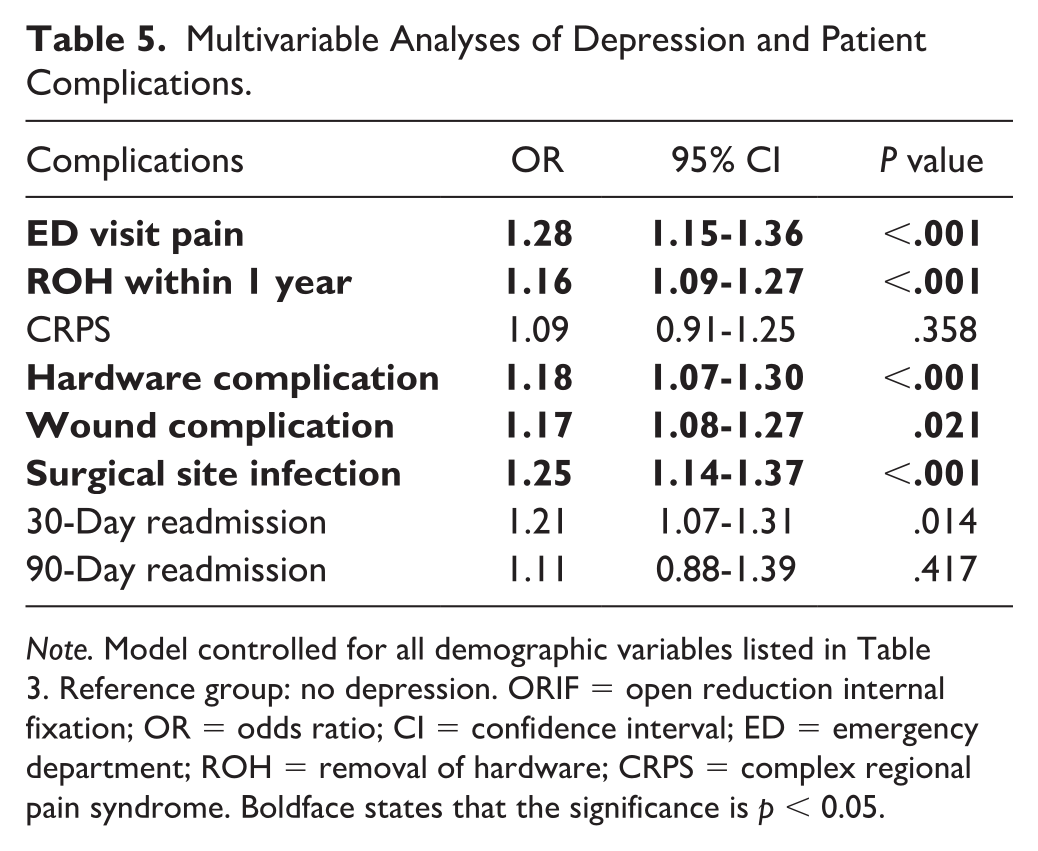
Note. Model controlled for all demographic variables listed in Table 3. Reference group: no depression. ORIF = open reduction internal fixation; OR = odds ratio; CI = confidence interval; ED = emergency department; ROH = removal of hardware; CRPS = complex regional pain syndrome. Boldface states that the significance is p < 0.05.
Discussion
Depression is an increasingly common medical comorbidity in patients with distal radius fractures. Postoperative complications associated with depression in other procedures have been investigated. Wilson et al 8 studied outcomes in patients with a preoperative depression diagnosis undergoing total ankle arthroplasty and found that there was a significant increase in wound complications, length of stay, and overall health care resource utilization when compared to those patients without a diagnosis of depression. A similar study found that preoperative depression was associated with a significant increase in prosthetic joint infections, a non-home discharge, and readmission rates in patients undergoing revision total hip and total knee replacements. 7
Depression has profound effects on patients, both mentally and physically. In patients with depression, there is an increased risk for hypertension, diabetes, stroke, obesity, and early mortality. 13 We found that depression was associated with increased odds of hospital readmission after surgery. This is in keeping with recent evidence suggesting a dose-dependent relationship between a patient’s depression and their odds for readmission after discharge.14 -16 The exact reason for this has yet to be fully elucidated, although much interest is being placed in exploring the relationship between pain and depression, as many of these readmissions are due to issues with pain control. 17
Among patients treated surgically for a distal radius fracture, we found a significant increase in complications such as surgical site infections, hardware complications, and ED visits for pain in patients with diagnosed depression when compared to patients without depression. The cost to care for patients with distal radius fractures is high, and factors adding to this expense should be thoroughly investigated. In our study, we found specifically that those with diagnosed depression have an increased odd of visiting the ED for postoperative pain control issues. A study by Galarraga and Pines 18 found that total cost of ED visits approximated nearly $330 billion in 2010, accounting for over 12% of national health care expenditures. It has been established that a relationship exists between depression and perception of pain. 19 Based on the results of the current investigation, it seems that providers might tailor pain management strategies accordingly.
In our study, those with preoperative depression experienced an ROH rate of 13.5%, which is higher than the general rates published in prior US reports of about 3%.20,21 The most common reasons for hardware removal after distal radius ORIF include pain, tenosynovitis, and infection. Based on the underlying pathophysiological changes depression causes on the healing body described in the following section, it stands to reason that the increased pain and inflammation experienced by depressed patients would result in increased ROH rates.
Another major postoperative outcome is the incidence of infection, particularly to the operative site. Like other investigations, our study found that those with diagnosed depression had increased odds of surgical site infection (approximately 1.25 times higher) when compared to those without depression, even when controlling for medical comorbidities. While the relationship between infection and depression is likely complicated by a multitude of factors, it is known that the psychological stress experienced by patients with depression coincides with an increased inflammatory state due to the release of proinflammatory cytokines. 22 It has been theorized that this increased systemic inflammatory state diminishes the immune systems’ local responses and that this predisposes the patient to an increased risk of surgical site infection. This may be further exacerbated by the body’s additional global proinflammatory state in the postoperative period.23,24
There are several limitations to the current study, most of which are inherent to a database study. These results are not generalizable to the uninsured population because data from IBM Marketscan contain only privately insured and Medicare patients. We assumed accurate and complete procedural coding for the patient surgeries as well as comorbidities, including depression. It is assumed that the true prevalence of depression is greater than the number of formally diagnosed cases. 25 It is likely that we failed to capture some patients with undiagnosed depression. Furthermore, the database query was not able to account for the severity of depression, which might add nuance to the results. Additional limitations include the inability to link the postoperative complications directly to the original CPT code for distal radius ORIF. We limited our follow-up to 12 months and assumed that codes reported from postoperative day 1 to postoperative 1 year are related to the distal radius fracture. While our sample was large enough to find significant differences between groups, it is possible that these significant differences are due to cohort sizes rather than clinical significance. In addition, we recognize that we are limited in our ability to make generalizable claims because our statistical analyses did not include effect size measures.
While the study included many of the most pertinent patient characteristics and comorbidities, it is impossible to completely control for all possible risk factors in our analysis. We were unable, for instance, to capture the degree of injury, fracture pattern, comminution, and other fracture characteristics. In addition, we were unable to control for the type of hardware used, quality of reduction, and surgical technique. Furthermore, it is impossible for us to discern causation from the correlation seen between depression and postoperative outcomes; therefore, we are unable to comment on how varying depression severity can affect outcomes.
Despite these limitations, the utilization of a large national database allows for the analysis of a significant number of patients, which provide for a strong generalizability of the data. This allows for the identification of differences between groups that may not be realized in small, single-institution studies.
Conclusion
Preoperative diagnosed depression is a risk factor for inferior outcomes after distal radius fracture ORIF. These results can help guide perioperative and postoperative protocols in these higher risk patients, which can include increased surveillance to ensure that their depression is adequately treated and their pain is adequately controlled. Furthermore, patients with diagnosed depression can be made aware of their increased risk for complications to further aid them in shared decision-making. More research is needed to investigate how modifiable depression is as a risk factor given that treatment for depression could potentially improve surgery outcomes.
Supplemental Material
sj-xlsx-1-han-10.1177_15589447231207910 – Supplemental material for Preoperative Depression Is Associated With Increased Complications Following Distal Radius Fracture Surgery
Supplemental material, sj-xlsx-1-han-10.1177_15589447231207910 for Preoperative Depression Is Associated With Increased Complications Following Distal Radius Fracture Surgery by Matthew S. Broggi, William O. Runge, John T. Hurt, Alexander A. Dawes, Roy J. Toston, Akinade A. Ojemakinde, Hayden L. Cooke, Michael B. Gottschalk and Eric R. Wagner in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Statement of Human and Animal Rights
Not applicable, because this article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.S.B., W.O.R., J.T.H., A.A.D., R.J.T., A.A.O., and H.L.C. have nothing to disclose. M.B.G. receives institutional research support from Stryker and Konica Minolta. He is a board or committee member of the American Society for Surgery of the Hand. He is an editor for Journal of Hand Surgery and Surgical Techniques in Orthopedics. E.R.W. receives consulting fees from Stryker, Biomet, Acumed, and Osteoremedies and research support from Arthrex and Konica Minolta.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.