
Abstract
Background:
The appropriate initial management of pediatric trigger thumb (PTT) remains controversial. Some providers advocate for prolonged nonoperative management, whereas others may offer surgical release to provide a reliable and expedient resolution. The goal of this study was to elucidate the practice patterns of surgeons with different fellowship training who treat patients with PTT. We hypothesized that an association between surgeon specialty training and treatment algorithm would be identified.
Methods:
A cross-sectional survey was sent to mailing lists of 3 professional organizations whose members represent most providers caring for pediatric hand patients. Respondents were asked their training background and treatment recommendations for several clinical scenarios. Responses were compared across subspecialties.
Results:
Of the respondents, 444 completed a fellowship in hand surgery, 167 completed a pediatric orthopedic fellowship, and 155 completed an additional congenital hand fellowship. Providers with hand fellowship training were more likely to offer surgical intervention as a first-line treatment for a 3-year-old patient with a flexible trigger thumb than those who completed a pediatric orthopedic fellowship (P = .001), and more likely to offer surgical intervention to a 3-year-old patient with an intermittent (P = .007), painful (P = .015), or locked (P = .012) trigger thumb than those providers who completed additional training in congenital hand surgery. No statistically significant differences in practice patterns were appreciated for children aged 6 and 18 months.
Conclusion:
Variability was appreciated in practice patterns for initial treatment recommendation for a patient presenting with PTT. Subspecialty training does appear to affect treatment recommendations for clinical scenarios involving a 3-year-old patient with PTT, although this trend is not observed when treating younger patients.
Keywords
Introduction
Pediatric trigger thumb (PTT) is a common condition with an estimated incidence between 0.5 and 3 in 1000 patients.1 -3 Pediatric trigger thumb is thought to be acquired with a potentially genetic predisposition, as a positive family history of trigger thumbs is often elicited. 1 The underlying pathophysiology contributing to the anatomical mismatch of the first annular pulley and flexor pollicis longus tendon remains unclear. Classically, children with trigger thumb present with either dynamic triggering or with a thumb locked in interphalangeal joint flexion. 2 Approximately 25% of patients have bilateral trigger thumbs, although these may develop asynchronously.4,5
Appropriate treatment of PTT remains a point of controversy. Nonoperative management with observation alone, stretching exercises, or splinting have been demonstrated to have satisfactory results in the literature. 2 ,6 -10 However, it may take years for the trigger thumb to resolve, and residual restrictions in thumb interphalangeal joint range of motion may occur. 11 Conversely, surgical intervention is fast and reliable but carries the inherent risks of pediatric anesthesia and potential operative complications such as infection and neurovascular injury. 9 ,11 -14
Marek et al 11 found differences in opinion regarding initial management of PTT in a cohort of 27 pediatric hand surgeons. Given the growing body of literature on the outcomes of nonoperative management, our study aims to elucidate practice patterns of those managing PTT in a larger, more diverse cohort. We hypothesized that surgeon specialty training would influence treatment decisions for initial management of patients with PTT.
Methods
The mailing lists for members of the Pediatric Orthopaedic Society of North America, American Society for Surgery of the Hand, and American Association for Hand Surgery were used to contact providers involved in management of PTT. A cross-sectional survey using both multiple-choice and case-based questions was distributed to participants via REDCap. Branching logic was used for the survey so that appropriate follow-up questions were shown based on previous responses. Multiple-choice questions regarding fellowship training and practice information were included. The clinical cases used to assess treatment decisions included children with either painful or painless trigger thumb with varying degrees of motion and in some instances a locked digit. Case scenarios were replicated for children aged 6 and 18 months and 3 years. If providers selected nonoperative management, then they were asked the duration of nonoperative treatment and whether they would recommend observation, exercises, or splinting. The full list of questions can be found in Supplemental Appendix A.
Survey results were then compiled and analyzed. Those who reported not actively treating patients with PTT and those who responded to less than half of the survey questions were excluded. χ2 analysis was used to evaluate an association between fellowship training and initial treatment decision. If the χ2 test was significant, post hoc tests with Bonferroni adjustments were calculated. For any identified group differences, odds ratios (ORs) were also calculated to aid in interpretation.
Results
Although 981 participants indicated that they actively treat patients with PTT, 189 responses were excluded from analysis due to missing data. An additional 17 responses were excluded because they did not have a relevant fellowship (congenital hand surgery, hand surgery, or pediatric orthopedic surgery), and due to a small sample size, 9 participants were excluded who completed fellowships in both hand and pediatric orthopedic surgery. After application of the exclusion criteria, a total of 766 respondents were included in our statistical analysis. Of the respondents, 444 completed a fellowship in hand surgery, 167 completed a pediatric orthopedic fellowship, and 155 completed an additional congenital hand fellowship. A total of 42.8% of respondents practiced in an academic setting and 57.2% in a private setting. Approximately 85% of those answering the survey practiced in the United States.
For a 3-year-old patient presenting for evaluation of PTT, there were several significant group differences across the 4 scenarios (Table 1). For a 3-year-old patient who presents with a trigger thumb that actively and passively extends to neutral, there was a statistically significant difference in initial treatment recommendation, χ2 = 14.35, P = .001. Specifically, hand fellowship-trained surgeons (n = 172, 39%) offered surgery more frequently than pediatric orthopedic-trained surgeons (n = 39, 23%), OR = 2.08 (95% confidence interval [CI], 1.38-3.13). There were no other significant group differences.
Initial Treatment Recommendations for a 3-Year-Old Patient with PTT.
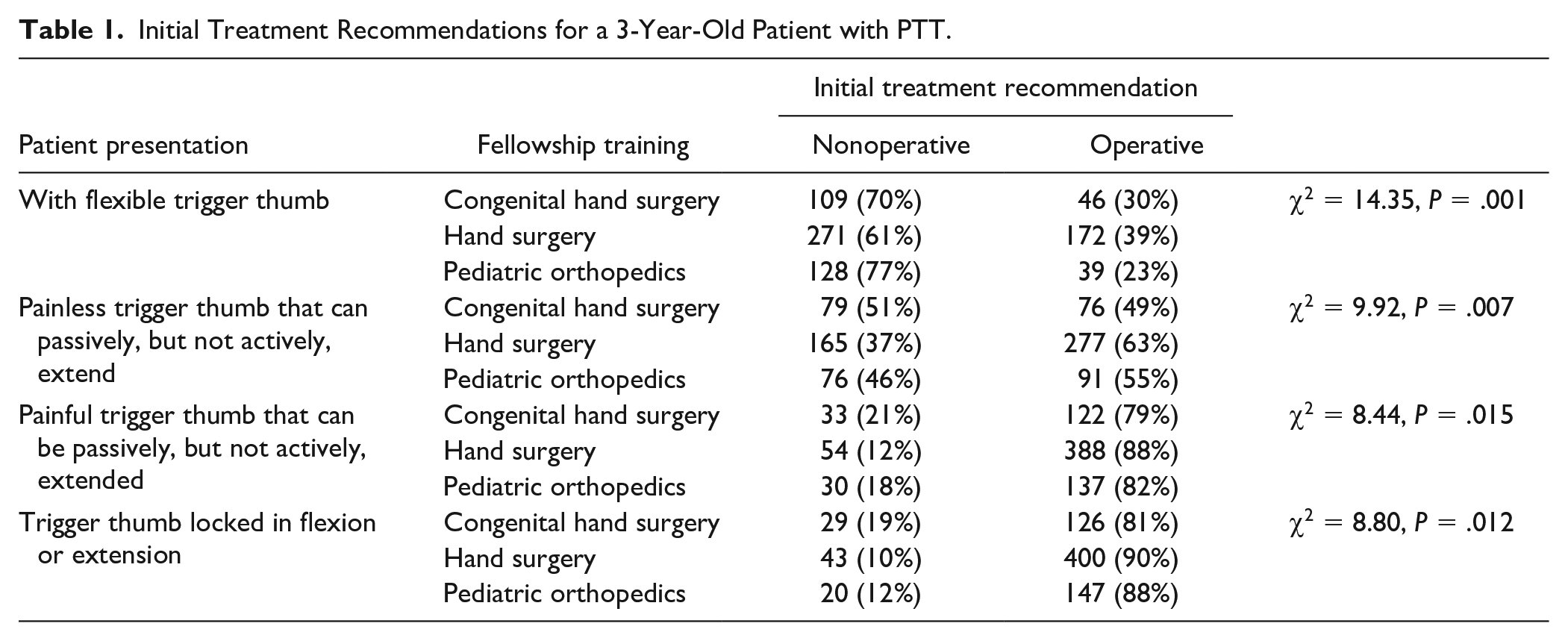
For a 3-year-old patient who presents with a painless trigger thumb that can be passively, but not actively, extended to neutral, there was a statistically significant difference in initial treatment recommendation, χ2 = 9.92, P = .007. The only significant difference was between hand fellowship-trained surgeons (n = 277, 63%) offering surgery more frequently than surgeons with additional formal training in congenital hand surgery (n = 76, 49%), OR = 1.75 (95% CI, 1.21-2.52).
For a 3-year-old patient who presents with a painful trigger thumb that can be passively, but not actively, extended to neutral, there was a statistically significant difference in initial treatment recommendation, χ2 = 8.44, P = .015. The only significant difference was between hand fellowship-trained surgeons (n = 388, 88%) offering surgery more frequently than surgeons with additional formal training in congenital hand surgery (n = 122, 79%), OR = 1.75 (95% CI, 1.21-2.52).
For a 3-year-old patient who presents with a trigger thumb locked in flexion or extension, there was a statistically significant difference in initial treatment recommendation, χ2 = 8.80, P = .012. The only significant difference was between hand fellowship-trained surgeons (n = 400, 90%) offering surgery more frequently than surgeons with additional formal training in congenital hand surgery (n = 126, 81%), OR = 2.13 (95% CI, 1.28-3.57).
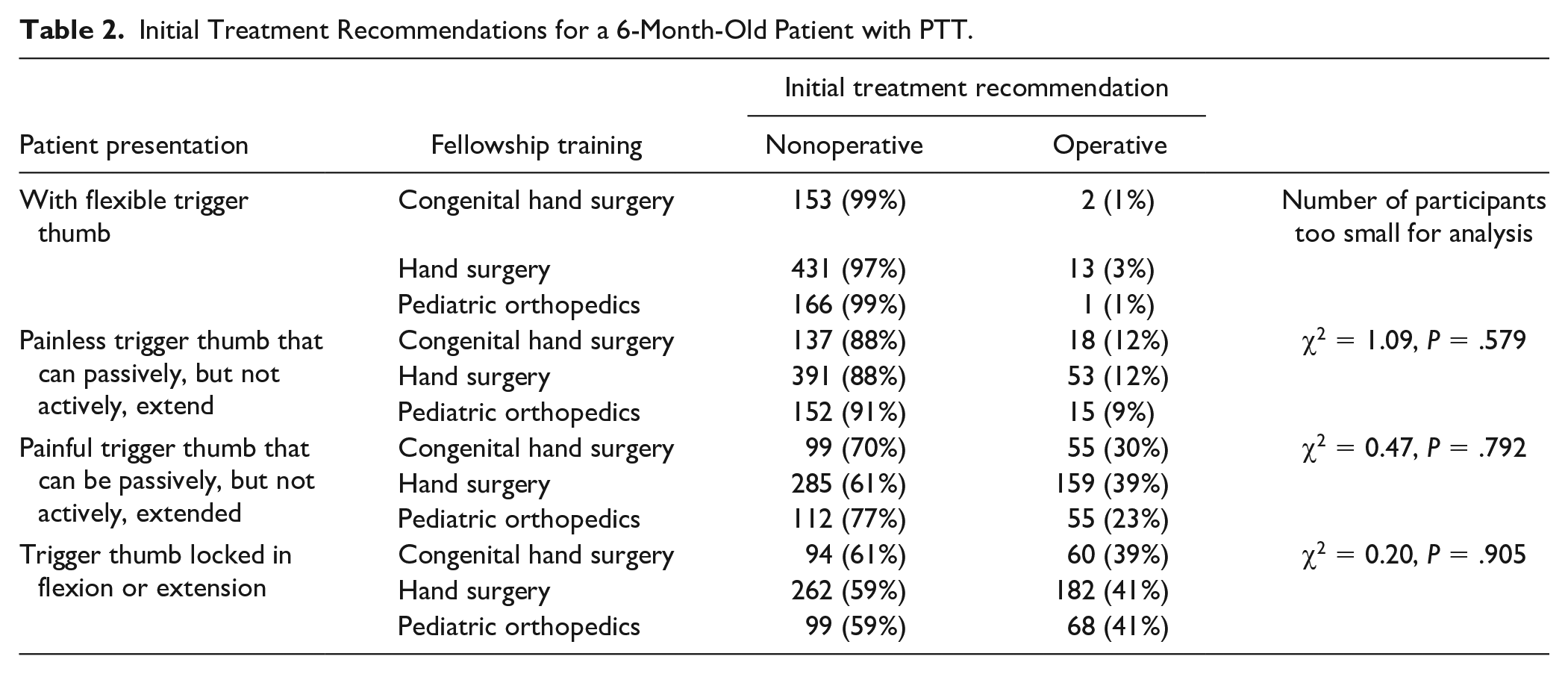
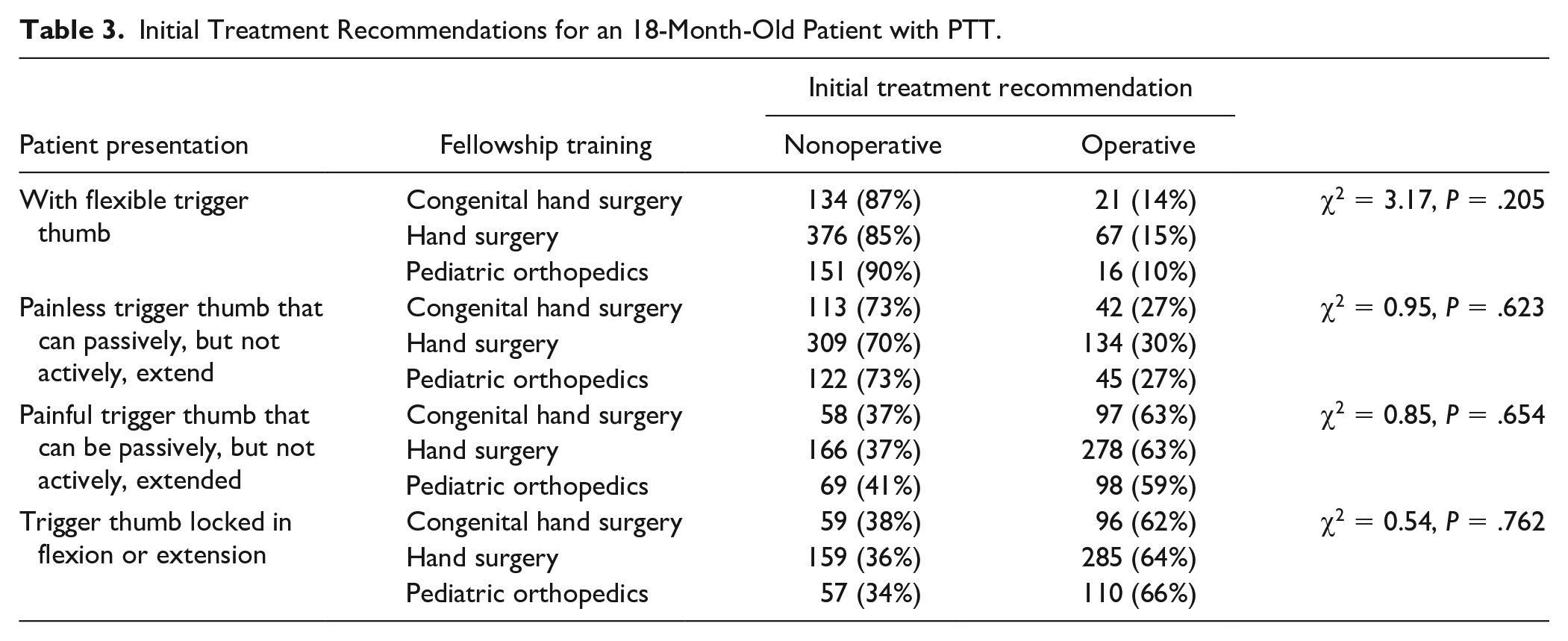
For 6- and 18-month-old patients presenting for evaluation of PTT, there was no significant difference in initial treatment recommendations in relation to fellowship training for all 4 scenarios in each age group (Tables 2 and 3).
Initial Treatment Recommendations for a 6-Month-Old Patient with PTT.
Initial Treatment Recommendations for an 18-Month-Old Patient with PTT.
Discussion
The appropriate approach to the treatment of PTT remains a topic of controversy in hand surgery. Common treatment options consist of either surgical release or nonoperative management with observation, stretching, or splinting. Some advocate for prolonged nonoperative management as resolution can occur over time, whereas others advocate for surgical management due to high rates of complete resolution and low overall rates of complications. The reported rates of successful nonoperative management vary quite significantly across studies, which makes it challenging to use a data-based approach.
We have experience with patients presenting who have been advised by providers that, given the relatively low risk of operative intervention, surgery is indicated for management of PTT. In light of these encounters, we sought to clarify practice patterns among surgeons who care for patients with PTT, in an effort to determine whether training background had any association with proposed treatment.
We found an association between surgical subspecialty training and the recommended initial management of PTT in clinical scenarios involving 3-year-old patients. Hand surgeons were more likely to select operative management as initial treatment than pediatric orthopedic surgeons for a 3-year-old patient with a flexible painless trigger thumb. Hand surgeons were more likely to select operative management as initial treatment than surgeons with additional training in congenital hand surgery for 3-year-old patients with both painless and painful limitation in active thumb extension, as well as 3-year-old patients with a locked trigger thumb. There was no significant difference in treatment recommendations in relation to surgical training for patients who were aged 6 or 18 months.
Treatment trends in management of PTT were previously analyzed by Marek et al 11 in a survey of 27 pediatric hand surgeons. Participants were presented 2 clinical scenarios: a 2-year-old with a 6-month history of intermittent triggering, or a 2-year-old with a 6-month history of a locked trigger thumb. In their cohort, initial surgical management was recommended by 48% and 85% of surgeons, respectively. Although our study did not provide the exact clinical scenario described in this study, similar trends were identified in our data in scenarios involving a 3-year-old patient with the history of a flexible versus locked digit. In our study, a 3-year-old patient with a flexible trigger thumb was offered initial surgical management by 34% of respondents, while a 3-year-old patient with a locked trigger thumb was offered initial surgical management by 88% of respondents. Owing to the difference in how the questions were presented, including duration of symptoms, age, and presence of intermittent triggering, it is difficult to make a direct comparison. However, our results are similar in that there is heterogeneity in treatment algorithms, and a patient with a locked trigger digit is more likely to be offered surgery, regardless of fellowship-training background.
An evidence-based decision about an optimal treatment algorithm for management of patients with PTT is complicated by the discrepancy in outcome studies, particularly regarding those managed nonoperatively. Baek et al 2 found resolution of PTT in 63% of patients at 48 months and 75.9% at 87 months of follow-up with observation alone. Similarly, Koh et al 15 followed up PTT with locked thumbs and found 92% resolved with night-time splinting and 60% resolution with observation alone at 22 and 59 months, respectively. Jung et al 8 in a cohort of patients with varying degrees of trigger thumb reported successful nonoperative management in 80% of patients, although they did note residual symptoms that were well tolerated in a subset. These high rates of resolution with nonoperative management are contrasted by several other studies that found more modest results. Hutchinson et al 16 followed up 93 trigger thumbs and noted spontaneous resolution in 32% at 4.3 years, while 43% of the patients underwent surgical release at an average of 4.1 years. Yano et al 10 in a group of all comers with PTT found 59% and 43% resolution with splinting and observation, respectively, after 30 months. Dittmer et al 14 found resolution in 54% of patients initially managed conservatively, with the remainder electing to proceed with surgical release at 1.3 years.
Outcomes following operative management of PTT are relatively consistent across studies. Marek et al 11 reported resolution of PTT in 217 thumbs treated surgically, with 4 thumbs having superficial infection or dehiscence that resolved with wound care and had no long-term complications. Han et al 17 treated 31 thumbs with surgical release, noting complete resolution of symptoms and no complications at an average of 2-year follow-up. McAdams et al 13 performed A1 pulley release on 30 thumbs and observed resolution of triggering in all patients.
The overall diversity in results with nonoperative management with comparatively predictable results with surgical release makes it challenging to advise families on the optimal initial treatment of their child with PTT. Our study demonstrated that for very young patients (6 months), very few surgeons would recommend surgical treatment initially. As patients grow older (18 months and 3 years) and their PTT becomes more restrictive and potentially painful, surgeons are more likely to offer surgery. Interestingly, hand surgeons are more likely to offer initial surgical management of PTT in the 3-year-old cohort than pediatric orthopedic surgeons and surgeons with additional training in congenital hand surgery. It could be postulated that training philosophy influences provider decision-making, although it is difficult to identify the subtleties of each training background that would lead to our findings. One possibility is that hand surgeons often encounter this condition in adults and may have an inclination toward operative management.
This study was limited in its scope, given the nature of a survey-based method of data collection. It is subject to potential sampling bias, as those who have a predilection to treating pediatric hand conditions are foreseeably more interested in this topic and more likely to participate. The general case descriptions that were distributed may have lacked certain nuanced data that contribute to the treatment decision, such as the level of discomfort, parent and patient preference, and time of trigger thumb onset. In particular, shared decision-making with the parent in the treatment of pediatric conditions is instrumental and would directly affect management in the clinical setting. Some providers did not answer every question in the survey, which may have affected the findings.
Supplemental Material
sj-docx-1-han-10.1177_15589447231210925 – Supplemental material for Treatment Trends in Pediatric Trigger Thumb Among Hand Surgeons, Pediatric Orthopedic Surgeons, and Pediatric Hand Surgeons
Supplemental material, sj-docx-1-han-10.1177_15589447231210925 for Treatment Trends in Pediatric Trigger Thumb Among Hand Surgeons, Pediatric Orthopedic Surgeons, and Pediatric Hand Surgeons by Ashley E. MacConnell, Theodore L. Schoenfeldt, Christine A. Bowman, Alicia M. January and Felicity G. Fishman in HAND
Footnotes
Acknowledgements
The authors thank the American Society for Surgery of the Hand, American Association for Hand Surgery, and Pediatric Orthopaedic Society of North America.
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies performed on human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.