
Abstract
Background:
The Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) is a validated, static hand and upper extremity patient-reported outcome measure (PROM) commonly used. However, with the growth of PROM implementation across orthopedic and plastic surgery clinics, it is beneficial to determine whether a more general PROM can be used to capture the same insights. This would ease implementation broadly. There is a paucity of literature assessing whether the QuickDASH and Patient-Reported Outcomes Measurement Information System (PROMIS) Global-10 are correlated and perform similarly.
Methods:
Between June 2016 and December 2020, hand and upper extremity patients seeking care at clinics associated with a single quaternary academic medical center were identified. Those who completed the PROMIS Global-10 and QuickDASH as part of routine care were identified. The PROMIS Global-10 is divided into the PROMIS Global Physical Health and PROMIS Global Mental Health subscores. Spearman rho (ρ) correlations were calculated across PROMs, and ceiling and floor effects were determined.
Results:
Across the 18 744 included patients, there was a strong correlation and strong-moderate correlation found between the QuickDASH and PROMIS Global Physical Health (ρ = 0.70, P < .001) and PROMIS Global Mental Health (ρ = 0.69, P < .001), respectively. Although small, QuickDASH demonstrates the worst floor effect (2.6%, [n = 478]), whereas PROMIS Global Mental Health demonstrated a much more notable ceiling effect (11%, [n = 2034]).
Conclusions:
The PROMIS Global-10 can be used to assess the functional status of patients presenting for hand and upper extremity concerns, while also capturing aspects of mental health. The PROMIS Global-10 may ease PROM implementation broadly.
Keywords
Introduction
Health care transformation efforts remain a focus of many stakeholders, with the goal of developing a more sustainable care delivery system that rewards value, or clinical outcomes per dollar spent. 1 This effort is occurring in hand surgery and at the subspecialty level in orthopedics. 2 A major part of this movement requires measuring and assessing outcomes that are important to patients. This is currently accomplished with validated patient-reported outcome measures (PROMs), which are surveys designed to capture symptoms such as function, pain, and depression, among others. PROMs may not only be able to improve shared clinical decision-making and predict who may or may not benefit from a certain intervention, 3 but early research suggests they may improve the patient experience for certain populations too. 4
Many PROMs exist within hand surgery. 5 Across orthopedic surgery, the Patient-Reported Outcomes Measurement Information System (PROMIS) questionnaires are attractive due to their generalizability. 6 This has led to a rise in the amount of scholarly work in hand surgery focused on assessing PROMIS,7,8 as well as comparing PROMIS domains to legacy upper extremity PROMs.9 -11 Among legacy upper extremity PROMs, the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) 12 is commonly used. Early research comparing PROMIS with QuickDASH found the PROMIS Upper Extremity (UE) computerized adaptive test (CAT) v1.2 was strongly correlated with the QuickDASH. 13 In contrast, the PROMIS Global Physical Health subscale and initial version of the PROMIS Physical Function (PF) CAT were only moderately correlated with the QuickDASH, respectively.14,15 The prior study assessing the relationship between the PROMIS Global Physical Health, however, had a relatively small sample size (n = 112) and incorporated patients seen at both new patient visits and follow-up appointments. 14
Because there continues to be a growing interest in using PROMs in hand and upper extremity care and the PROMIS Global-10 remains a single easy-to-use, static form that can be easily implemented across a variety of surgical and nonsurgical subspecialties in the setting of technology limitations, it behooves us to confirm prior findings in a larger sample. Thus, across a large, multiyear sample of hand and upper extremity patients, we aim to: (1) assess the correlation between the 2 subscores (ie, PROMIS Global Physical Health and PROMIS Global Mental Health) of the commonly used PROMIS Global Health-10 and the QuickDASH; (2) assess the correlation between PROMIS Global Physical Health and PROMIS Global Mental Health subscores; and (3) determine the ceiling and floor effects of each PROM.
Materials and Methods
This retrospective observational study was approved by the appropriate institutional review board.
Between June 2016 and December 2020, all hand and upper extremity patients seeking care at clinics affiliated with a single, quaternary referral academic medical center were identified. As a part of routine clinical care at our institution, PROMs are collected electronically; however, over the study timeframe, different PROMs at different clinic sites were added and/or removed over time in an effort to try to optimize care. This led to an unexpected, yet valuable natural study environment in which patients may have completed both PROMs at the same encounter: QuickDASH and the PROMIS Global Health, with its PROMIS Global Physical Health and PROMIS Global Mental Health subscores. None of the collected PROMs were CATs. The PROMIS Global-10 includes 10 items, while the QuickDASH contains 11 items. In this study, only patients who completed both these PROMs were included. The following patient characteristics were also assessed: age (in years), sex (men or women), self-reported race (White, Asian, Black, or other), primary language (non-English or English), marital status (married, single, divorced, widowed, or other), and payor (commercial, Medicaid, Medicare, workers’ compensation, or other).
Across patient sociodemographic characteristics and PROM scores, descriptive statistics were calculated. Spearman rho (ρ) correlations were calculated between the QuickDASH and each included PROMIS domain. The absolute value of the correlations was used to focus on correlation strength. All calculated correlations were grouped as strong (≥0.7), strong-moderate (0.61-0.69), moderate (0.4-0.6), moderate-poor (0.31-0.39), or poor (≤0.3). 16 By determining the number of patients who scored the highest or lowest score of each PROM, ceiling and floor effects were calculated.
Results
A total of 18 744 patients were included in this study. The mean age was 53 years (SD: 17 years), and just more than half of the sample were women (52% [9775 of 18 744 patients]) (Table 1). Commercial insurance was the most common payor (62% [11 676 of 18 744 patients]) and a majority of included patients were of self-reported white race (81% [15 134 of 18 744 patients]). The mean QuickDASH, PROMIS Global Physical Health, and PROMIS Global Mental Health scores were 38 (SD: 24; range, 0-100), 46.5 (SD: 8.6; range, 16.2-67.7), and 51.6 (SD: 9.7; range, 21.2-67.6), respectively.
Patient Characteristics (n = 18 744).
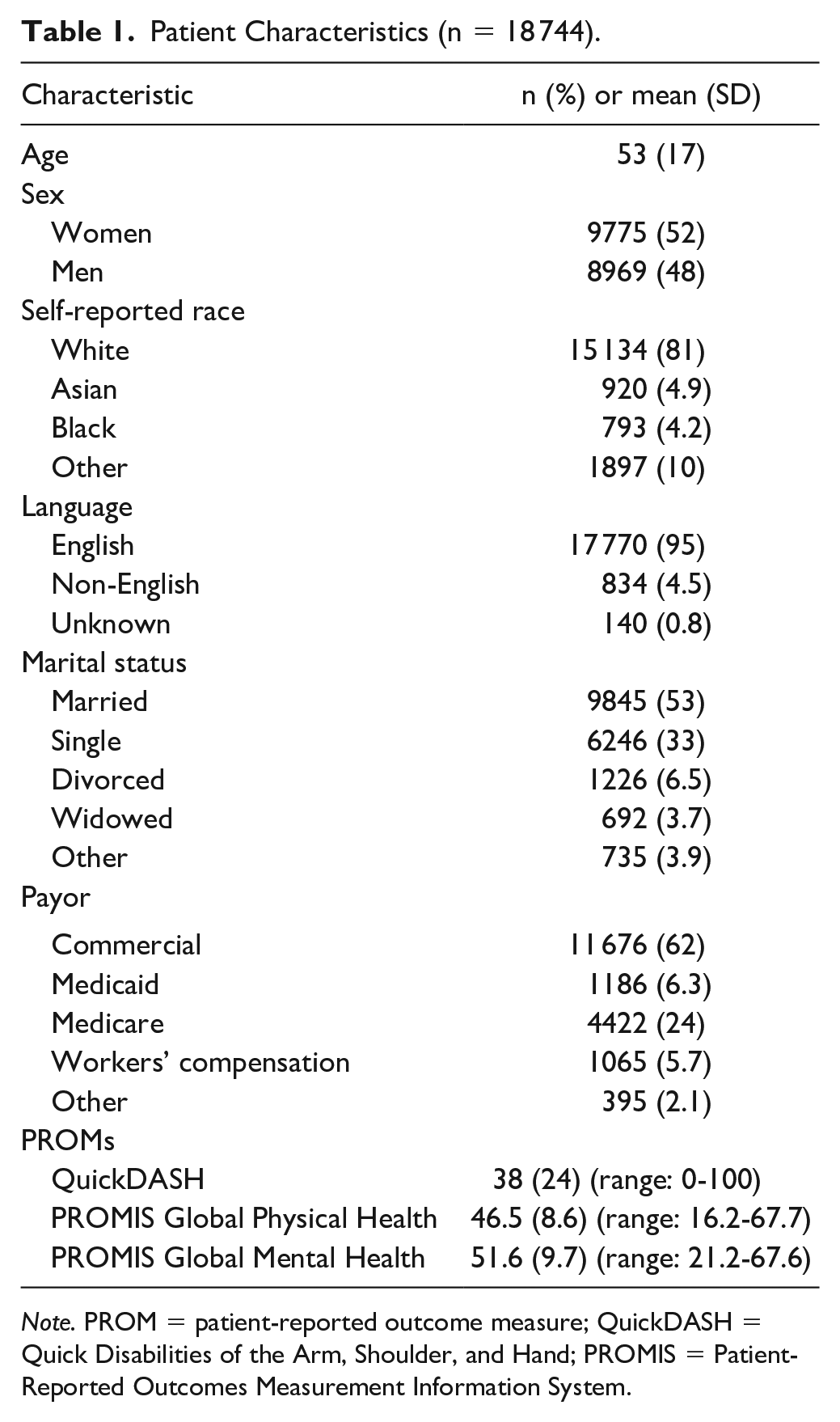
Note. PROM = patient-reported outcome measure; QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand; PROMIS = Patient-Reported Outcomes Measurement Information System.
There was a strong correlation found between the QuickDASH and PROMIS Global Physical Health (ρ = 0.70, P < .001) (Table 2). A strong-moderate correlation was found between the PROMIS Global Physical Health and PROMIS Global Mental Health (ρ = 0.69, P < .001). A moderate correlation was appreciated between QuickDASH and PROMIS Global Mental Health (ρ = 0.43, P < .001).
Spearman (ρ) Correlation Coefficients (n = 18 744). a
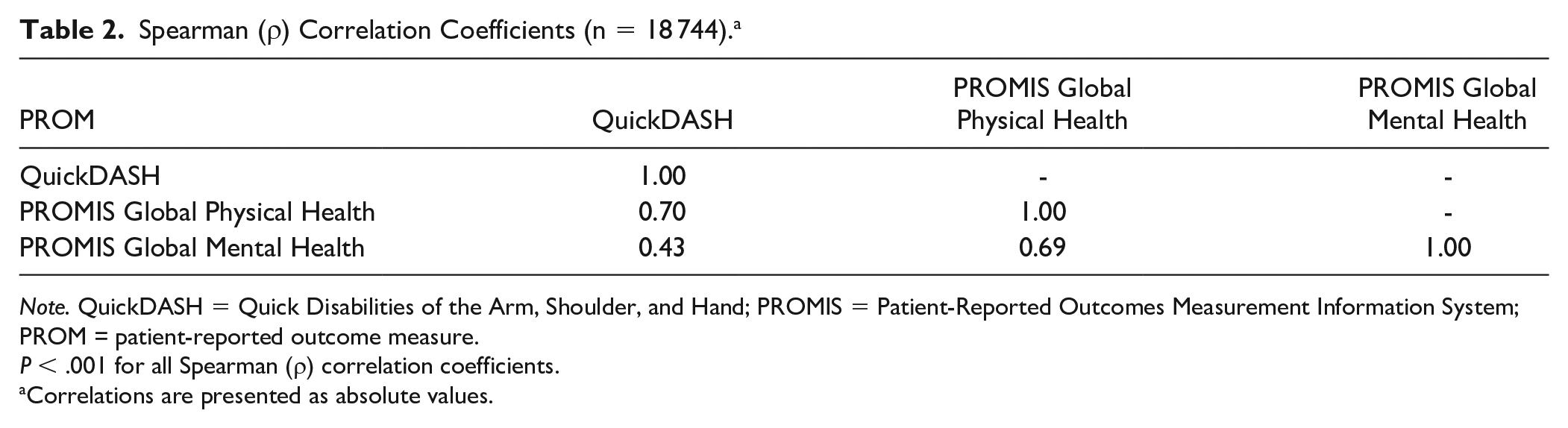
Note. QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand; PROMIS = Patient-Reported Outcomes Measurement Information System; PROM = patient-reported outcome measure.
P < .001 for all Spearman (ρ) correlation coefficients.
Correlations are presented as absolute values.
The QuickDASH demonstrated a small floor effect (2.6%, [n = 478]), whereas PROMIS Global Physical Health (0.06%, [n = 11]) and PROMIS Global Mental Health (0.3%, [n = 58]) did not (Table 3). In contrast, the QuickDASH did not demonstrate an appreciable ceiling effect (0.2%, [n = 30]). PROMIS Global Physical Health demonstrated a small ceiling effect (1.7%, [= 319]), whereas PROMIS Global Mental Health demonstrated a much more notable ceiling effect (11%, [n = 2034]).
Evaluation of Ceiling and Floor Effects by PROM (n = 18 744).
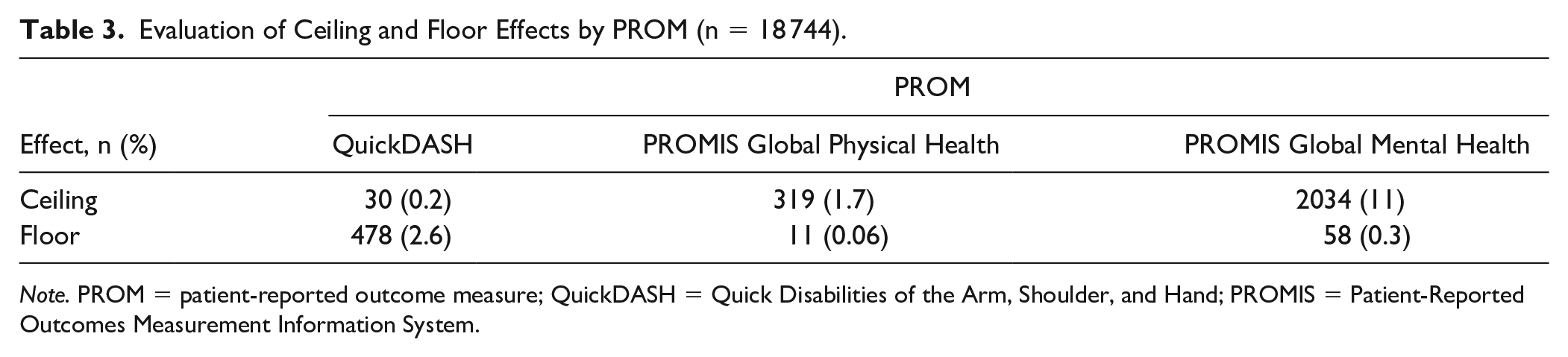
Note. PROM = patient-reported outcome measure; QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand; PROMIS = Patient-Reported Outcomes Measurement Information System.
Discussion
In this study, we assessed whether PROMIS Global-10 (and its 2 subscores—Physical Health and Mental Health) captured a similar construct to the QuickDASH and evaluated the performance (ie, ceiling and floor effects) of each PROM across a large hand and upper extremity patient sample. We found a strong correlation between the QuickDASH and PROMIS Global Physical Health subscore, with similar performance between the 2 measures as well. The PROMIS Global Mental Health subscore was moderately correlated to the QuickDASH, suggesting different constructs are likely being measured. Our findings suggest that the PROMIS Global-10 is a reasonable PROM in hand and upper extremity clinic settings, and it may also provide added mental health insight not captured by the QuickDASH as well.
Our work builds on a prior study demonstrating a substantial correlation between the PROMIS Global-10 and QuickDASH. For example, Stoop et al 14 found that QuickDASH and PROMIS Global Physical Health subscale were significantly correlated, but only moderately so. However, in contrast to our work, this study only incorporated 112 patients, of which less than half were new patients and nearly one-quarter had already had surgery. In this study, we included nearly 19 000 patient encounters, which we believe provides a more robust assessment of the potential value of the PROMIS Global-10 and its Physical Health subscale across a large, diverse patient sample.
Unlike prior research that showed no significant correlation between QuickDASH and the PROMIS Global Mental Health subscale, 14 we found a moderate correlation. Furthermore, we discovered a moderate-strong correlation existed between the PROMIS Global Mental Health and PROMIS Global Physical Health subscales. Our findings are more consistent with the literature, which shows moderate correlations exist between mental health measures (eg, depression) and functional measures in hand and upper extremity patients. 17 In addition, this finding makes sense, given our growing understanding of how mental health, including depression, can explain a great deal of the variation in functional well-being among hand and upper extremity patients. 18 While significant correlations exist, the strength of these correlations confirms that these measures assess different constructs. We believe both (ie, physical and mental health) are equally important to assess.
The low ceiling and floor effects seen in our sample by the QuickDASH and PROMIS Global Physical Health subscale suggest that these instruments can differentiate patient functional status even at the extremes. However, the PROMIS Global Mental Health subscale demonstrated a substantial ceiling effect (11%) in our sample, meaning that patients in this group report the “best” mental health status possible. Unfortunately, this is a phenomenon well documented in the orthopedic surgery literature for mental health-related PROMs.19,20 One hypothesis of this finding is that patients do not fully appreciate why they are being asked to share their mental health symptoms in a hand and upper extremity setting. However, because of the importance of mental health on physical well-being, it is crucial to stress to patients the value of accurately completing the mental health PROMs while in a musculoskeletal clinic setting.
Our findings should be examined keeping our study’s limitations in mind. First, all patients came from a single, quaternary referral academic medical center. Furthermore, while some patient sociodemographic factors are quite diverse across the sample, others—such as self-reported race—are not, with just more than 80% self-reporting as White. These issues may limit generalizability of our findings; however, our large sample and consistency in findings with what is reported in the literature to date using smaller samples support the value of our work. Second, we included all patients regardless of diagnosis. Therefore, we cannot comment as to whether the relationship between the studied PROMs would differ in other patient samples (eg, when broken down by diagnosis). However, because our work still focused on the relationship of the PROMs at a single moment and did not assess changes in PROMs over time (eg, in response to a given treatment), we believe our findings would be unlikely to change dramatically. Nonetheless, future work can seek to assess our assumption. Third, we only included patients who completed both the PROMIS Global-10 and QuickDASH. Because our PROMs implementation process across our institution shifted over the study timeframe, it is not possible to determine accurately which patients were offered both PROMs; thus, we cannot assess which patients are nonresponders. While this may introduce an element of selection bias, we believe that because—as noted above—we are assessing PROMs at a single point in time (and not the response of PROMs to any intervention), the impact—if any—is minimal and would not affect our main findings. Finally, this work does not assess which PROMIS questionnaire (or set of questionnaires) is best in the hand and upper extremity patient population; instead, it highlights that a general, static PROM (ie, PROMIS Global-10) can be substituted appropriately for a hand and upper extremity-specific, static PROM (ie, QuickDASH). Future work can compare the PROMIS Global-10 with other PROMIS measures, such as PROMIS UE or PROMIS PF static forms or CATs.
Overall, in a very large sample of hand and upper extremity patients, we found that the QuickDASH and PROMIS Global Physical Health subscale were strongly correlated and demonstrated similar ceiling and floor effects. In addition, the PROMIS Global Mental Health subscale was significantly correlated with both functional scales but to a lesser degree. The PROMIS Global Mental Health subscale also demonstrated a notable ceiling effect (ie, measurable number of patients achieving the “best” possible score). These findings suggest that the PROMIS Global-10 can be used to assess the functional status of patients presenting for hand and upper extremity concerns, while also capturing aspects of mental health. Because the PROMIS Global-10 can be used in such a patient population, its use may help simplify PROM collection in broad clinical settings across multiple orthopedic subspecialties and/or hospital settings. However, future research should assess the ability of PROMIS Global-10 to detect change and predict outcomes following treatment or intervention for common hand and upper extremity conditions.
Footnotes
Author Contributions
D.N.B. and D.G.T. researched the literature and were involved in protocol development and study plan. All authors helped conceive the study. D.N.B., C.V.B., and D.G.T. were involved in data extraction, cleaning, and analysis. D.N.B. and C.V.B. were involved in writing the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript. All authors confirmed accuracy.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
This was a retrospective review of data collected as part of routine clinical care; thus, we were not required per our institutional review board to obtain individual informed consent for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.N.B. received research grant funding from the American Orthopaedic Foot & Ankle Society, American Foundation for Surgery of the Hand (unrelated to this study), and Cervical Spine Research Society and personal fees from the Institute for Strategy and Competitiveness at Harvard Business School, COSF/Boston Children’s Hospital, Mass General Brigham, CAPADEV, The Heritage Foundation, National Academy of Medicine (NAM), and Spine (Social Media Editor), outside of the submitted work. Each of the other coauthors (C.V.B., J.L., R.G., A.R.B., and D.G.T.) certify that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.