
Abstract
Background:
The annual volume of carpal tunnel release (CTR) in the United States has been estimated to be 577 000 per year. Our objectives were to evaluate the incidence and risk factors for revision CTR within 1 year of primary CTR.
Methods:
We identified all adult patients undergoing primary CTR from October 2015 to September 2019 in the New York Statewide Planning and Research Cooperative System database using Current Procedural Terminology (CPT) codes. We used the CPT modifier codes to determine laterality of index and revision procedures. We estimated multivariable hierarchical logistic regression models to evaluate risk factors for revision CTR within 1 year.
Results:
Of the 80 423 primary CTR procedures, 178 (0.22%) underwent a revision CTR within 1 year of the index surgery. The mean (SD) age of the entire cohort was 58.69 (14.43) years, 61.1% were women, 73.2% were non-Hispanic white, 42.9% were covered through private insurance, and 9.5% had diabetes mellitus. Workers’ compensation insurance (odds ratio [OR] = 1.83, 95% confidence interval [CI], 1.13-2.98, P = .02) and simultaneous bilateral CTR (OR = 14.91, 95% CI, 9.62-23.12, P < .001) were associated with revision CTR within 1 year of the index procedure. No models demonstrated an association between endoscopic technique or surgeon volume and revision CTR.
Conclusions:
The incidence of revision CTR within 1 year was lower than that previously reported. Patients covered by workers’ compensation and those undergoing simultaneous bilateral CTR had higher likelihood of a revision CTR within 1 year, whereas endoscopic technique and surgeon volume were not associated with revision CTR within 1 year.
Keywords
Introduction
Carpal tunnel syndrome is a common condition, with an annual incidence of 2 to 3 cases per 1000 individuals.1,2 Surgical treatment consisting of release of the transverse carpal ligament is indicated in the setting of advanced disease or persistent symptoms after nonoperative treatment. Carpal tunnel release (CTR) may be performed by hand fellowship-trained orthopedic, plastic, or general surgeons, as well as general orthopedic surgeons, general plastic surgeons, and neurosurgeons.
The annual volume of CTR in the United States has been estimated to be 577 000 per year, 3 and lifetime incidence of CTR has been estimated at 3.1%. 4 A total of 7% to 20% of patients may experience either recurrent symptoms after a period of relief following a technically successful procedure or persistent symptoms throughout the recovery period. 5 Patients may undergo revision CTR in these situations.
The previously reported incidence of revision CTR after index CTR was 1.5% in a single-institution study at a median follow-up of 4.8 years 6 and 3.4% in a study of patients undergoing CTR in England at a median follow-up of 7.5 years. 7 The latter study did not evaluate the association of surgical approach with revision CTR. A recent study that examined revision rates reported an overall incidence of revision CTR within 1 year of 4.8% and that endoscopic technique was associated with 1.3 times increased odds of revision surgery within 1 year. 8 However, the data source used in this study only included patients with private insurance, limiting its generalizability. In addition, prior studies have not controlled for surgeon factors such as surgical volume or specialty which may be associated with revision CTR.
Thus, previous studies have been single-center studies, focused on private insurance patients, or did not evaluate the effect of endoscopic approach. Hence, little is known about the overall risk of revision CTR, and the determinants of revision among the general population. The objective of this study was to evaluate the incidence of revision CTR within 1 year of the index surgery (primary CTR), and its association with patient and surgeon factors in a large cohort of patients with multiple payers in a large geographic area. Our hypothesis was surgeon training and endoscopic technique would be more likely to result in revision carpal tunnel surgery.
Materials and Methods
Data Sources and Study Cohort
We used the 2015 to 2020 outpatient and ambulatory surgery files from the New York Statewide Planning and Research Cooperative System (SPARCS) database for our study. The SPARCS database is a deidentified comprehensive all-payer data-reporting system that collects encounter-level data on patient characteristics, diagnoses and treatment, services and charges for inpatient hospital admissions, ambulatory surgery, emergency department visits, and other outpatient data from New York State. The Statewide Planning and Research Cooperative System has been previously used to examine outcomes after hand surgery including upper extremity amputation and flexor pulley reconstruction.9,10
We included all patients aged 18 years and older undergoing CTR in New York State from October 1, 2015, to September 31, 2019, using Current Procedural Terminology (CPT) codes to identify procedures which are listed in Table 1. We used CPT modifier codes to determine the laterality of the index CTR. We defined simultaneous bilateral CTR as an encounter for CTR with a modifier code of 50 indicating bilateral surgery or CPT modifier codes indicating laterality as both left and right at the same encounter. Staged bilateral CTR was defined as 2 separate unilateral CTR procedures with differing laterality within 42 days, a time interval previously used to identify planned staged procedures. 11 We linked the physician license number in the SPARCS database to the National Plan and Provider Enumeration System database 12 to obtain the National Provider Identifier (NPI). The NPI was then used to link the SPARCS observations with the American Society for Surgery of the Hand (ASSH) membership directory for identifying hand surgeons 13 and the Physician Compare database 14 for identifying surgeon covariates and primary specialty among non-hand surgeons.
CPT Codes Used to Identify Procedures.
Note. CPT = Current Procedural Terminology.
We initially identified 105 102 CTR procedures during the period of interest. We excluded any patient with a prior CTR within the past 4 years (n = 2102), no surgeon identifier (n = 12 714), no diagnosis code for carpal tunnel syndrome (n = 1134), no laterality for index procedure (n = 7617), a diagnosis of compartment syndrome or concomitant procedure code for distal radius fracture fixation (n = 1061), or for patients younger than 18 years (51). Our final cohort consisted of 80 423 primary CTRs performed on 69 903 patients. We used the 2011 to 2014 files in addition to the 2015 to 2019 files from SPARCS to identify concomitant procedures within 4 years prior to the primary CTR. The flowchart for patient selection is shown in Supplemental Figure S1.
Outcome Variables
The primary outcome was revision CTR within 1 year after the index procedure. We considered any encounter with a procedure code for endoscopic or open CTR and procedure code modifier indicating the same laterality or bilateral surgery after the primary CTR to represent revision carpal tunnel surgery. For patients undergoing bilateral CTR at the time of the index procedure, any future procedure with an identified laterality during the study period was considered a revision procedure. We required future procedures following index bilateral CTR to have a recorded laterality so as not to bias our findings toward a higher rate of revision surgery with bilateral CTR.
Patient Covariates
We used the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes to identify encounters for carpal tunnel syndrome (G56.00, G56.01, G56.02, and G56.03). We also used ICD-10-CM codes to identify a concomitant diagnosis code for upper extremity compartment syndrome (M79A1 and T79A1), and medical comorbidities. We identified diagnosis of compartment syndrome to exclude cases of CTR associated with this as this is a different procedure than elective CTR. We used the Healthcare Cost and Utilization Project Clinical Classifications Software Refined list of diagnosis codes 15 to define medical comorbidities present at the time of the index procedure based on previous work.8,16 These comorbidities included rheumatoid arthritis, gout, systemic lupus erythematosus, diabetes mellitus, thyroid disease, tobacco use, psychiatric disease (defined as presence of a diagnosis code for depression, anxiety, or bipolar disorder), and spondylopathies/spondyloarthropathy.
To test the association of revision CTR with patient factors, we used the following patient-level variables: a categorical indicator for patient age (whether the patient was aged 65 years or older), and categorical indicators for patient race and ethnicity (non-Hispanic black, Hispanic, non-Hispanic white, or Other), sex (male or female), medical comorbidities listed above, whether the patient underwent bilateral CTR (unilateral, simultaneous bilateral, or staged bilateral), insurance type (private, Medicare, Medicaid, workers’ compensation, or other), endoscopic or open approach, whether the patient underwent concomitant cubital tunnel release, and whether the patient underwent other concomitant hand or wrist procedures (surgical treatment of thumb carpometacarpal arthritis, trigger finger release, or extensor tendon release).
Surgeon Covariates
We also controlled for the following surgeon-level variables because these may partially explain the variation in the outcome: categorical indicators for annual volume of CTR surgeries classified into quartiles, percentage of CTR procedures performed with endoscopic approach for a given surgeon in a given year, and specialty (hand, general orthopedic, general plastic, or neurosurgeon). General orthopedic and plastic surgeons were defined as non-hand orthopedic and plastic surgeons, respectively. Membership in the ASSH was considered a proxy for hand fellowship completion and was used to identify hand surgeons because membership requires successful completion of the Subspecialty Certificate in Surgery of the Hand. 17
Statistical Analysis
We first computed the incidence of revision CTR within 1 year of the index CTR. We used the χ2 and Mann Whitney U test to evaluate unadjusted differences in the key characteristics between the patients who did and did not undergo revision CTR. We evaluated the association of key patient and surgeon factors with the likelihood of undergoing revision CTR. The multivariable model controlled for patient- and surgeon-level covariates as well as random effects for facility to account for clustering of observations within facilities. We assessed for multicollinearity with the variance inflation factor and confirmed a value of less than 5 for all variables. A 2-tailed P value of less than .05 was considered statistically significant.
Sensitivity Analysis
Several sensitivity analyses were conducted. First, we reevaluated the risk factors of interest with the outcome of revision CTR within 3 years of the index surgery, a time point previously used to evaluate outcomes after a different upper extremity compressive neuropathy. 18 For this analysis, we evaluated patients undergoing primary CTR between October 2015 and September 2017. 18 Second, we repeated the analysis with hand surgeon defined by specialty entered in the Physician Compare data set instead from the ASSH membership directory. Third, we repeated the analysis with a more inclusive definition of revision CTR to include any repeat ipsilateral CTR or any repeat CTR with missing laterality.
Ethical Approval
The study was approved by our institutional review board.
Results
Unadjusted Analysis
Of the 80 423 primary CTR procedures, 178 (0.22%) underwent a revision surgery within 1 year of the index surgery (Table 2). The median time of revision CTR within 1 year was 96 days (interquartile range = 43-186 days). The mean (SD) age of the entire cohort overall was 58.7 (14.4) years, 61.1% were women, 73.2% were non-Hispanic white, 42.9% were covered through private insurance, 9.5% had diabetes mellitus, and 36.3% underwent endoscopic CTR. In year 1 (October 2015-September 2016), the median number of CTR procedures per surgeon was 8 (interquartile range = 2-31). Endoscopic approach was not associated with revision surgery at 1 year on bivariate analysis (P = .49). Compared with CTR cases that did not undergo revision, cases that underwent revision did not have a different distribution of insurance type (P = .25) but had a higher proportion of simultaneous bilateral procedures (P < .001). There were no significant differences in other patient or surgeon factors between the 2 groups.
Descriptive Statistics for Patients Who Did Versus Did Not Undergo Revision Carpal Tunnel Release Within 1 Year After the Index Procedure.
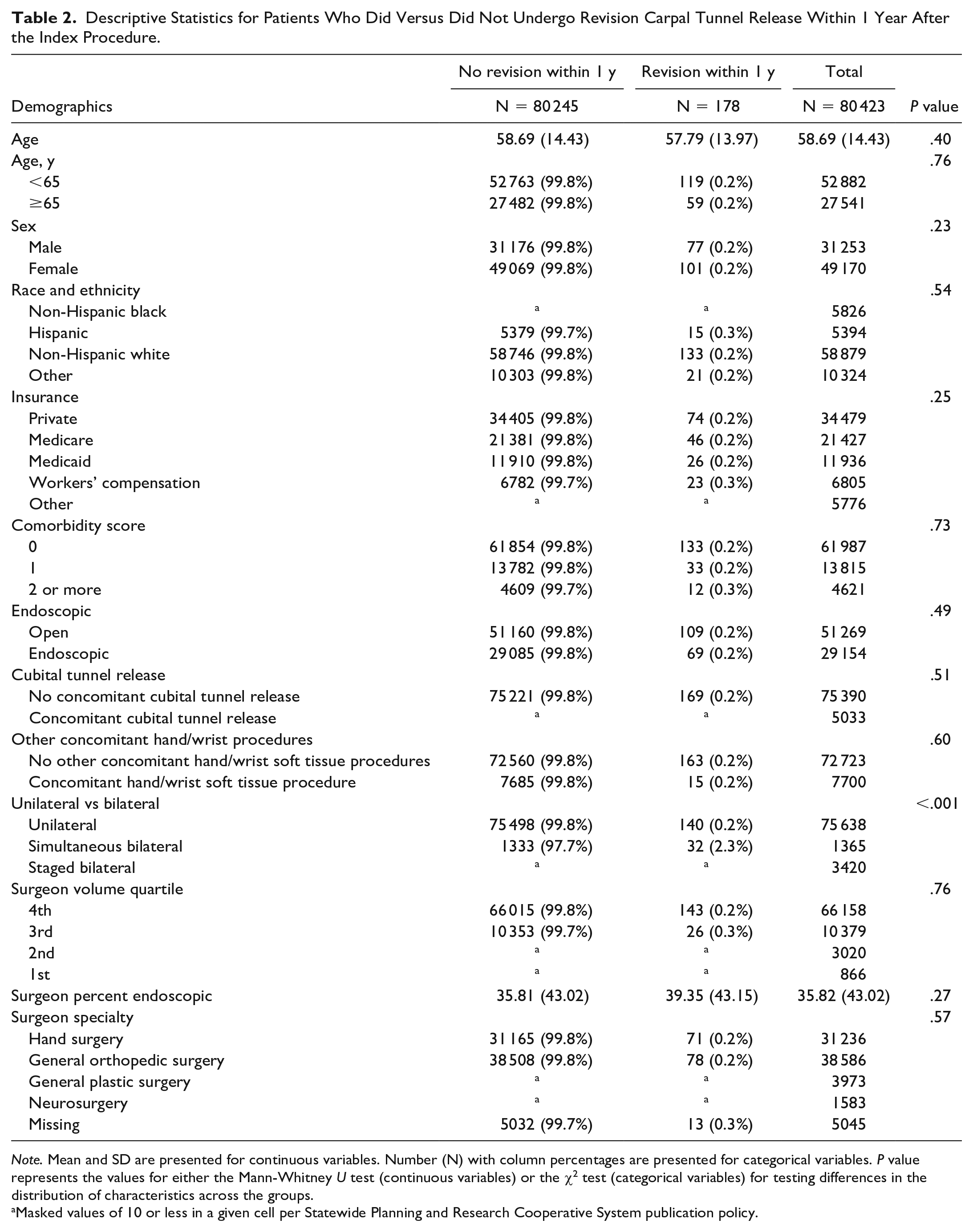
Note. Mean and SD are presented for continuous variables. Number (N) with column percentages are presented for categorical variables. P value represents the values for either the Mann-Whitney U test (continuous variables) or the χ2 test (categorical variables) for testing differences in the distribution of characteristics across the groups.
Masked values of 10 or less in a given cell per Statewide Planning and Research Cooperative System publication policy.
Multivariable Analysis
The results of the multivariable analysis are shown in Table 3. After controlling for patient- and surgeon-level covariates, as well as facility random effects, and compared with their respective baseline counterparts, the odds for revision CTR within 1 year were 83% higher for patients with workers’ compensation insurance (odds ratio [OR] = 1.83, 95% confidence interval [CI], 1.13-2.98, P = .02), 1.391% higher for patients undergoing simultaneous bilateral primary CTR (OR = 14.91, 95% CI, 9.62-23.12, P < .001). We found no association of endoscopic surgical technique, concomitant procedures, surgeon volume, or surgeon specialty with revision CTR.
Results of Model Evaluating Odds of Undergoing Revision Carpal Tunnel Release Within 1 Year of Index Carpal Tunnel Release.
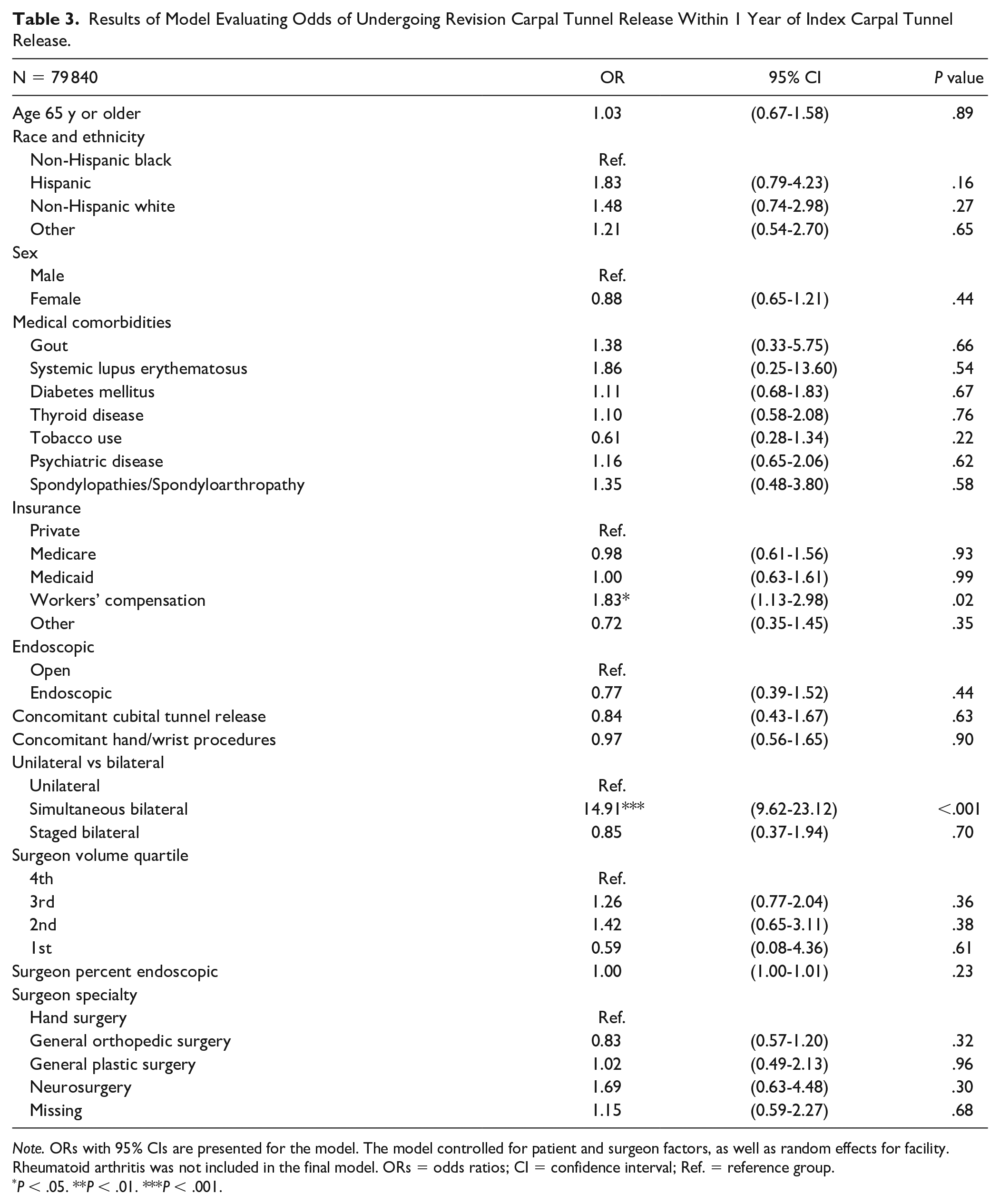
Note. ORs with 95% CIs are presented for the model. The model controlled for patient and surgeon factors, as well as random effects for facility. Rheumatoid arthritis was not included in the final model. ORs = odds ratios; CI = confidence interval; Ref. = reference group.
P < .05. **P < .01. ***P < .001.
Sensitivity Analysis
We found that 153 of 34 042 (0.45%) cases went on to revision CTR within 3 years. The results of the multivariable sensitivity analyses were generally consistent with the main findings (Supplemental Tables S1-S3). Notably, spondylopathies/spondyloarthropathy were also associated with revision CTR within 3 years (Supplemental Table S1). After adjusting the definition of revision CTR to include repeat ipsilateral CTR and repeat CTR with missing laterality, the more inclusive estimate of the incidence of revision CTR within 1 year was 0.47%; staged bilateral CTR was associated with lower odds of revision CTR when revision CTR was defined using the more inclusive definition of revision CTR.
Discussion
We found that the incidence of revision CTR within 1 year of primary CTR was 0.22%. The risk of revision CTR within 1 year was higher for those with workers’ compensation insurance and simultaneous bilateral CTR. We found no association between revision CTR and endoscopic technique, surgeon specialty, or surgeon volume in patients undergoing CTR in New York State in our main analysis. The strengths of this study also include the modeling of surgeon and facility effects and defining procedure laterality based on procedure modifier codes rather than on diagnosis codes.
Westenberg et al manually reviewed patient medical records of patients from a single institution and found an incidence of revision CTR of 1.5% at median follow-up of 4.8 years. Wessel et al 8 reported an incidence of revision surgery of 4.8% at 1 year. They defined revision CTR as repeat procedure code for CTR and used diagnosis codes to confirm laterality. We speculate that our use of procedure modifier codes to be a more reliable indicator of laterality than diagnosis codes as procedure modifier codes is linked to claims processing 19 and therefore reimbursement. 8 We were not able to identify any studies comparing the accuracy of laterality identified using diagnosis versus procedure codes. In addition, we cannot rule out regional differences in patient populations or practice patterns contributing to the differences between our study and the prior literature. It is unclear why there was such a difference in the findings between the studies, particularly given they were both from large administrative databases, but clearly differences exist. Notably, there were differences in insurances with Wessel et al 8 reporting on predominantly patients with private insurance and the SPARCS database being more reflective of the population of New York (Table 4).
Insurance Distribution and Incidence of Revision CTR in This Study and Prior Studies.
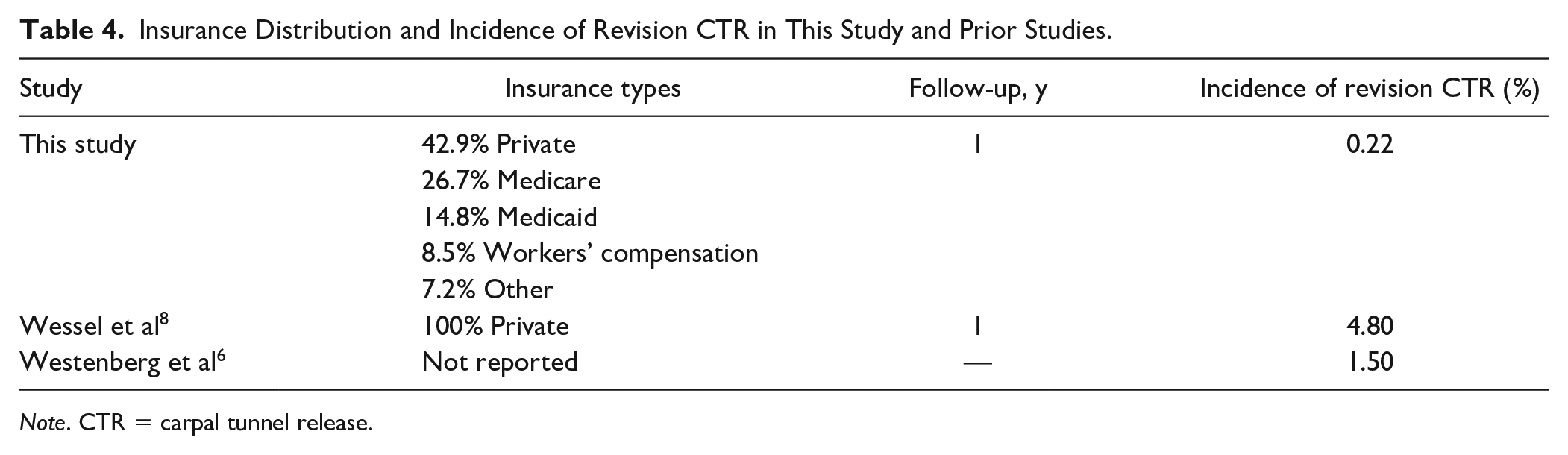
Note. CTR = carpal tunnel release.
We found no association between endoscopic technique and revision CTR. Agee et al 21 reported 2 cases of revision CTR after endoscopic CTR and zero cases of revision CTR after open CTR in a randomized trial involving 122 patients. Williamson et al 22 found no difference in complications after endoscopic versus open CTR in an analysis of multiple state ambulatory surgery databases. Our findings are in contrast to the findings reported by Wessel et al 8 and Westenberg et al 6 who reported that endoscopic technique was associated with revision CTR (OR = 1.3 and 2.3, respectively). The reason for this finding is unclear. We suspect that this may be partially due to the difference in coding used to define revision CTR between the prior literature and this study. In addition, these prior studies did not account for the effects of surgeon or facility where the procedure was performed. We did find lower revision rates for general orthopedic surgeons. We speculate this is because our data track patients and a general orthopedic surgeon may be less likely to see the more advanced or complex cases, or refer to a specialists in the case of persistent symptoms following surgery.
There are limited data on the relationship of insurance and outcomes after CTR. Sun Cao et al 23 found that Medicaid and private insurance were associated with increased complications relative to Medicare in patients undergoing CTR. Less than half of the patients in our study had private insurance, which suggests that the overall complication rate of 2.23% reported by Sun Cao et al may be an overestimation. Westenberg et al 6 found that workers’ compensation insurance was not associated with revision CTR. However, the study by Westenberg et al evaluated insurance as a binary variable (workers’ compensation vs any other insurance type) and also included a smaller cohort of patients (7464) at a single institution. Workers’ compensation typically requires electrodiagnostic studies to approve CTR surgery and it is possible patients with diagnosis of Carpal Tunnel Syndrome (CTS) on nerve studies do not correlate with clinical symptoms, and thus, incomplete relief of symptoms or those with other issues related to their workers’ compensation claim lead to higher revision rates.
Similar to the findings reported by Westenberg et al, 6 we found a strong association between bilateral primary CTR and future revision CTR. While patients with bilateral CTR may have systemic conditions that may predispose patients to recurrent or persistent symptoms, we did not find an association between staged bilateral CTR and future revision surgery. Most patients undergoing bilateral CTR in the study by Westenberg et al underwent staged (timing unknown) rather than simultaneous CTR, limiting the conclusions that could be drawn regarding the association between timing of bilateral CTR and outcomes in that study. We speculate that this finding may be due to errors in coding, as any patient who was erroneously coded as having simultaneous bilateral CTR would have any subsequent contralateral CTR procedure mislabeled as a revision surgery.
In addition, we did not find any association of medical comorbidities with revision CTR in the main analysis. This is in contrast to the findings reported by Westenberg et al 6 who reported an association of rheumatoid arthritis and smoking with revision CTR on multivariable analysis. We also reported relatively low prevalence of these comorbidities in our cohort. It may be that these comorbidities are not consistently recorded during encounters for outpatient surgery in databases derived from billing records and that an association may be seen if we were able to review full clinical histories from the included patients. Future work may seek to further investigate the association of medical comorbidities with revision CTR.
While a relationship between high surgeon or facility volume and superior outcomes has been demonstrated in a number of areas in orthopedic and hand surgery,20,24 -26 we did not observe such a relationship in this study, and the overall median annual number of CTR surgeries per surgeon performed (8) was lower than expected. We speculate that there may be a relationship between surgeon volume and other outcomes such as improvement in function or reduction in pain and that there may be a relationship between surgeon volume and reoperation after more complex nerve surgeries such as brachial plexus reconstruction. We also did not find that hand surgeons, defined using either ASSH membership or using the Physician Compare database, had superior outcomes of revision surgery. However, we speculate that hand surgeons may be operating on patients with more advanced disease.
Based on our findings, patients and surgeons may consider endoscopic approach is reasonable and may not have increased risk of revision CTR within 1 year. Further work should focus on differences in patients who undergo staged versus simultaneous bilateral CTR and how these differences may influence outcomes, as well as optimizing treatment protocols for patients with workers’ compensation insurance. If other patient outcomes are shown to be correlated with surgeon or facility factors, this may lead to changes in how patients choose surgeons and surgical practices if patients were made aware of these differences.
This study has several limitations. First, this was a retrospective analysis of administrative data from New York State and is dependent on reliable coding of variables. However, the geographic scope of this data set allows for evaluation of outcomes in a large cohort of patients, which increases the generalizability of the findings. In addition, CTR is more commonly performed as an office-based procedure and these patients are not captured in the SPARCS database. Second, we did not have access to data on patient symptoms that led to revision surgery, findings at the time of revision surgery, and objective findings such as electrodiagnostic studies, and we were only able to evaluate revision CTR as an outcome. Third, we limited our analysis to revision CTR within 1 and 3 years after index CTR, and it is possible that patients underwent revision CTR after that time or outside of New York State. Similarly, we excluded patients with CTR in the 4 years prior to the index CTR in attempt to identify primary CTR cases. However, it is possible that patients underwent CTR at earlier time points or during this time period outside of NY and thus were incorrectly considered to be undergoing primary CTR. Fourth, while we used a time interval for staged bilateral procedures previously reported in the literature, our definition could be excluding planned staged bilateral procedures with time intervals greater than 42 days between procedures. Fifth, we used ASSH membership to identify hand surgeons, which may result in misidentification of surgeon specialty. While there are clearly hand fellowship-trained surgeons who are not members of ASSH, we feel this number is likely small considering the study size and this misidentification would lead to highly trained surgeons being included in the general orthopedic or plastic surgeon groups and not affect our findings. In addition, our results did not change substantially when we used a different definition, the Physician Compare data set, to identify surgeon specialty. Finally, while SPARCS includes data from both hospital-affiliated and freestanding facilities, there are some facilities in the state that are not included, and some procedures performed in the office setting may not be captured. Hence, our findings can be generalized to this group of facilities only, but do not feel revision rates would be related to the type of facility in which the procedure was performed.
Conclusions
Our findings suggest that the incidence of revision CTR in New York State is lower than that previously reported in other populations, as we speculated and the reason for performing this study. We were, however, surprised to find the magnitude of difference and feel this warrants further investigation to be confident in revision rates. We did not find an independent association between endoscopic technique or surgeon specialty and revision surgery and thus rejected our hypothesis related to these variables. We found that workers’ compensation and simultaneous bilateral CTR were associated with revision CTR within 1 year. This information may help patients and surgeons better understand prognosis after CTR.
Supplemental Material
sj-docx-1-han-10.1177_15589447231211608 – Supplemental material for Incidence and Risk Factors for Revision Within 1 Year of Primary Carpal Tunnel Release
Supplemental material, sj-docx-1-han-10.1177_15589447231211608 for Incidence and Risk Factors for Revision Within 1 Year of Primary Carpal Tunnel Release by Derek T. Schloemann, Caroline P. Thirukumaran and Warren C. Hammert in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
The institutional review board granted an exemption of informed consent.
Disclaimer
This work was performed at the University of Rochester Medical Center. This publication was produced from raw data purchased from or provided by the New York State Department of Health (NYSDOH). However, the conclusions derived, and views expressed herein are those of the author(s) and do not reflect the conclusions or views of the NYSDOH. The NYSDOH, its employees, officers, and agents make no representation, warranty, or guarantee as to the accuracy, completeness, currency, or suitability of the information provided here.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no conflicts related to this work. D.T.S. reports grants from the University of Rochester and the American Foundation for Surgery of the Hand, outside the submitted work. C.P.T. reports grants from the National Institutes of Health, outside the submitted work; reports honoraria from Veterans Affairs, National Institutes of Health, Brown University, outside the submitted work; and reports serving as the Section Editor of the disparities section of Current Osteoporosis Reports and as an Assistant Editor for the disparities section of Anesthesia and Analgesia, neither of which are related to this work. W.C.H. received payment from the International Bone Research Association and is a participant on a data safety monitory board or advisory board for Sonex Health, neither of which are related to this work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.